Prostate
2026-06-25
ENZARAD (ANZUP 1303)
ForHigh-risk localized/locally-advanced prostate, Gleason 8-10, EBRT-eligible
TL;DRPrimary MFS endpoint negative (HR 0.88, p=0.34); enzalutamide benefit concentrated in cN1 (HR 0.43) and planned-pelvic-RT (HR 0.47) subgroups.
Reported via UroToday →
The actionable split is by RT field: enzalutamide's benefit concentrates in cN1 (MFS HR 0.43) and planned-pelvic-RT (HR 0.47) pts, near-absent otherwise. But the pelvic-RT subgroup carried far higher baseline risk (28% N1 vs 0%), so nodal coverage and risk are confounded. Moves the cN1/pelvic-RT intensification decision, not cN0.
- Weaker all-pt effect vs STAMPEDE abiraterone tracks more favorable ENZARAD risk profile
9 details 2 trials watching
- 🔍 International phase III, N=802 (8 countries), median f/u 8yr
- 💊 Exp = enzalutamide 160mg ×24mo; control = conventional NSAA ×6mo; both +24mo LHRH +EBRT
- 🔍 RT: prostate 78Gy or 46Gy+brachy boost; pelvic nodes required for cN1 (46Gy elective +boost to gross nodes), optional/pre-declared for cN0
- 📊 1° EP MFS negative: 8-yr 74% vs 72%, HR 0.88 (0.67-1.15), p=0.34
- 📊 PFS positive: 8-yr 67% vs 62%, HR 0.78 (0.61-0.99), p=0.044
- 📊 OS NS: 8-yr 83% vs 80%, HR 0.87 (0.63-1.20), p=0.40 (OS was original 1° EP, switched to MFS after fewer deaths than expected)
- 📊 Prespecified subgroup HRs (enzalutamide favored)
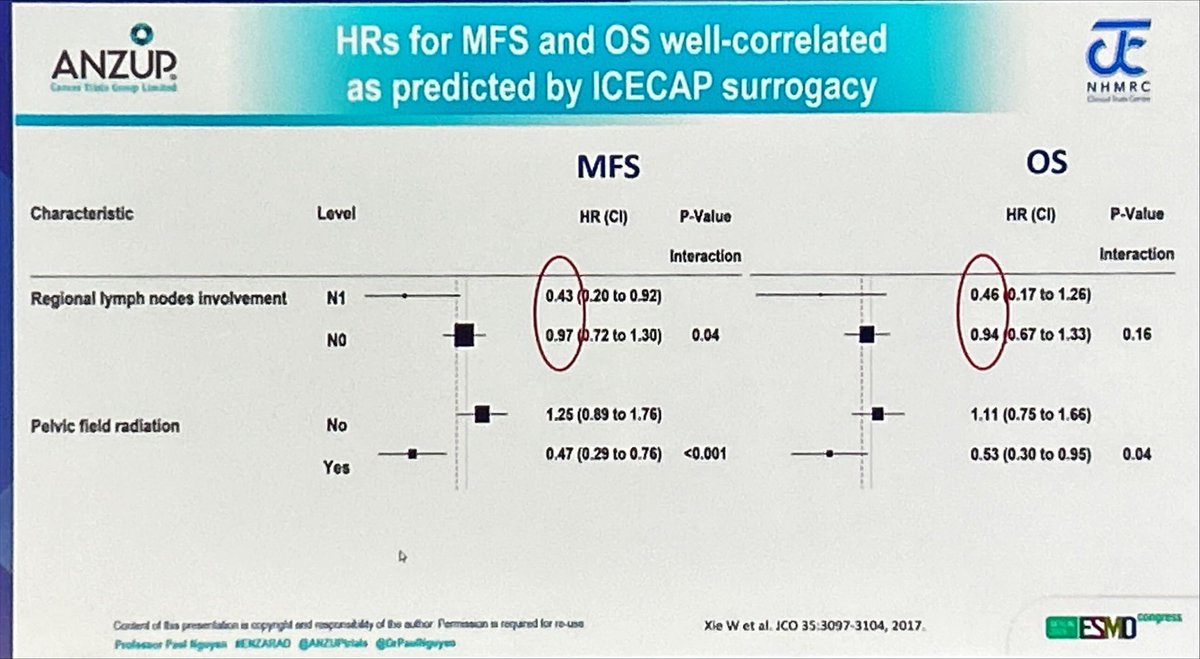
Subgroup MFS HR (95% CI) OS HR (95% CI) cN1 regional nodes 0.43 (0.20-0.92) 0.46 (0.17-1.26) Pelvic RT planned 0.47 (0.29-0.76) 0.53 (0.30-0.95) Very high-risk 0.85 (0.64-1.13) 0.81 (0.57-1.13)
- ⚠️ Pelvic-RT subgroup confounded by risk: that group 28% N1 / 62% Gleason 9-10 vs 0% N1 / 49% Gleason 9-10 in no-pelvic-RT pts
- ⚠️ Subgroups preplanned but hypothesis-generating; p-values nominal, no multiplicity adjustment, wide CIs
- Which pelvic-RT subgroups drive the enzalutamide benefit recruiting Reduced Length of ADT and ARTA With XRT in High-Risk Prostate Cancer (RELAX): A Randomised Trial Phase 2n=206 · primary completion 2035-01 · high-risk pelvic-nodal XRT + enza/abi intensification
- Biomarkers to select patients for treatment intensification active Genomics in Michigan to AdJust Outcomes in Prostate canceR (G-MAJOR) for Men With Newly Diagnosed Favorable Risk Prostate Cancer Phase NAn=805 · primary completion 2028-03 · Decipher/Prolaris genomic classifier decision impact
- Whether pelvic nodal RT is required for enzalutamide's distant-met benefit
📚 Sources · 📄 1 paper
Abstract
2026-06-18
PRIMARY2 NCT05154162
ForBiopsy-naive, high clinical risk, PI-RADS 2-3 MRI, PSA ≤20 ng/mL, ≤cT2
TL;DRPSMA-PET avoided biopsy in 49% while csPCa detection (12% vs 16%, diff −3.7%, 95% CI −8.9 to 1.5) was non-inferior to systematic biopsy.
