Thoracic / Lung
2026-06-02 ASCO Annual Meeting 2026
LBA8005: Concurrent TRT + Chemoimmunotherapy in ES-SCLC
ForExtensive-stage SCLC, treatment-naive, ECOG 0-1, stable brain mets allowed
TL;DROS 10.0 vs 11.8mo, HR 1.14 (0.84-1.56), p=0.40: concurrent thoracic RT added no survival benefit to 1L chemoimmunotherapy in ES-SCLC.
Concurrent thoracic RT (30 Gy/10 fx) adds nothing to 1L chemoimmunotherapy in ES-SCLC, and the subgroups where CREST's late benefit would be expected (chemoIO completers, no brain/liver mets) were null too. But this tested concurrent-during-induction RT in an unselected population, not CREST's consolidative-to-responders design, so consolidative TRT stays an open question.
- vs CREST (Slotman, Lancet 2015): same 30Gy/10fx but consolidative in the chemo-only era; that late-OS signal does not carry into the IO era here

| Arm | Median OS | HR (95% CI) | p |
|---|---|---|---|
| ChemoIO + TRT | 10.0 mo (8.3-11.7) | 1.14 (0.84-1.56) | 0.40 |
| ChemoIO | 11.8 mo (10.0-13.6) | ref | — |
+2 more figures

| Arm | Median PFS | HR (95% CI) | p |
|---|---|---|---|
| ChemoIO + TRT | 5.1 mo (4.7-5.4) | 1.10 (0.84-1.45) | 0.49 |
| ChemoIO | 5.0 mo (4.6-5.4) | ref | — |

| Subgroup | TRT median OS | ChemoIO median OS | HR (95% CI) | p |
|---|---|---|---|---|
| Completed all 4 chemoIO courses | 11.9 mo (9.7-14.1) | 12.1 mo (9.4-14.8) | 1.02 (0.72-1.44) | 0.92 |
| No brain/liver mets | 11.9 mo (6.2-17.7) | 13.2 mo (10.4-16.1) | 1.10 (0.65-1.87) | 0.72 |
7 details 5 trials watching
- 🔍 Randomized phase III, concurrent TRT n=115 vs chemoIO alone n=113, 1° endpoint OS
- 🔍 TRT 30 Gy/10 fx given concurrently (start day 21-28, cycle 2), not as post-chemo consolidation
- 💊 Backbone: durvalumab 1500mg + carboplatin AUC5 + etoposide x4, then durvalumab maintenance to PD
- 🔍 PCI 25-30 Gy optional to responders
- 📊 Even in the subgroups most likely to benefit (chemoIO completers, no brain/liver mets), TRT showed no OS advantage
- ⚠️ Concurrent timing and an unselected (not response-enriched) population differ from CREST's design; not a clean replication
- ⚠️ Toxicity was a key secondary; no AE numbers reported in source
- Does consolidative (not concurrent) thoracic RT still benefit ES-SCLC responders in the IO era? recruiting Tislelizumab Combined With Chemotherapy Followed by Thoracic Consolidation Radiotherapy in the First-line Treatment of Extensive Stage Small Cell Lung Cancer Phase 2n=36 · primary completion 2027-12 · consolidation TRT only in induction respondersn=46 · primary completion 2027-12 · sequential TRT + durvalumab maintenance post-1Lnot yet Adebrelimab Combined with Chemotherapy and Thoracic Radiotherapy for First-line Treatment of ES-SCLC Phase 3n=524 · primary completion 2029-06 · phase 3 consolidative TRT vs IO maintenance alone
- Any role for TRT in oligometastatic or low-burden ES-SCLC subsets? not yet Durvalumab Combined With Consolidation Radiotherapy After First-line Treatment in Extensive Stage Small Cell Lung Cancer With Oligometastases Phase 2n=58 · primary completion 2024-08 · consolidation RT in 1-5 lesion oligomet ES-SCLCnot yet Tislelizumab in Combination with Chemotherapy ± Radiotherapy for Extensive-Stage Oligometastatic Small Cell Lung Cancer. Phase 2n=64 · primary completion 2027-01 · randomized RT vs no RT in oligomet ES-SCLC
📚 Sources · 🐦 1 tweet
🚨 #ASCO26 | #️⃣LBA8005⁰☢️ Concurrent thoracic radiotherapy + chemoimmunotherapy in ES-SCLC
— Masahiro TORASAWA, MD. PhD. (@M_Torasawa) June 2, 2026
👥 ES-SCLC⁰Durvalumab + platinum/etoposide⁰± concurrent thoracic radiotherapy⁰TRT: 30 Gy / 10 fractions, starting day 21–28
📊 Randomized phase III⁰ChemoIO + TRT: n=115⁰ChemoIO… pic.twitter.com/TDA5amz59e
2026-06-01 ASCO Annual Meeting 2026
DeLLphi-304
ForRelapsed SCLC (2L), baseline brain mets, >70% prior CNS-directed therapy
TL;DRIn brain mets, CNS-PFS 6.5 vs 4.2mo HR 0.40 and CNS CR 14.9% vs 5.4% favoring tarlatamab over chemo in 2L SCLC.
The RT read is intracranial control on a pre-treated brain: >70% of brain-mets pts had prior CNS-directed therapy (typically cranial RT), yet tarlatamab extended CNS-PFS to 6.5 vs 4.2 mo (HR 0.40) with CNS CR 14.9% vs 5.4%. Bears on deferring or spacing salvage WBRT/SRS in 2L SCLC with brain mets, not omitting upfront RT.
