Prostate
Nodal staging strategy, not a new trial: PSMA-PET vs ePLND read through an RT-morbidity lens.
ePLND vs PSMA PET staging in prostate cancer (AUA 2026)
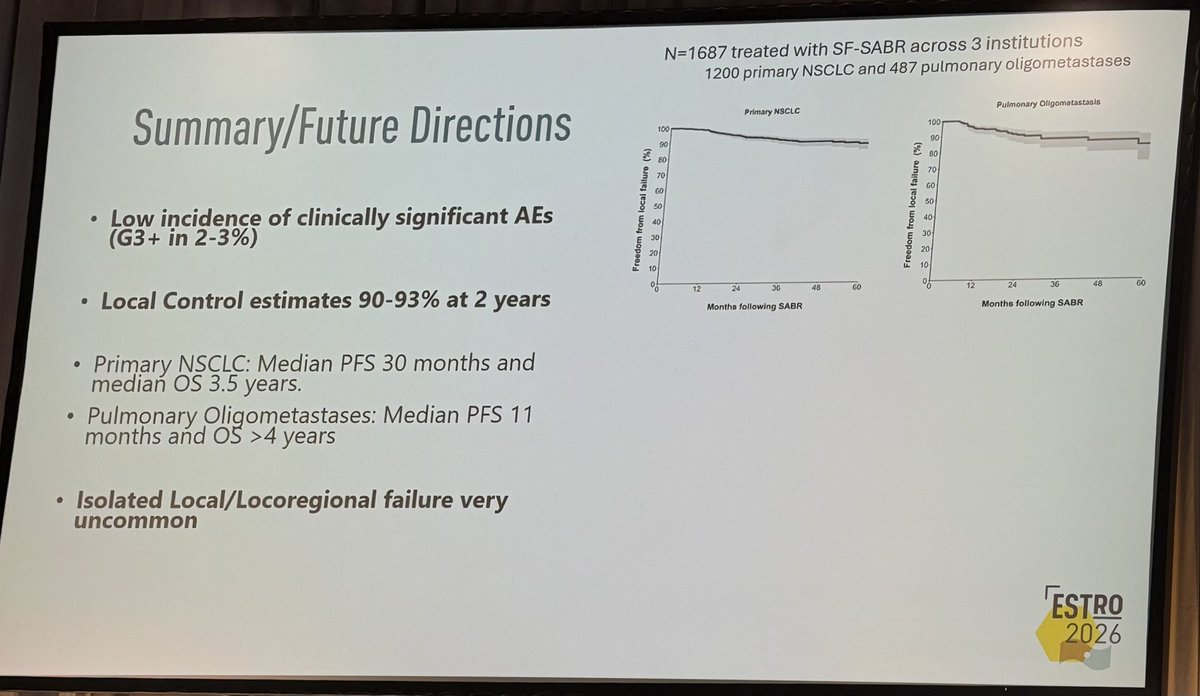
TL;DRPSMA PET/CT (NPV ~96%) may safely omit ePLND for nodal staging; ePLND's therapeutic benefit unproven and its morbidity compounds with pelvic RT.
The RT read is compounded morbidity: lymphedema runs 19-29% after PLND plus salvage pelvic RT (2-22% also genital) vs 0-9% for nodal RT alone. With PSMA PET NPV ~96%, omitting ePLND when pelvic nodal RT is anticipated spares that additive toxicity without losing staging confidence.