- Extends PRIMARY1 (defined the PRIMARY score used here): PSMA-PET+MRI sharpened csPCa detection; PRIMARY2 converts that read into a biopsy-avoidance strategy
8 details 5 trials watching
- 🔍 Phase 3 non-inferiority RCT, 7 Australian sites, N=660 biopsy-naive, randomised 1:1, no masking, ITT (NCT05154162)
- 🔍 Strategy: negative PSMA-PET (PRIMARY score 1-2) → biopsy avoided; positive (3-5) → PSMA-PET-targeted transperineal biopsy
- 🔍 Enrolled high clinical risk despite non-suspicious/equivocal MRI (PI-RADS 2 51%, PI-RADS 3 49%); any one of:
- PSA density >0.1 ng/mL/mL
- Strong family history of prostate cancer
- Abnormal DRE or BRCA mutation
- PSA >10 ng/mL, PSADT <36mo, or PSA velocity >0.75 ng/mL/yr
- All with PSA ≤20 ng/mL and ≤cT2
CONSORT flow
- 📊 Co-1° EP (biopsy avoidance): 163/331 (49%) avoided biopsy with PSMA-PET (95% CI 44-55), p<0.0001 vs 20% threshold
- 📊 Co-1° EP (csPCa detection): 39/331 (12%) PSMA-PET vs 51/329 (16%) biopsy; diff −3.7% (95% CI −8.9 to 1.5), p=0.0093, non-inferior (10% margin)
- 📊 Post-biopsy symptoms by arm (among those biopsied)
Symptom PSMA-PET arm Biopsy arm Pain 21% (33) 21% (62) Haematuria 38% (60) 43% (126) Haematospermia 48% (77) 45% (133)
- ⚠️ Non-inferiority, not superiority: PSMA-PET detected fewer csPCa (12 vs 16%); point estimate favours biopsy, rests on the 10% margin
- ⚠️ Follow-up ongoing; whether biopsy-avoided men harbour missed csPCa is not yet established at maturity
- Missed csPCa in biopsy-avoided men at longer follow-up n=230 · primary completion 2026-09 · PSMA-PET/MRI bx targets missed csPCa, prior neg bxrecruiting Biological Markers and Advanced Imaging for Prostate Cancer Progression in Active Surveillance Phase NAn=74 · primary completion 2028-05 · PSMA-PET flags GG2+ upgrade at 1y confirmatory bx
- Generalisability to 18F-PSMA tracers and other settings recruiting Fully Hybrid 18F-PSMA PET/MRI as One-stop Approach for the Diagnosis of Clinically Significant Prostate Cancer. Phase 2n=167 · primary completion 2026-03 · 18F-PSMA+mpMRI pre-bx to cut false negativesactive Study of PSMA-targeted 18F-DCFPyL PET/CT for the Detection of Clinically Significant Prostate Cancer Phase 2n=150 · primary completion 2028-03 · 18F-DCFPyL PET csPCa detection, screening popn=30 · primary completion 2030-07 · 18F-rhPSMA-7.3 PET for PIRADS 2/3 vs MRI bx
- Cost-effectiveness vs systematic biopsy
📚 Sources · 📄 1 paper
2026-06-16
REVELUTION
ForNon-metastatic prostate ca, intermediate/high-risk, on ADT with pelvic RT
TL;DRAdjusted total plaque volume +68.9mm³ with leuprolide vs relugolix at 12mo, GnRH agonist accelerating coronary atherosclerosis.
Reported via UroToday →
Leuprolide added +68.9mm³ adjusted total coronary plaque vs relugolix at 12mo (driven by non-calcified plaque), a mechanism for HERO's MACE signal. For the radonc prescribing ADT alongside prostate RT, this supports choosing relugolix in pts with baseline cardiovascular risk.
- vs HERO (2020): HERO showed lower MACE with relugolix; REVELUTION supplies a coronary-plaque-progression mechanism for that signal
8 details 3 trials watching
- 🔍 Single-institution open-label RCT (4 Emory centers); ADT-eligible pts 1:1 relugolix vs leuprolide, stratified by ASCVD 10yr risk; N=94 enrolled
- 🔍 All pts got pelvic RT (prostate ± nodes), intermediate/high-risk; parallel prospective RT-alone (no ADT) cohort as control
- 💊 Relugolix 360mg load → 120mg/day vs leuprolide 3-month depot, ADT ≥6mo
- 🔍 Serial CCTA baseline + 12mo, blinded to arm, HeartFlow automated quantification; ANCOVA adjusted for age, statin, baseline plaque
- 📊 1° EP (12mo total coronary plaque volume change): adjusted mean difference +68.9mm³ favoring relugolix over leuprolide
- 📐 Crude 12mo total plaque volume Δ: leuprolide 56mm³ vs relugolix 25mm³
- 📊 Difference driven by non-calcified plaque; calcified + low-attenuation plaque changes small, no significant between-arm difference
- ⚠️ Surrogate imaging endpoint (plaque volume) not clinical MACE; small single-institution N, 12mo f/u, open-label (imaging read blinded)
- Does the plaque-volume difference translate to clinical MACE reduction? n=94 · primary completion 2025-01 · relugolix vs leuprolide coronary-vessel cardiac trialrecruiting Effects of Relugolix vs Leuprolide on Cardiac Function in Patients With Prostate Cancer Phase 2n=70 · primary completion 2027-12 · relugolix vs leuprolide cardiac function + MRIrecruiting REVELUTION-2: Relugolix+Abiraterone Acetate (AA) Versus Leuprolide+AA Cardiac Trial Phase 3n=72 · primary completion 2029-07 · phase 3 relugolix vs leuprolide+AA cardiac trial
- Durability of the plaque difference beyond 12 months
- Generalizability beyond a single-institution pelvic-RT population
📚 Sources · 📄 1 paper
Abstract
2026-06-12
ORIOLE NCT02680587
ForRecurrent oligometastatic HSPC, 1-3 mets, no ADT within 6mo
TL;DRSABR cut 6-mo progression to 19% vs 61% (P=.005) and improved mPFS (NR vs 5.8mo, HR 0.30) in oligomet HSPC.