- Short median f/u 11.4 vs 11.5 mo (tarla vs chemo); intracranial durability beyond ~1y unknown

| Arm (brain mets) | Median CNS PFS | HR (95% CI) |
|---|---|---|
| Tarlatamab (n=67) | 6.5 mo (4.3, 13.7) | 0.40 (0.24, 0.66) |
| Chemotherapy (n=56) | 4.2 mo (2.9, 5.5) | ref |
+2 more figures
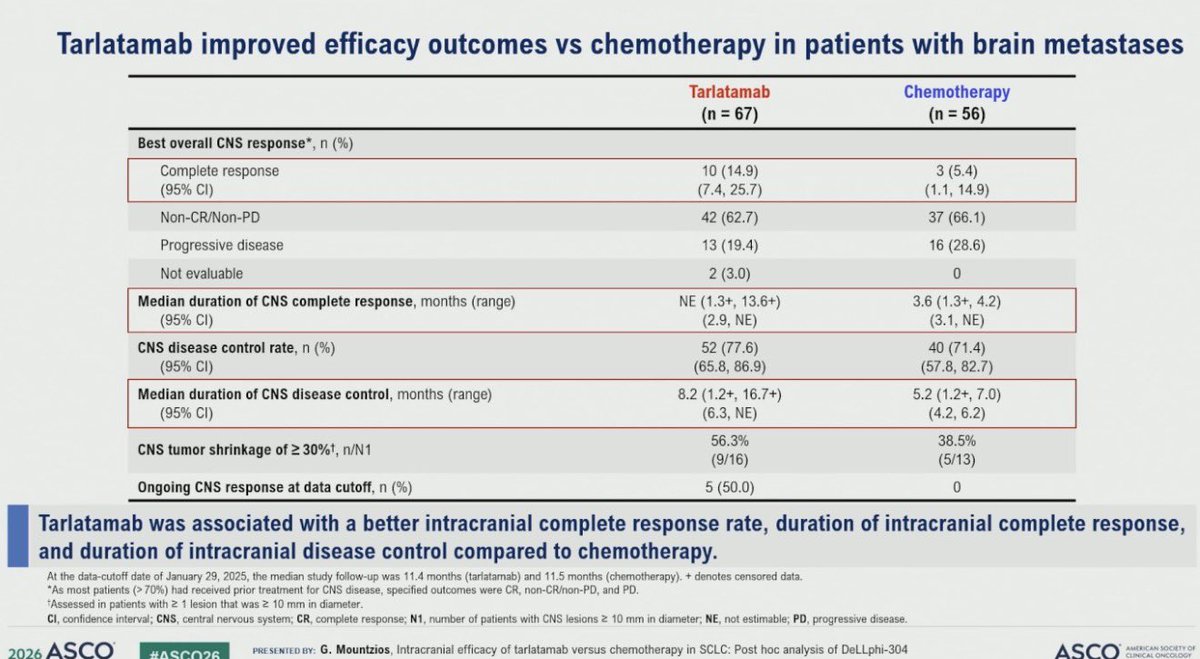
| Endpoint (brain mets) | Tarlatamab (n=67) | Chemotherapy (n=56) |
|---|---|---|
| CNS complete response | 14.9% (7.4, 25.7) | 5.4% (1.1, 14.9) |
| CNS disease control rate | 77.6% (65.8, 86.9) | 71.4% (57.8, 82.7) |
| Median duration CNS DC | 8.2 mo (6.3, NE) | 5.2 mo (4.2, 6.2) |

| Arm (ITT) | Median CNS PFS | HR (95% CI) |
|---|---|---|
| Tarlatamab (n=254) | NE (13.7, NE) | 0.54 (0.39, 0.75) |
| Chemotherapy (n=255) | 7.2 mo (5.6, NE) | ref |
6 details 3 trials watching
- 🔍 Post hoc intracranial analysis of DeLLphi-304 (phase 3 RCT, tarlatamab vs chemo, 2L SCLC); CNS-PFS ITT n=254 vs 255, brain-mets subgroup n=67 vs 56
- 🔍 >70% of brain-mets pts had prior CNS-directed therapy (typically cranial RT); intracranial activity is on a pre-treated brain, not RT-naive
- 📊 Ongoing CNS response at data cutoff: 50.0% tarlatamab vs 0% chemo
- 📊 CNS tumor shrinkage ≥30%: 56.3% (9/16) tarlatamab vs 38.5% (5/13) chemo
- 📐 Brain-mets HR from unstratified Cox (small subgroup); ITT HR from a stratified model
- ⚠️ CNS criteria differ across the two analyses: ITT used RECIST per investigator, brain-mets subgroup used mRANO-BM by BICR
- Can tarlatamab defer or replace salvage cranial RT in SCLC brain mets? n=35 · primary completion 2029-02 · systemic intracranial efficacy in active brain mets
- Durability of intracranial control beyond ~1y median follow-up n=35 · primary completion 2029-02 · intracranial efficacy readout, f/u to 2029
- Activity in CNS-treatment-naive brain mets (most here had prior CNS therapy) n=35 · primary completion 2029-02 · intracranial efficacy in active SCLC brain mets
📚 Sources · 🐦 1 tweet
Dr. @g_mountzios #ASCO26 presents CNS outcomes with 2L tarlatamab in DeLLphi-304. Improved time to CNS progression overall (HR 0.54). In pts with brain nets, tarlatamab vs chemo CNS CR rate 15% vs 5% with DCR 78% vs 71% and time to CBS progression 6.5m vs 4.2m, HR 0.40 pic.twitter.com/5i8jL1zlKW