- RT-relevant: PSMA-PET staging can route to post-op pelvic nodal RT, sparing ePLND and its additive morbidity, especially with no prior eLND (Roberts, PCAN 2024)

+1 more figure

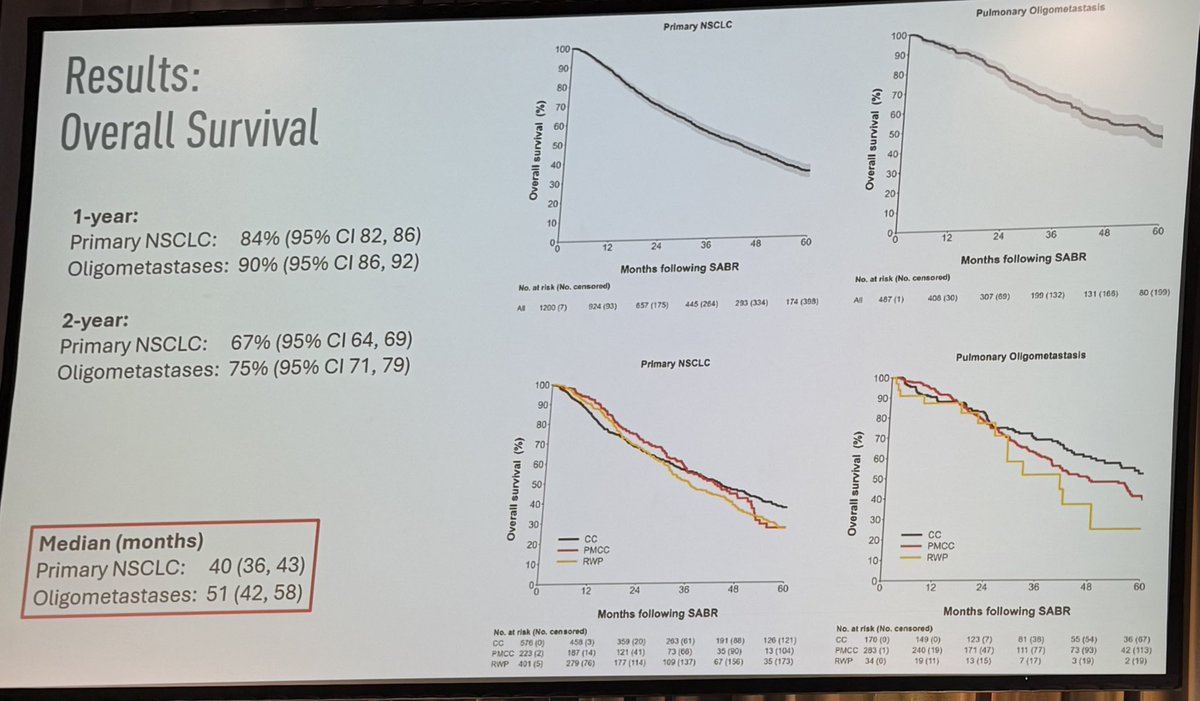
| Setting | Lower-limb lymphedema | Genital lymphedema |
|---|---|---|
| RP + PLND | 0-14% | — |
| Pelvic LN RT | 0-9% | — |
| PLND + salvage pelvic RT | 19-29% | 2-22% |
6 details 4 trials watching
- 🔍 Proposed risk-tiered PLND decision
- Intermediate-risk: omit PLND if PSMA PET LNI-negative; missed LN small, would be missed in ePLND too
- GG3: nomograms add value
- High-risk: individualized; flag that adjuvant/salvage pelvic RT may increase side effects
- 🔍 If PLND is performed, it should be extended (ePLND), per the AUA 2026 message
- 📊 RCTs have not shown consistent BCR improvement from ePLND; provides staging, therapeutic benefit unproven
- 📊 PSMA PET/CT NPV ~96% for nodal disease; a negative scan may safely avoid unnecessary PLND
- ⚠️ PLND morbidity beyond lymphedema: 6-10x increased DVT/PE risk (Tyritzis, 3544 pts RP vs RARP)
- ⚠️ Perspective/review synthesis, not new RCT data; level 1 evidence for ePLND oncological benefit absent
- Oncological benefit of ePLND beyond staging recruiting Extended vs. No Pelvic Lymph Node Dissection During Radical Prostatectomy. DISSECTION 2.0. Phase NAn=400 · primary completion 2027-02 · RCT: extended vs no PLND tests therapeutic benefit
- PSMA PET reliability for nodal staging in high-risk disease recruiting Dutch National Randomized Study: PSMA-PET/CT As a Triage Tool for Pelvic Lymph Node Dissection in Prostatectomy Patients Phase NAn=706 · primary completion 2025-07 · RCT: PSMA PET triages ePLND, comparable prognosisrecruiting Accuracy of 18F-rhPSMA-7.3 PET/ MRI for Prediction of Lymph Node Metastasis in Localized High-Risk Prostate Cancer Phase NAn=50 · primary completion 2027-05 · PSMA PET/MRI accuracy vs PLND for LN mets, high-riskrecruiting Preoperative PSMA PET/CT As Triage for EPLND in Patients Scheduled for RALP (PrePSMA) Phase NAn=600 · primary completion 2029-12 · tests if PSMA PET can replace ePLND for staging
📚 Sources · 🐦 1 tweet
At #AUA2026, the message was clear:⁰📌 ePLND provides staging information, but its therapeutic benefit remains uncertain.⁰📌 RCTs have not shown consistent improvements in BCR outcomes.⁰📌 PSMA PET/CT has a high NPV (~96%) and may safely avoid unnecessary PLND in… pic.twitter.com/7vJFe2hG77
— DR CARVAJAL (@RomanCarvajal) May 17, 2026