Surfaced from a review's discussed trials
The RT-actionable signal is target definition, not the headline: men whose PSMA-PET-avid disease was fully consolidated had mDMFS 29.0 vs 6.0 mo (HR 0.19) over those with PET lesions left untreated. Argues for PSMA-PET-guided total consolidation, not conventional-imaging-only targeting, when offering oligomet SABR.
- vs STOMP (phase 2 MDT): consistent metastasis-directed benefit; together anchor the oligomet-prostate MDT paradigm
8 details 5 trials watching
- 🔍 Phase 2 RCT, N=54, randomized 2:1 SABR:observation; recurrent HSPC, 1-3 mets on conventional imaging, ADT-free within 6mo
CONSORT flow
- 📊 1° EP — composite progression at 6mo: 7/36 (19%) SABR vs 11/18 (61%) observation, P=.005
- 📊 PFS efficacy, SABR vs observation
Endpoint SABR Observation HR (95% CI), p mPFS not reached 5.8 mo 0.30 (0.11-0.81), p=.002 Biochemical PFS not reached 6.4 mo 0.31 (0.13-0.75), p=.002 PSA progression 6mo 4/36 (11%) 9/18 (50%) p=.005 - 📊 Local control 98.9% at 6mo; no grade 3+ AEs (SABR well tolerated)
- 📊 PSMA-PET consolidation matters — team blinded to PET, so 16/36 had PET-avid lesions left untreated
Outcome All PSMA disease treated (n=19) Any PSMA lesion untreated (n=16) HR / p Progression at 6mo 1/19 (5%) 6/16 (38%) P=.03 mPFS not reached 11.8 mo 0.26 (0.09-0.76), p=.006 New mets at 180d 3/19 (15.8%) 10/16 (62.5%) P=.006 mDMFS 29.0 mo 6.0 mo 0.19 (0.07-0.54), p<.001
- ⚠️ Primary is a 6-mo composite surrogate (PSA/imaging/symptoms/ADT-start/death), not OS or MFS
- ⚠️ Small N=54, short median f/u 18.8mo; Gleason higher in observation arm (mean 8 vs 7) despite randomization
- ⚠️ Exploratory: PFS benefit confined to high-risk-mutation-negative subgroup (biomarker-gated)
- Durability of ADT-free interval and MFS/OS benefit beyond 6-month endpoint active Prostate-cancer Treatment Using Stereotactic Radiotherapy for Oligometastases Ablation in Hormone-sensitive Patients Phase 3n=550 · primary completion 2026-06 · phase 3 ablative RT vs SOC, MFS in oligomet HSPCrecruiting Metastasis Directed Stereotactic Body Radiotherapy for Oligo Metastatic Hormone Sensitive Prostate Cancer Phase NAn=118 · primary completion 2031-12 · phase 3 MD-SBRT vs SOC, failure-free survival 1°EP
- Does PSMA-PET-guided total consolidation improve outcomes vs conventional imaging? n=130 · primary completion 2026-05 · RT guided by PSMA-PET vs conventional staging
- MDT alone vs MDT plus systemic intensification in oligomet HSPC n=88 · primary completion 2028-12 · SABR+ADT vs added niraparib/abiraterone 6morecruiting Duration of Androgen Receptor Pathway Inhibitor and ADT With Metastasis Directed Therapy in Oligometastatic Cancer of the Prostate (DIRECT) Phase 2n=132 · primary completion 2031-02 · SBRT+ADT ± 8-9mo abiraterone intensification
📚 Sources · 📄 1 paper
Abstract
ARTO NCT03449719
ForOligometastatic CRPC, ≤3 nonvisceral mets, on first-line abiraterone
TL;DRPSA response 92% vs 68.3% (OR 5.34) and PFS HR 0.35 adding SBRT to abiraterone in oligomet CRPC.
Surfaced from a review's discussed trials
The whole between-arm benefit is RT-attributable: both arms got abiraterone, so SBRT alone drove complete biochemical response from 23.2% to 56% and PFS HR 0.35 on an active ARSI backbone. Supports offering metastasis-directed SBRT to all oligomet CRPC sites, though source omits dose/fractionation, which gates transfer to practice.