— Stephen V Liu, MD (@StephenVLiu) June 1, 2026
2026-05-30 ASCO Annual Meeting 2026
CHRYSALIS-2
For1L treatment-naïve atypical EGFR-mutant advanced NSCLC
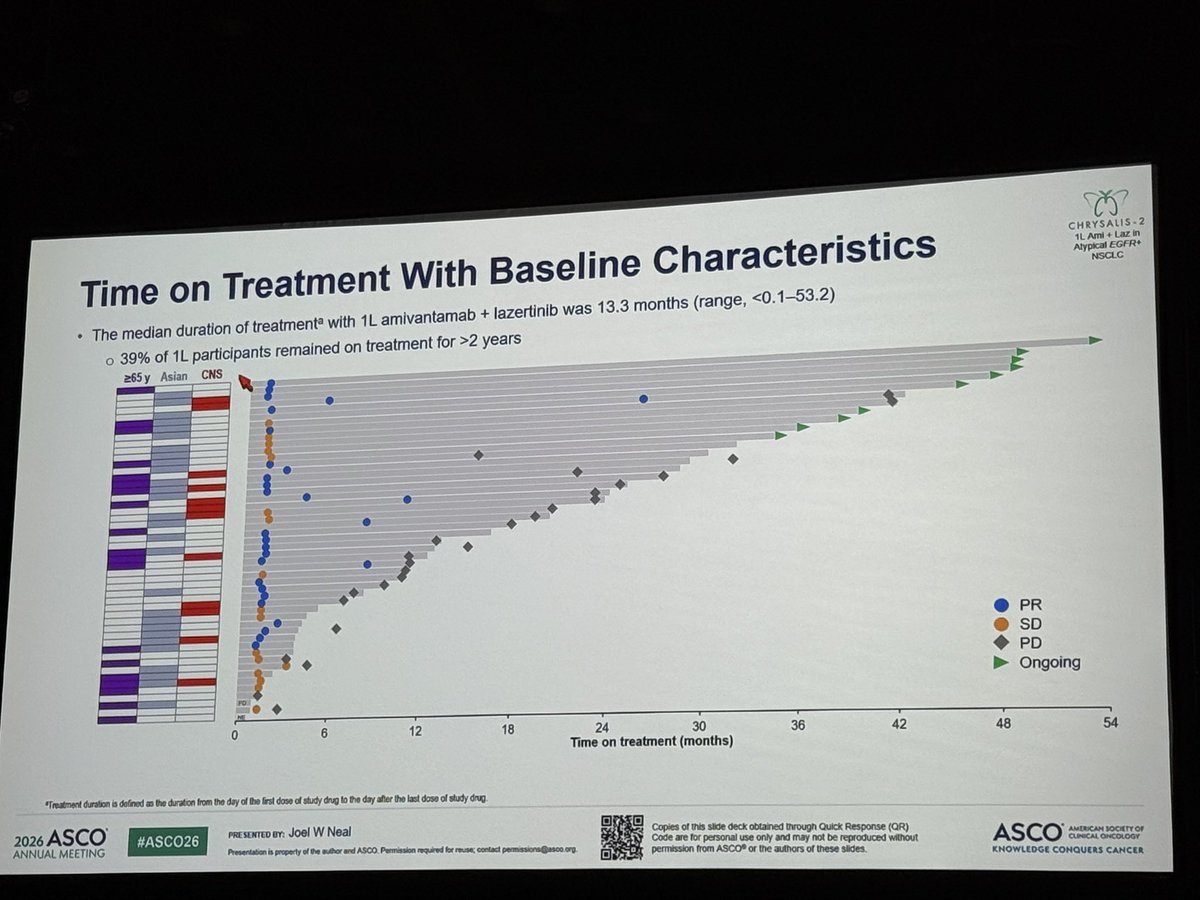
TL;DRmOS 41.0mo (95% CI 27.7-NE) with 1L ami+laz in treatment-naïve atypical EGFR-mutant NSCLC; single-arm, n=49.
- vs common EGFR-mutant 1L ami+laz (MARIPOSA, NEJM 2025): durable OS now extended to atypical EGFR

+1 more figure
8 details 3 trials watching
- 🔍 single-arm, n=49, 1L treatment-naïve atypical EGFR-mutant advanced NSCLC
- 💊 amivantamab (EGFR×MET bispecific) + lazertinib (3rd-gen EGFR TKI)
- 📊 mOS 41.0 mo (95% CI 27.7-NE), median f/u 31.3 mo
- 📊 median tx duration 13.3 mo (range <0.1-53.2)
- 📊 39% of 1L pts remained on treatment >2 yr
- 📊 no clear association between EGFR variant subtype and outcome
- ⚠️ single-arm, no randomized comparator; small N limits subtype-specific conclusions
- ⚠️ atypical EGFR is heterogeneous (S768I, L861Q, G719X, ex20ins); pooled n=49 can't resolve per-subtype benefit
- Activity by specific atypical EGFR subtype (S768I, L861Q, G719X) n=160 · primary completion 2025-06 · phase 1b activity in G719X/S768I uncommon EGFRn=480 · primary completion 2029-02 · phase 3 in PACC uncommon EGFR subtypes
- Randomized comparison vs single-agent osimertinib in atypical EGFR n=480 · primary completion 2029-02 · phase 3 randomized vs osimertinib in PACC uncommon EGFR
- Durability beyond 3.5-year median OS
📚 Sources · 🐦 1 tweet
Amivantamab + lazertinib achieved a median OS of 41.0 months in treatment-naïve atypical EGFR-mutant NSCLC, with no clear association between EGFR variant subtype and outcome. A compelling option. Meanwhile, amivantamab continues evaluation across multiple tumor types. #ASCO26 pic.twitter.com/aWn3Ja60Ji
— Chul Kim (@chulkimMD) May 29, 2026
ESAONA
For1L EGFR-mutant metastatic NSCLC with brain metastases
TL;DRIntracranial ORR 95.5% vs 79.6% (p=0.0004) and iPFS not reached vs 17.5mo, asandeutertinib beating osimertinib in 1L EGFR-mutant NSCLC brain mets.