- Extends oligomet MDT paradigm (STOMP, ORIOLE in hormone-sensitive prostate) to the CRPC/ARSI setting
6 details 3 trials watching
- 🔍 Phase II multicenter RCT, N=157 enrolled Jan 2019-Sep 2022, randomized 1:1
- 🔍 Eligibility: oligomet CRPC, ≤3 nonvisceral metastatic lesions; SBRT delivered to ALL sites of disease
- 💊 Both arms receive abiraterone + prednisone, so the between-arm delta is the RT-attributable effect of adding SBRT
- 📊 Outcomes adding SBRT to abiraterone+prednisone (experimental) vs AAP alone (control)
Endpoint SBRT+AAP AAP alone Effect Biochemical response (PSA↓≥50%, 6mo) 92% 68.3% OR 5.34 (2.05-13.88), p=.001 Complete BR (PSA<0.2, 6mo) 56% 23.2% OR 4.22 (2.12-8.38), p<.001 PFS n/a n/a HR 0.35 (0.21-0.57), p<.001
- ⚠️ Primary endpoint is biochemical (PSA ≥50% decline at 6mo), a surrogate; no OS reported in source
- ⚠️ SBRT dose/fractionation and met-site distribution (nodal vs bone) not reported in source, limiting transferability
- OS benefit of adding SBRT in oligomet CRPC unknown n=102 · primary completion 2027-04 · randomized SBRT vs SOC in oligomet CRPCrecruiting Treatment With Darolutamide +/- Radiation Therapy for Patients With a Castration Resistant Cancer and Metastases Detected by Functional Imaging Phase 3n=336 · primary completion 2029-10 · phase 3 darolutamide ± SBRT in CRPC
- Durability of PFS benefit beyond 6-month biochemical readout n=102 · primary completion 2027-04 · endpoint is progression delay in CRPC
- Optimal SBRT dose/fractionation for CRPC oligometastases
📚 Sources · 📄 1 paper
Abstract
WOLVERINE
ForOligometastatic prostate (≤5 mets), 65% castration-sensitive, 85% prior local Rx
TL;DRMDT+SOC cut PFS events vs SOC alone (HR 0.44, p<0.0001) across 6 oligomet prostate RCTs; OS HR 0.63 (p=0.051) not significant.
Surfaced from a review's discussed trials
The RT read is CRFS: MDT delayed castration resistance (HR 0.58), and the sensitivity analysis restricted to active-SOC comparators (dropping observation-only arms) held PFS and CRFS benefit (HR 0.46 each), so adding SBRT to mets earns its place on top of systemic therapy, not just vs surveillance. Per-trial dose and fractionation aren't in source.
- Sensitivity analysis dropping observation-only SOC trials (STOMP, ORIOLE, COMET-SABR): benefit holds vs active SOC
7 details 5 trials watching
- 🔍 IPD meta-analysis (PROSPERO CRD42023479078), 6 randomised phase 2 trials, 472 pts: MDT+SOC 248 vs SOC 224, median f/u 40.7mo
- 🔍 Trials pooled: EXTEND (2 baskets), STOMP, ORIOLE, ARTO, COMET-SABR (16 prostate pts)
- 🔍 65% castration-sensitive (n=375); CRPC enrolled in EXTEND baskets + ARTO; 85.5% had prior definitive local therapy
- 📊 MDT vs SOC efficacy across endpoints (HR, 95% CI, p) — comparison values omitted (cell value "0.0001" not verified in source)
- 📐 rPFS showed moderate inter-trial heterogeneity (I²=50%)
- ⚠️ 'Some concerns' risk of bias across most trials from non-blinded randomisation; open-label PFS open to assessment bias
- ⚠️ OS (coprimary) not significant; every component is phase 2, no level-1 phase 3 evidence yet
- OS benefit unconfirmed; phase 3 trials needed active Prostate-cancer Treatment Using Stereotactic Radiotherapy for Oligometastases Ablation in Hormone-sensitive Patients Phase 3n=550 · primary completion 2026-06 · phase 3 SBRT to all oligomets vs SOC, efficacy 1°recruiting Veterans Affairs Seamless Phase II/III Randomized Trial of STAndard Systemic theRapy With or Without PET-directed Local Therapy for Oligometastatic pRosTate Cancer Phase 2/3n=464 · primary completion 2026-09 · phase 2/3 MDT vs systemic alone, CRPC-free survivalrecruiting Metastasis Directed Stereotactic Body Radiotherapy for Oligo Metastatic Hormone Sensitive Prostate Cancer Phase NAn=118 · primary completion 2031-12 · phase 3 MD-SBRT add-on, failure-free survival 1°
- MDT benefit differs in castration-resistant vs sensitive subsets n=102 · primary completion 2027-04 · phase 2/3 SBRT to eradicate CRPC oligometsrecruiting Treatment With Darolutamide +/- Radiation Therapy for Patients With a Castration Resistant Cancer and Metastases Detected by Functional Imaging Phase 3n=336 · primary completion 2029-10 · phase 3 SBRT +/- darolutamide in CRPC
- Optimal MDT modality, dose, and fractionation across trials
📚 Sources · 📄 1 paper
Abstract
RADIOSA NCT02680587
ForMetachronous oligorecurrent HSPC, ≤3 nodal/bone lesions, post-radical tx
TL;DRcPFS 32.2 vs 15.1mo, HR 0.43 (0.26-0.72), p=0.001 adding 6mo ADT to metastasis-directed SBRT in oligorecurrent HSPC.
Surfaced from a review's discussed trials
The radonc decision is whether to layer 6mo ADT onto metastasis-directed SBRT: doing so roughly doubled cPFS (32.2 vs 15.1mo), but the SBRT-alone arm still held 15.1mo, so an ADT-free interval stays viable in selected pts. Toxicity was near-nil in both arms (one G3 GU event).
- STOMP/ORIOLE tested MDT vs surveillance; RADIOSA instead isolates the added value of 6mo ADT atop a fixed SBRT backbone
8 details 2 trials watching
- 🔍 Randomized open-label phase 2, single-centre (Milan); N=105 (52 vs 53), modified ITT, 51/51 analyzed
- 🔍 SBRT 30Gy/3fx every other day (EQD2 98.6Gy, BED >100Gy, α/β 1.5), or site-equivalent regimens
- 🔍 ADT arm: 6mo LHRH analogue, started ≤1wk before SBRT (short-course, not continuous)
- 🔍 Eligibility + stratification
- ≤3 lesions: pelvic nodal, extra-regional nodal, or bone (next-gen imaging)
- BCR after radical local prostate tx, ECOG 0-1
- Stratified: PSA-DT ≤3 vs >3mo, node vs bone, PET vs MRI
CONSORT flow
- 📊 1° EP clinical PFS by arm — comparison values omitted (cell value "15.1" not verified in source)
- 📊 Toxicity minimal, no treatment-related deaths
- SBRT-attributable: 1 GI G1 (SBRT alone), 1 GU G3 left ureter stenosis (SBRT+ADT)
- No late toxicities in either arm
- ADT-related: 22 G1 AEs, all resolved at last follow-up
- ⚠️ 1° EP clinical PFS, a surrogate; no MFS or OS reported
- ⚠️ Single-centre, open-label, N=105, median f/u 31mo (IQR 16-36); broader confirmation needed
- Optimal duration of ADT added to metastasis-directed SBRT n=873 · primary completion 2027-04 · 1mo vs 6mo short-term ADT added to MDTrecruiting Duration of Androgen Receptor Pathway Inhibitor and ADT With Metastasis Directed Therapy in Oligometastatic Cancer of the Prostate (DIRECT) Phase 2n=132 · primary completion 2031-02 · 8-9mo ARPI added to SBRT+ADT, randomized
- Biomarkers predicting which pts benefit from SBRT alone
- Whether cPFS benefit translates to MFS or OS
📚 Sources · 📄 1 paper
Abstract
EAU 2026: MDT/SBRT in Oligometastatic Prostate Cancer
TL;DRMDT/SBRT delays progression across oligomet prostate states; ARTO first randomized OS signal, WOLVERINE PFS-positive but OS-negative; patient selection the open challenge.
Reported via UroToday →
The actionable RT read is the split OS data: ARTO gives the first randomized signal of an OS and PCSS benefit from MDT, while WOLVERINE improved PFS/rPFS and delayed CRPC but missed OS. SOLAR vs SATURN hints synchronous disease gains more, supporting earlier SBRT in selected low-volume pts.
- SOLAR (synchronous, n=21) vs SATURN (metachronous): ADT-discontinuation after MDT; outcomes favored synchronous disease (hypothesis-generating)
6 details 5 trials watching
- 🔍 EAU 2026 thematic-session review (V. Fonteyne, Ghent): evidence for MDT/SBRT across oligometastatic prostate states
- 🔍 De novo oligo HSPC evidence thin; awaiting STAMPEDE2 (SBRT), PLATON, TERPS, OLIGOPRESTO; LUNAR testing Lu-177 + MDT
- 🔍 PSMA PET burden (PP3) may refine selection beyond the ≤5-lesion cutoff; biomarkers still needed
- 📊 Randomized MDT signals by setting (direction only; no effect sizes reported in source tweets)
- ARTO (oligo-CRPC): MDT added to SOC improved PFS, plus OS and PCSS, the first randomized OS signal for MDT
- WOLVERINE (oligo HSPC): MDT improved PFS/rPFS and delayed CRPC, but no significant OS benefit
- RADIOSA: ADT + MDT improved PFS vs MDT alone
- STOMP / ORIOLE (metachronous HSPC): excellent local control, delayed progression, minimal toxicity
- ⚠️ RAVENS: adding Ra-223 to MDT did not improve PFS or MFS vs MDT alone
- ⚠️ Guideline integration limited by small trials, heterogeneous inclusion criteria and endpoints
- Role of MDT in de novo oligometastatic HSPC active Prostate-cancer Treatment Using Stereotactic Radiotherapy for Oligometastases Ablation in Hormone-sensitive Patients Phase 3n=550 · primary completion 2026-06 · phase 3 SBRT to all oligomets vs SOCrecruiting Veterans Affairs Seamless Phase II/III Randomized Trial of STAndard Systemic theRapy With or Without PET-directed Local Therapy for Oligometastatic pRosTate Cancer Phase 2/3n=464 · primary completion 2026-09 · phase 2/3 PET-directed local therapy, de novorecruiting Comprehensive Versus Primary Tumor Radiotherapy in Oligometastatic Prostate Cancer Phase NAn=390 · primary completion 2027-01 · phase 3 comprehensive vs primary-tumor RT
- Whether radioligand therapy adds benefit to MDT recruiting An Open-label Study Comparing Lutetium (177Lu) Vipivotide Tetraxetan Versus Observation in PSMA Positive OMPC. Phase 3n=450 · primary completion 2028-04 · phase 3 177Lu-PSMA vs observation in OMPC
- Optimal patient selection beyond lesion count recruiting Phase II Non-Randomized Study Evaluating POSLUMA-PSMA PET Response After Oligo- Metastatic/Progressive-directed Treatment With Radiotherapy (PROMPT-R) Phase 2n=50 · primary completion 2028-05 · PSMA-PET + ctDNA to predict progression
📚 Sources · 📄 1 paper
Abstract
2026-06-04 ASCO Annual Meeting 2026
MROQC ADT Practice Patterns
ForHigh-risk localized prostate (GG4-5 dominant), M0/N0-1, definitive RT
TL;DROnly 67% of high-risk RT pts recommended guideline-concordant ADT (≥18mo); ARPI intensification reached 23.2% of STAMPEDE-eligible post-publication, with persistent facility variability.
Facility, not just patient risk, predicted ADT duration (site variability P<.0001): where a high-risk pt is treated shifts whether he gets ≥18mo ADT. The actionable gap is ARPI intensification, recommended in only 23.2% of STAMPEDE-eligible (≥2 risk features) pts. This moves a practice-standardization audit, not an RT technique choice.
- Benchmark: 2022 AUA/ASTRO = 18-36mo ADT; STAMPEDE M0 = add ARPI for ≥2 of cT3/4, GG4-5, PSA≥40, cN1.
8 details 1 trial watching
- 🔍 Prospective practice-patterns analysis, MROQC statewide consortium; 553 high-risk pts, 26 centers, Jun 2020–Nov 2024.
- 🔍 Cohort: intact high-risk M0/N0-1; GG4-5 75.0%, PSA≥20 40.0%, cN1 19.9%, cT3/4 13.3%.
- 📊 ADT recommended in 91.3%; guideline-concordant (≥18mo) in only 67.0% (1° outcome).