The RT-relevant read is upfront brain-RT deferral: intracranial ORR 95.5% and iPFS not reached (vs 17.5mo for osimertinib) argue a more CNS-penetrant TKI can hold brain disease without immediate SRS/WBRT. No RT comparator and CNS failure patterns aren't reported, so this informs deferral, not omission.
- Osimertinib (FLAURA-era SOC) already has CNS activity; this positions asandeutertinib as a more CNS-penetrant next-gen TKI, head-to-head
7 details 5 trials watching
- 🔍 Randomized phase II, N=224 (asandeutertinib 111 vs osimertinib 113), 1L EGFR-mutant NSCLC with brain mets, BICR-assessed endpoints
CONSORT flow
- 📊 Efficacy by arm (BICR), asandeutertinib vs osimertinib
Endpoint Asandeutertinib Osimertinib HR / p Intracranial ORR 95.5% (89.8-98.5) 79.6% (71.0-86.6) p=0.0004 Intracranial PFS NR 17.5 mo (15.18-NA) HR 0.46, p=0.0020 Overall PFS NR 17.2 mo (15.18-19.55) HR 0.64, p=0.0473 - 📊 TRAEs by arm
TRAE Asandeutertinib Osimertinib Any 99.1% 95.6% Serious 10.8% 7.1%
- ⚠️ Surrogate endpoints only (iORR, PFS); no OS reported in source
- ⚠️ Overall PFS edge is marginal, p=0.0473 just clears significance; the intracranial signal is the stronger result
- ⚠️ Phase II, both PFS medians not reached in experimental arm → follow-up still immature
- ⚠️ Source is a branded social-media infographic of an LBA, not peer-reviewed primary data
- OS benefit vs osimertinib unproven; PFS/ORR surrogates only not yet High-dose Furmonertinib Versus Osimertinib in Advanced EGFRm NSCLC Patients With Brain Metastases Phase 2n=255 · primary completion 2026-12 · high-dose furmonertinib vs osimertinib, CNS survival
- Durability of intracranial control and CNS failure patterns active Study of Osimertinib + SRS vs Osimertinib Alone for Brain Metastases in EGFR Positive Patients With NSCLC Phase 2n=40 · primary completion 2025-04 · randomized osimertinib ± SRS for EGFR brain metsrecruiting Observation or Upfront Cranial RT in Oncogene Mutated NSCLC With Asymptomatic BM: A Phase III RCT Phase 3n=190 · primary completion 2025-12 · RCT: upfront cranial RT vs obs in asymptomatic BMrecruiting Armatinib Alone or in Combination With SRT for Brain Metastases EGFR-mutated Non-small Cell Lung Cancer Phase 3n=300 · primary completion 2027-12 · phase 3 almonertinib ± SBRT, RT timing for brain metsrecruiting Hippocampus-Protective Radiotherapy Combined With Osimertinib for Symptomatic Brain Metastases in EGFR-Mutated Lung Cancer Phase 2n=74 · primary completion 2028-01 · iPFS of hippocampal-sparing WBRT + osimertinib
📚 Sources · 🐦 1 tweet
#ASCO26 🧠🌍
— Dr Rishabh Jain (@DrRishabhOnco) May 30, 2026
Could a next-generation EGFR TKI outperform osimertinib in patients with brain metastases?
The phase II ESAONA trial suggests the answer may be yes.
🧪 LBA2007 | ESAONA
1L EGFR-mutated NSCLC with brain metastases
👥 n=224
⚔️ Asandeutertinib vs Osimertinib
Key… https://t.co/mEOKGNKgf7 pic.twitter.com/pUQuH6i2cV
OptiTROP-Lung05 NCT06448312
For1L metastatic/unresectable NSCLC, PD-L1 TPS≥1%, no EGFR/ALK alteration
TL;DRmPFS NR vs 5.7mo, HR 0.35, adding TROP2 ADC sac-TMT to 1L pembro in PD-L1+ NSCLC; OS immature (HR 0.55).
- 1L TROP2-ADC+IO data in NSCLC; single-agent TROP2 ADCs (e.g. dato-DXd) showed modest activity in pretreated disease

| Arm | mPFS, mo (95% CI) | PFS events n (%) | HR (95% CI) |
|---|---|---|---|
| Sac-TMT + Pembro | NR (13.6-NE) | 66 (31.7) | 0.35 (0.26-0.47) |
| Pembro | 5.7 (4.3-7.0) | 128 (62.4) | — |
+2 more figures

| PD-L1 TPS | mPFS Sac-TMT+P vs Pembro, mo | HR (95% CI) |
|---|---|---|
| ≥50% | NR vs 9.5 (6.9-13.8) | 0.47 (0.29-0.77) |
| 1-49% | NR vs 4.3 (2.9-5.5) | 0.28 (0.19-0.41) |

| Arm | OS events n (%) | Median OS | HR (95% CI) |
|---|---|---|---|
| Sac-TMT + Pembro | 33 (15.9) | NR | 0.55 (0.36-0.85) |
| Pembro | 54 (26.3) | NR | — |
8 details 4 trials watching
- 🔍 Phase 3, randomized 1:1, open-label, multicenter; N=413 (208 vs 205)
- 🔍 1L NSCLC, PD-L1 TPS≥1% (22C3), no EGFR/ALK, stage IIIB/IIIC or IV, ECOG 0-1
- 💊 Sac-TMT (TROP2 ADC) 4 mg/kg Q2W + pembro 400 mg Q6W vs pembro mono; pembro max 18 cycles
CONSORT flow
- 📊 ORR 70.2% vs 42.0%
- ⚠️ OS immature: descriptive at PFS interim analysis, median f/u 10.5 mo; await mature OS
- ⚠️ Open-label, but primary PFS by blinded independent central review (BICR) limits assessment bias
- ⚠️ Comparator is pembro mono; in PD-L1 TPS 1-49% chemo-IO is standard, so benefit partly vs weaker comparator
- ⚠️ No safety/AE data in source tweets; adding a TROP2 ADC carries toxicity beyond pembro alone
- Does the PFS benefit translate to mature OS? n=614 · primary completion 2028-01 · phase 3 sac-TMT+pembro vs pembro, OS primaryrecruiting Pembrolizumab With or Without Maintenance Sacituzumab Tirumotecan (Sac-TMT; MK-2870) in Metastatic Squamous Non-small Cell Lung Cancer (NSCLC) [MK-2870-023] Phase 3n=851 · primary completion 2029-01 · phase 3 OS, sac-TMT maintenance added to pembro
- Efficacy vs chemo-immunotherapy standard in PD-L1 TPS 1-49%?
- Tolerability of adding a TROP2 ADC to pembrolizumab n=30 · primary completion 2026-06 · phase 1 safety/tolerability, sac-TMT + pembron=356 · primary completion 2026-06 · phase 2 safety/tolerability, sac-TMT + pembro combo
📚 Sources · 🐦 2 tweets
Right patient. Right treatment. Right timing.
— Yakup Ergün (@dr_yakupergun) May 30, 2026
The result: curves like these👇#ASCO26 https://t.co/72KByLKz90
🔁REVIEW #ASCO26 #LCSM Oral
— Hidehito HORINOUCHI (@HHorinouchi) May 30, 2026
🔥OptiTROP-Lung05: 1L Sac-TMT + Pembro vs Pembro in PD-L1+ NSCLC
✅mPFS NR vs 5.7m (HR 0.35)
✅ORR 70.2% vs 42.0%
✅OS HR 0.55 (95%CI 0.36-0.85, immature)
🎙️Dr. Caicun Zhou
🔗 https://t.co/DcbK1dGrhO@OncoAlert @Larvol @ASCO @IASLC https://t.co/512k6dZviW pic.twitter.com/Vdo86N50h9
2026-05-29 ASCO Annual Meeting 2026
Wait or Treat — Upfront vs Delayed Cranial RT in Asymptomatic Brain Mets, Oncogene-Mutated NSCLC (NCT05236946) NCT05236946
ForMetastatic EGFR/ALK+ NSCLC, asymptomatic measurable brain mets, ECOG 0-2
TL;DRicPFS sub-HR 0.35 favoring upfront RT but no OS gain (2y OS 48% vs 60%, HR 1.45 favoring delayed).
The RT read is local control without a survival payoff: upfront cranial RT cut 2y intracranial progression to 21.7% vs 50% (sub-HR 0.35), but 2y OS ran 48% vs 60% favoring delayed and added radiation necrosis (6% vs 0%). Supports deferring RT, letting TKI hold the CNS, reserving RT for intracranial PD.
- Consistent with TKI-first/defer-RT direction in oncogene-driven NSCLC (CNS-penetrant osimertinib, lorlatinib)

| Intracranial progression | Upfront RT | Delayed RT |
|---|---|---|
| 1-year | 8.7% (2.9-14.5) | 25.7% (16.8-34.7) |
| 2-year | 21.7% (12.6-30.8) | 50% (39.2-60.9) |
| Sub-HR | 0.35 (0.21-0.59) | ref |
| Events | 20 | 47 |
7 details 4 trials watching
- 🔍 Phase III open-label RCT, N=208 (1:1), EGFR/ALK+ metastatic NSCLC w/ asymptomatic measurable brain mets; both arms TKI + chemo
- 🔍 Delayed arm got cranial RT only at intracranial PD or patient wish; MRI brain q3mo yr 1, then q6mo; median f/u 30.6mo
- 🔍 RT dose, fractionation, and modality (SRS vs WBRT) not reported in source
- 🔍 Stratified by GPA score (0-2 vs >2) and synchronous vs metachronous BM
CONSORT flow
- 📊 OS not improved by upfront RT: 2y OS 48% upfront vs 60% delayed, OS HR 1.45 (favoring delayed)
- ⚠️ Radiation necrosis 6% upfront vs none in delayed arm; less severe with delay (per @DrRiyazShah, @StephenVLiu)
- ⚠️ Open-label: neurocognition, PROM, toxicity (secondary endpoints) subject to assessment bias; not reported in source
- Neurocognition and quality-of-life outcomes by RT timing
- Whether CNS-active TKI choice modifies upfront RT benefit n=162 · primary completion 2024-12 · osimertinib ± early SRS in asymptomatic metsrecruiting Delayed or Upfront Brain RAdiotherapy in Treatment naïve Lung Cancer Patients With Asymptomatic or Minimally Symptomatic Brain Metastases and ALK rEarrangements Phase 1/2n=56 · primary completion 2028-02 · alectinib ± upfront SRS in ALK+ brain metsrecruiting Early or Delayed Intervention of Brain Radiotherapy Combined With Almonertinib in EGFR Mutated NSCLC With Brain Metastases Phase 3n=232 · primary completion 2028-12 · early vs delayed brain RT on almonertinib, EGFR
- Optimal cranial RT modality (SRS vs WBRT) for upfront treatment active Hippocampal Sparing Whole Brain Radiation Versus Stereotactic Radiation in Patients With 5-20 Brain Metastases: A Phase III, Randomized Trial Phase NAn=196 · primary completion 2024-11 · phase 3 hippocampal-sparing WBRT vs SRS
📚 Sources · 🐦 3 tweets
#ASCO26 | Wait or Treat? Brain RT in EGFR/ALK+ NSCLC
— OncLive.com (@OncLive) May 29, 2026
Presented by Dr Anil Ramakant Tibdewal.