- 📊 ARPI intensification in STAMPEDE-eligible (27.9% of cohort): 0% pre-STAMPEDE-M0 → 23.2% after.
- 📐 Predictors of guideline-concordant ADT recommendation (MVA)
Factor OR for GC-ADT (95% CI) GG5 9.45 (4.46-20.06) GG4 6.23 (2.85-13.62) PSA ≥40 3.64 (1.22-10.87) cN1 2.94 (1.44-5.99)
- ⚠️ Facility, not just patient factors, drove recommendations: site variability persisted on MVA (P<.0001).
- ⚠️ Endpoint is intended/recommended ADT, not delivered treatment or outcomes; no survival data.
- ⚠️ One-third of high-risk pts (GG4-5 dominant) recommended <18mo ADT: undertreatment signal vs AUA/ASTRO.
- Optimal ADT duration and ARPI intensification in high-risk RT patients n=2753 · primary completion 2033-12 · high-risk RT, Decipher-gated apalutamide intensification
- Whether intended guideline-concordant ADT translates to delivered care
- Drivers of persistent facility-level variability in ADT recommendations
📚 Sources · 📄 1 paper
Abstract
2026-05-31
COMPPARE
ForDe novo localized prostate cancer, excl very-high-risk and metastatic
TL;DRNo proton advantage over IMRT: bowel urgency 5.7 vs 6%, GI G2+ tox 5.2 vs 5.6%, 3yr biochemical control 98.0 vs 97.9%, all NS.
Not proton vs photon but the rectal spacer is the toxicity lever: it cut 2yr GI G2+ toxicity (4.4% IMRT, 4.7% proton with spacer vs 7.2% and 8.7% without, p=0.009), dwarfing modality. Both arms fell far below hypothesized rates, so paying the proton premium for less GI toxicity isn't supported.
- vs PARTIQoL (randomized proton vs IMRT, localized prostate): concordant null for patient-reported bowel/GI endpoints

| Endpoint | IMRT | Proton | p |
|---|---|---|---|
| Bowel urgency (EPIC) | 6% | 5.7% | 0.28 |
| Bowel frequency (EPIC) | 4% | 3.5% | 0.43 |
| GI tox (CTCAE ≥G2) | 5.6% | 5.2% | 0.60 |
| 3yr freedom from progression | 97.9% | 98.0% | 0.90 |
+1 more figure

| Group | 2yr GI G2+ toxicity (95% CI) |
|---|---|
| IMRT, no spacer | 7.2% (5.0%, 9.9%) |
| Proton, no spacer | 8.7% (5.0%, 14%) |
| IMRT, spacer | 4.4% (2.8%, 6.4%) |
| Proton, spacer | 4.7% (3.6%, 6.0%) |
7 details 4 trials watching
- 🔍 Prospective comparative-effectiveness cohort (non-randomized), PCORI-funded; 51 centers, 2524 accrued Jul 2018–Oct 2022
- 🔍 Cohorts: 1500 proton vs 1000 photon; all de novo localized prostate excl very-high-risk and metastatic
- 📊 Rectal spacer cut 2yr GI G2+ toxicity more than modality choice (p=0.009); proton vs IMRT negligible within spacer strata
- ⚠️ Realized GI/bowel toxicity ~5-6% in both arms, far below the 15-29% hypothesized for IMRT
- ⚠️ Low realized event rates leave the comparison likely underpowered to detect a true proton benefit
- ⚠️ Early results; late GI/GU toxicity (the main proton rationale) and long-term control not yet mature
- ⚠️ Non-randomized cohorts: baseline differences between proton and IMRT pts may confound the read
- Late GI/GU toxicity beyond 3 years for proton vs IMRT active A Prospective Comparative Study of Outcomes With Proton and Photon Radiation in Prostate Cancer Phase NAn=3000 · primary completion 2026-02 · proton vs IMRT toxicity cohort, n=3000n=400 · primary completion 2027-03 · proton vs photon late GI toxicity, high-risk
- Long-term biochemical and disease control with longer follow-up active A Prospective Comparative Study of Outcomes With Proton and Photon Radiation in Prostate Cancer Phase NAn=3000 · primary completion 2026-02 · proton vs IMRT disease-control cohort, n=3000n=303 · primary completion 2026-12 · proton vs IMRT, cancer-control endpoint
📚 Sources · 🐦 1 tweet
#COMPPARE early results: in localized #ProstateCancer, #proton therapy vs #IMRT showed no sig difference in pt-reported bowel urgency/frequency, ≥G2 GI toxicity, or 3-year biochemical control. Longer follow-up needed for late toxicity/long term outcomes #ASCO2026 pic.twitter.com/yli4l8nEOY
— QianJanieQin (@QianJanieQin) May 31, 2026
ENZARAD
ForHigh-risk localised prostate (GS 8-10, T3-4, N1, or PSA≥20), RT-eligible
TL;DRMFS HR 0.88 (0.67-1.15) p=0.34, OS HR 0.87 p=0.40: adding enzalutamide to high-dose RT + 2y ADT did not improve high-risk localised prostate.
The RT read is the pelvic-nodal-RT interaction: enzalutamide helped only pts who received pelvic RT (MFS HR 0.47 vs 1.25 without, interaction p<0.001) and N1 pts (HR 0.43). Hypothesis-generating, but it flags node-positive/whole-pelvis pts as the subgroup where ARSI intensification with definitive RT might still pay off.
- vs EMBARK (enzalutamide in nmHSPC biochemical recurrence): intensification improved MFS there but adds nothing layered on definitive RT + 2y ADT here.