A landmark Phase III randomized trial from @TataMemorial addressed a long-standing question: should asymptomatic brain metastases in oncogene-driven NSCLC receive upfront cranial RT or… pic.twitter.com/lRy9CfyQ8r
Should asymptomatic brain mets await systemic response in front line within EGFR/ALK context? I think yes. Despite reducing icPD, delayed brain RT OS looked better and radiation necrosis didn’t occur vs 6% #ASCO26 pic.twitter.com/O6d7GrvtU4
— Dr Riyaz Shah (@DrRiyazShah) May 29, 2026
No improvement in survival with up front radiation. OS favored delayed radiation with 2y OS 48% with early radiation vs 60% in late (OS HR 1.45). Also, radiation necrosis less common and less severe in delayed arm. Each case unique but delayed approach appealing #ASCO26 pic.twitter.com/wIhjqxhSaq
— Stephen V Liu, MD (@StephenVLiu) May 29, 2026
2026-05-26
SWOG/NRG S1914 NCT04214262
ForInoperable/surgery-declined T1-3N0M0 NSCLC ≤7cm, ≥1 recurrence risk factor
TL;DROS no different adding atezolizumab to SBRT in high-risk early-stage NSCLC: HR 1.15 (0.65-2.01), p=0.63; more local failure and G3+ AEs with IO.
The RT read is local control: adding atezo numerically worsened it (local failure 13% vs 7%), opposite the radiosensitization rationale, while SBRT alone held 82% 2-yr OS. No basis to add IO to SBRT off-protocol for inoperable early-stage NSCLC. Former/never smokers fared worse with IO (OS HR 2.50).
- First phase III to test IO + SBRT in early-stage NSCLC; refutes the positive phase II signal (I-SABR, PMID 37478883)
8 details
- 🔍 Phase III RCT, 403 eligible (201 SBRT alone / 202 atezo+SBRT); accrual goal was 432
- 🔍 Pts: T1-3N0M0 NSCLC ≤7cm, medically inoperable or surgery-declined, ≥1 recurrence risk factor (tumor ≥2cm, higher-grade histology)
- 🔍 SBRT 3-8 fx, BED ≥100 Gy; atezo 1200mg Q3wk ×8, SBRT from cycle 3 (neoadj/concurrent/adjuvant)
- 💊 G≥3 AEs far higher with added IO: 12% (AS) vs 2% (S)
- AS: 21 G3, 1 G4, 1 G5 (fatal respiratory failure)
- S: 3 G3, 1 G4
CONSORT flow
- 📊 Efficacy + failure patterns by arm (SBRT alone vs atezo+SBRT)
Endpoint SBRT (S) Atezo+SBRT (AS) HR (95% CI), p 2-yr OS 82% 80% 1.15 (0.65-2.01), p=0.63 2-yr PFS 71% 60% 1.35 (0.89-2.06), p=0.16 Local failure 7% 13% — Regional failure 2% 3% — Distant failure 4% 5% —
- ⚠️ Closed at first interim for futility (OS + PFS) per design; median f/u only 12 mo, 49 deaths — OS immature
- ⚠️ Added IO trended toward worse local control, opposite the radiosensitization rationale
- ⚠️ Former (53%) / never (3%) smokers did worse with added IO — unplanned subgroup, hypothesis-generating
- OS: HR 2.50 (1.11-5.59), p=0.03
- PFS: HR 2.16 (1.15-4.04), p=0.01
- Whether a PD-L1 or biomarker subset benefits from IO added to SBRT
- Why former/never smokers did worse with added atezolizumab
- Whether central review confirms the higher local-failure rate with IO
📚 Sources · 📄 1 paper
Abstract
2026-05-20
LS-SCLC High-Dose Hyperfractionated RT (54 Gy vs 45 Gy) Phase 3 NCT03214003
ForLimited-stage SCLC, ECOG 0-1, age 18-70, untreated or 1 prior chemo cycle
TL;DRmOS 60.7 vs 39.5mo, HR 0.55 (0.37-0.72), p=0.003 favoring 54Gy twice-daily SIB over 45Gy in LS-SCLC.
The transferable detail: the 54Gy boost hit only the GTV, the PTV stayed at 45Gy/30fx, so G3-4 oesophagitis (13 vs 12%) and pneumonitis (5 vs 6%) held flat despite the mOS jump to 60.7 vs 39.5mo. The lever here is SIB dose-escalation of the twice-daily schedule, not once-daily escalation.
- Standard LS-SCLC RT is 45Gy twice-daily (Turrisi, NEJM 1999); CONVERT found no OS gain from once-daily dose escalation. This escalates the twice-daily schedule itself to 54Gy
8 details 2 trials watching
- 🔍 Phase 3 open-label RCT, 16 Chinese sites, N=224 (54Gy 108 / 45Gy 116); median f/u 46mo
- 🔍 SIB technique: 54Gy/30fx boost to GTV only; PTV held at 45Gy/30fx in both arms
- 🔍 Both arms accelerated twice-daily VMAT, 10fx/week, concurrent platinum-etoposide; PCI 25Gy/10fx for responders
CONSORT flow
- 📊 1° EP OS (ITT): mOS 60.7mo (95% CI 49.2-62.0) with 54Gy vs 39.5mo (27.5-51.4) with 45Gy
- 📐 OS HR 0.55 (95% CI 0.37-0.72), p=0.003
- 📊 G3-4 radiotherapy toxicity by arm — comparison values omitted (cell value "0.84" not verified in source)
- ⚠️ DSMB-terminated early (Apr 2021) for sufficient benefit; early stopping can overestimate effect size
- ⚠️ Open-label, modest N=224, single-country (China); the unusually large OS gain warrants Western confirmation
- Generalizability beyond Chinese single-country cohort
- Comparison vs once-daily high-dose thoracic RT (66-70Gy)
- Dose escalation value with durvalumab consolidation (ADRIATIC era) n=70 · primary completion 2029-06 · phase 3 durvalumab consolidation after CRT in LS-SCLCn=100 · primary completion 2029-07 · durvalumab induction + chemoRT + maintenance, LS-SCLC
📚 Sources · 📄 1 paper
2026-05-19
Single-fraction SABR: pooled analysis (n=1687)
ForPrimary NSCLC (n=1200) or pulmonary oligometastases (n=487)
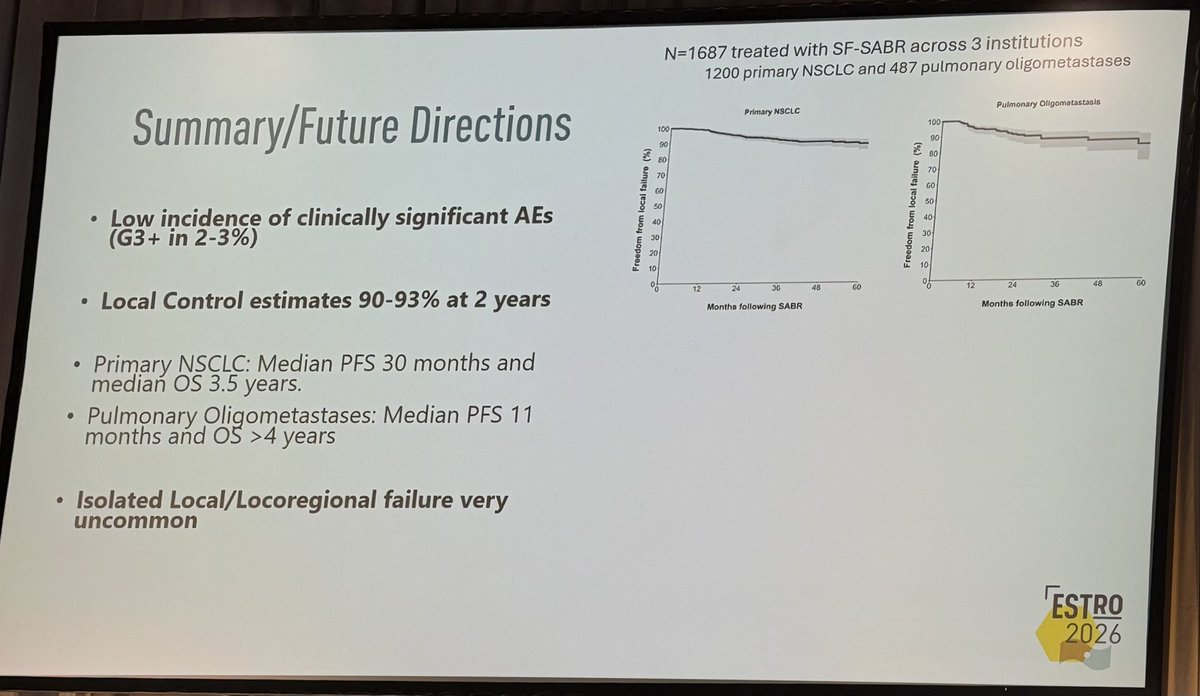
TL;DR2yr local control 90-93% with G3+ AEs 2.9%, across 1687 pts (1200 primary NSCLC, 487 oligomets) on single-fraction SABR.
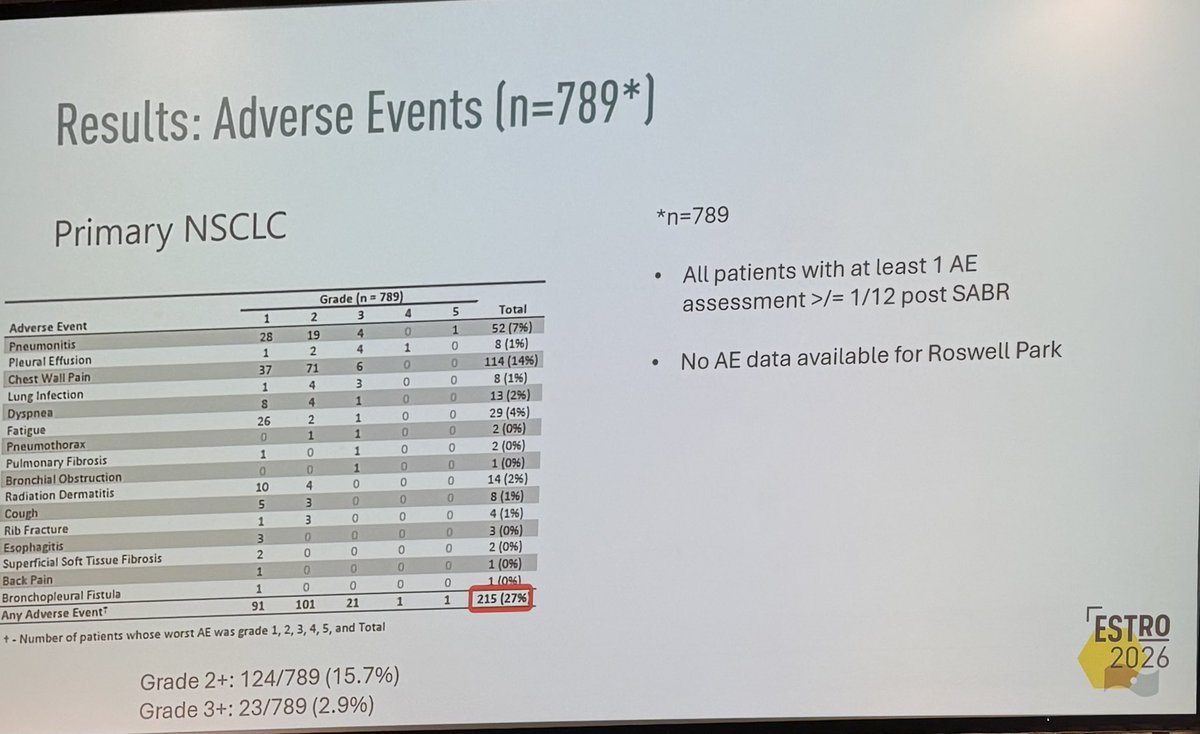
The RT read is toxicity, not the survival curves: chest wall pain (14%) dominates and G3+ sits at just 2.9% (n=789), so single-fraction earns its 'one-stop' pitch. But the prescription dose (Gy) isn't in the source, which gates whether this transfers to your practice.