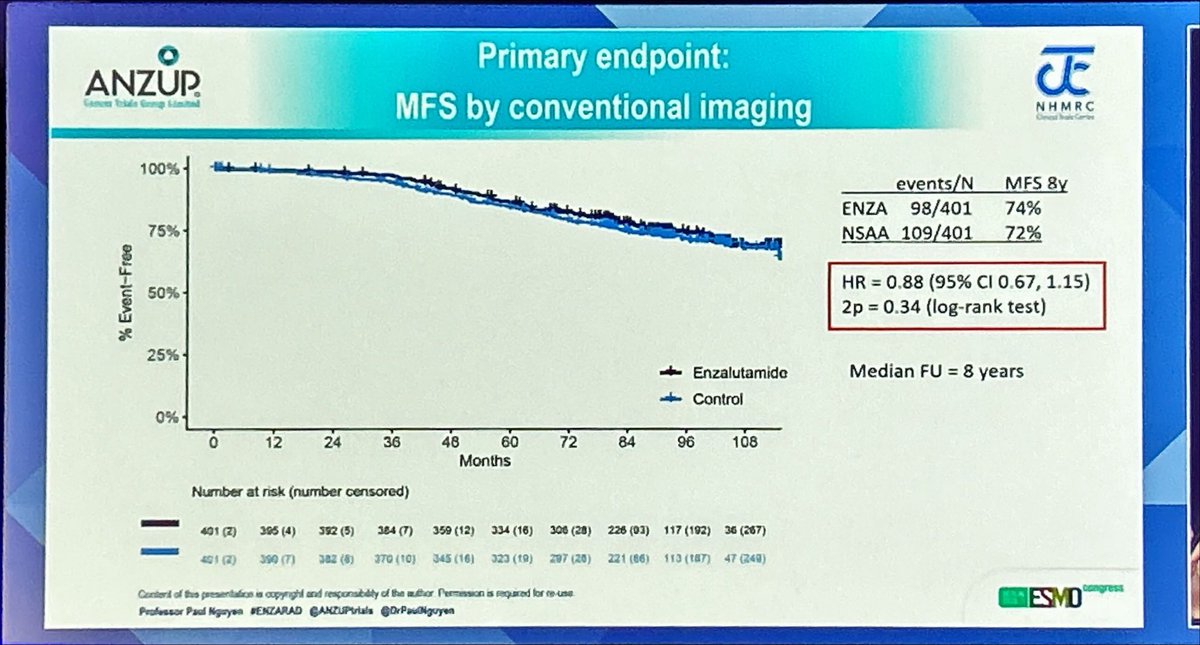
| Arm | MFS events/N | HR (95% CI) | 2p |
|---|---|---|---|
| Enzalutamide | 98/401 | 0.88 (0.67-1.15) | 0.34 |
| Control (NSAA) | 109/401 | ref | — |
+2 more figures
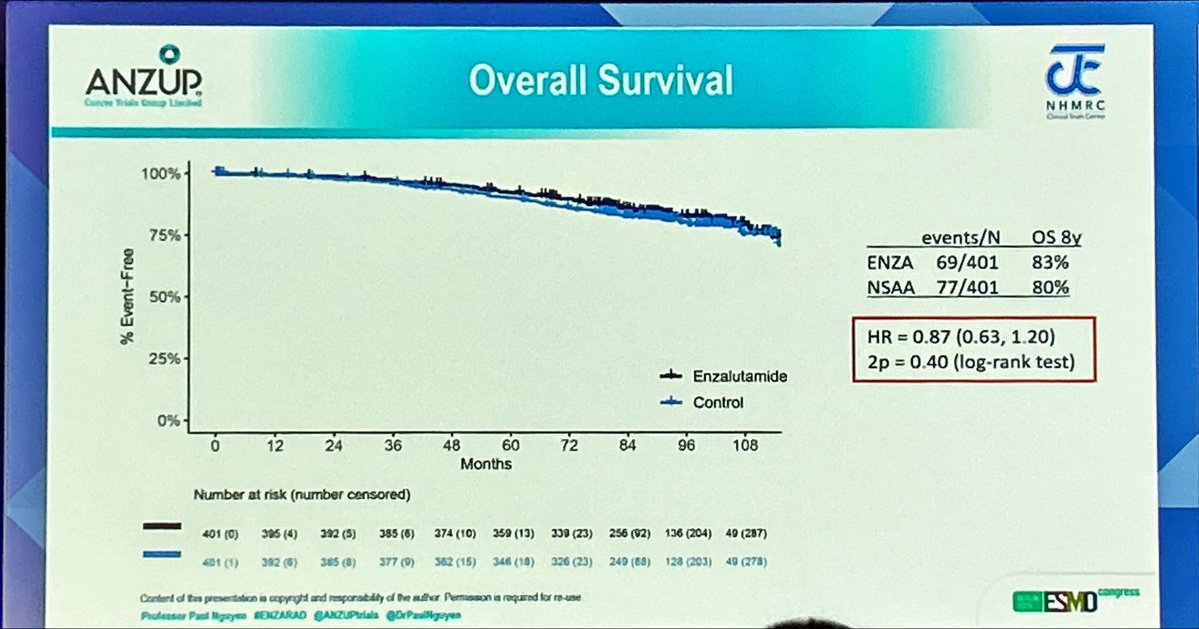
| Arm | OS events/N | OS 8y | HR (95% CI) | 2p |
|---|---|---|---|---|
| Enzalutamide | 69/401 | 83% | 0.87 (0.63-1.20) | 0.40 |
| Control (NSAA) | 77/401 | 80% | ref | — |
7 details 2 trials watching
- 🔍 Phase 3 RCT (ANZUP), N=800, high-risk localised prostate, all RT-treated.
- 🔍 Shared backbone both arms: 2y LHRHa + high-dose EBRT, brachy boost and pelvic nodal RT permitted, RT starting after 16wk.
- 💊 Randomised add-on: enzalutamide 160mg ×24mo vs conventional NSAA ×6mo.
CONSORT flow
- 📊 Negative trial: primary MFS not met and OS not improved at 8y median follow-up.