- Supports single-fraction approach; cf. RTOG 0915 (34Gy x1 for peripheral stage I NSCLC)
+2 more figures
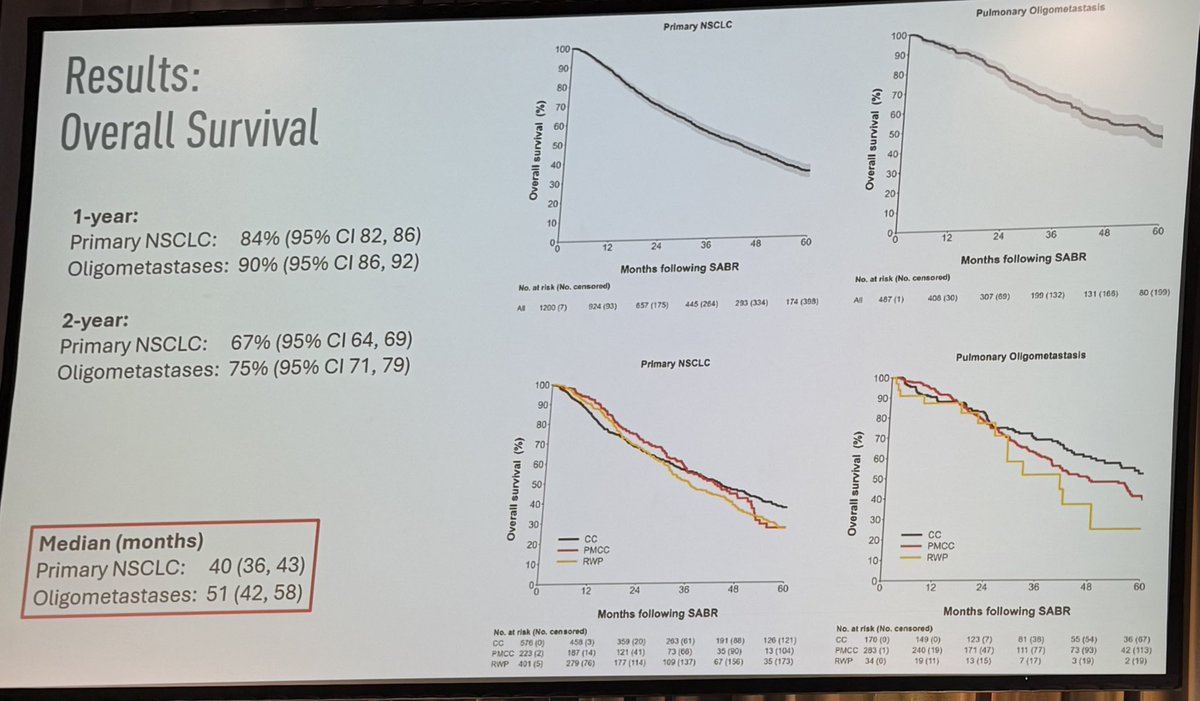
| Cohort | 1yr OS | 2yr OS | Median OS |
|---|---|---|---|
| Primary NSCLC | 84% (82-86) | 67% (64-69) | 40mo (36-43) |
| Oligomets | 90% (86-92) | 75% (71-79) | 51mo (42-58) |
6 details 2 trials watching
- 🔍 Pooled retrospective analysis, 3 institutions (Peter Mac, Cleveland Clinic, Roswell Park); 1200 primary NSCLC + 487 pulmonary oligomets
- 🔍 Single-fraction SABR (one fraction); total dose (Gy) not reported in source
- 📊 Isolated local/locoregional failure very uncommon across both cohorts
- 📊 Most common AEs, primary NSCLC (n=789)
- Chest wall pain 114 (14%), most common
- Pneumonitis 52 (7%)
- Fatigue 29 (4%)
- Rib fracture 4 (1%)
- ⚠️ No randomised comparator; dose/fractionation heterogeneity across 3 sites not detailed in source
- ⚠️ AE data missing for Roswell Park (n=789 of 1687); toxicity may be undercounted
- Single-fraction vs multifraction SABR for pulmonary oligometastases recruiting OligoCare TwiCs (Trials Within Cohorts) Trial Comparing Acute Toxicity in Single-fraction vs Multiple-fraction SBRT for Metastasis-directed Treatment (SPRINT) Phase NAn=302 · primary completion 2029-02 · single-fx vs multi-fx SBRT for oligomets incl NSCLC
- Optimal single-fraction dose and patient selection for primary NSCLC active A Pilot Study of Single Fraction Stereotactic Body Radiation Therapy (SBRT) in Central Non-Small Cell Lung Cancer Phase NAn=30 · primary completion 2028-03 · single-fx SBRT vs multi-fx in central NSCLC
- Durability beyond 2 years and late toxicity
📚 Sources · 🐦 1 tweet
👏🏽👏🏽👏🏽@neildwallaceie at #ESTRO26 - 1687 patients receiving single fraction SABR for #lungcancer and pulmonary oligomets, @PeterMacRadOnc / @ClevelandClinic / @RoswellPark. Fantastic local control, and low adverse rates. Should we be using “one stop” SABR more often #radonc ? pic.twitter.com/w2IlGKRU5o
— Shankar Siva (@_ShankarSiva) May 18, 2026