- 📐 ICECAP surrogacy held: MFS and OS hazard ratios well-correlated in the trial's analysis.
- ⚠️ Benefit seen only in predefined subgroups: cN1 disease and pts receiving pelvic nodal RT (MFS interaction p<0.001 for pelvic RT). Hypothesis-generating.
- ⚠️ Pelvic-RT subgroup reflects treatment received, not randomisation; interaction is exploratory and needs prospective confirmation before changing practice.
- Does ARSI intensification benefit only node-positive or whole-pelvis-RT pts? recruiting Treatment of High-Risk Prostate Cancer Guided by Novel Diagnostic Radio- and Molecular Tracers Phase 2/3n=493 · primary completion 2030-07 · darolutamide + RT, includes cN1 high-riskrecruiting Reduced Length of ADT and ARTA With XRT in High-Risk Prostate Cancer (RELAX): A Randomised Trial Phase 2n=206 · primary completion 2035-01 · ARTA + whole-pelvis RT in high-risk localised
- Confirmatory trial of enzalutamide in cN1 localised prostate needed?
📚 Sources · 🐦 1 tweet
🚨ENZARAD at #ESMO25 presented by @DrPaulNguyen
— Pierre Blanchard, MD (@PBlanchardMD) October 19, 2025
No improvement in MFS or OS with the addition of enzalutamide to high dose radiotherapy + 2y ADT in high risk #prostatecancer
Possible benefit in cN1 pts or pts treated with pelvic RT. pic.twitter.com/vXLRKuIPeg
CAN-2409
ForLocalized prostate cancer, definitive EBRT (78Gy)
TL;DRDFS HR 0.7 (0.52-0.94, p=0.0155), median NR vs 86.1mo, adding intra-prostatic oncolytic virus to definitive 78Gy RT; OS/PCSM immature.
The RT-relevant read is local control: 2yr positive-biopsy fell to 19.6% vs 36.4% (p=0.0015) without dose escalation or added ADT, a new local-intensification lever. But the control RT (78Gy, no boost or ADT) predates modern intensification, leaving its place vs brachy boost or ADT unsettled.
- Local-control gain reached without dose escalation or ADT, a different lever than brachy boost or hormones

| Endpoint | CAN-2409 | Placebo | HR / p |
|---|---|---|---|
| DFS, median | NR | 86.1 mo | HR 0.7 (0.52-0.94), p=0.0155 |
| 2yr biopsy pCR | 80.4% | 63.6% | |
| 2yr +biopsy (local) | 19.6% | 36.4% | p=0.0015 |
| OS | NS | NS | |
| PCSM events | 1 | 1 |
+1 more figure

| Method (trial) | Endpoint | Control | Intensified |
|---|---|---|---|
| +ADT (RTOG 9408) | 2yr +biopsy | 40% | 20% |
| Brachy boost (ASCENDE-RT) | 10y local failure | 7.1% | 1.5% |
| Dose SIB (FLAME) | crude local failure | 7.7% | 2.7% |
| CAN-2409 | 2yr +biopsy | 36.4% | 19.6% |
5 details 1 trial watching
- 🔍 Intra-prostatic oncolytic-viral therapy (CAN-2409) added to definitive EBRT 78Gy, vs RT + placebo, randomized
- 📊 ≥Gr 3 toxicity <1% with CAN-2409 added, no major added RT toxicity
- ⚠️ DFS driven mainly by 2yr post-RT biopsy pCR, a surrogate endpoint
- ⚠️ OS and PCSM still flat, so clinical benefit unproven
- ⚠️ Per discussant: control RT 78Gy lacked modern dose intensification (brachy boost, SIB) or ADT, blunting relevance to current SOC
- Does the DFS benefit translate to OS/PCSM with longer follow-up? active Phase 3 Study of ProstAtak® Immunotherapy With Standard Radiation Therapy for Localized Prostate Cancer Phase 3n=711 · primary completion 2024-08 · phase 3 same virus+RT, n=711, intermediate-high risk
- Does benefit hold against modern dose-escalated RT and ADT?
📚 Sources · 🐦 1 tweet
🗣️Prostate Oral Abstract #ASCO25
— Michael Serzan, MD (@MikeSerzanMD) June 3, 2025
👉Dr @angela_jia_ discusses "Better Treatments, Better Selection: Improving Patient Outcomes in Localized Prostate Cancer"
🔑 KEY TAKE AWAYS
- #CAN2409 improves DFS and 2yr PathCR however PCSM and OS remain immature.
❓How to integrate with… pic.twitter.com/WamsneYBI1
PROTEUS
TL;DRPreview only; most distant mets found by PSMA PET (53.0% apalutamide vs 60.7% ADT), so MFS events were PET- not conventionally-driven.
8 details 1 trial watching
- 🔍 Arms per source: apalutamide + ADT vs ADT alone; endpoints reference EFS, BCR, MFS.
- 🔍 Phase, N, and study population/setting not stated in source tweets.
- 📊 Preview release; primary MFS effect size (HR, medians) not reported in source tweets.
- 📊 Distant mets identified by PSMA PET: 53.0% apalutamide vs 60.7% ADT.
- ⚠️ Majority of MFS events were PET-detected, not conventional imaging, per the NEJM report.
- ⚠️ More-sensitive PSMA PET ascertainment shifts MFS event counts vs conventional-imaging-era trials.
- ⚠️ @seanmmcbride 50 vs 60 BCR/100 figures are a hypothetical thought experiment, not reported results.
- ⚠️ Curator flags as controversial pre-presentation: framed as either homerun or large negative.
- Does the MFS benefit hold when limited to conventional-imaging mets? n=1503 · primary completion 2026-06 · apalutamide MFS by conventional imaging (BICR)
- Will PSMA-PET-defined MFS translate to an OS benefit?
📚 Sources · 🐦 3 tweets
#ASCO26
— Daniel E Spratt (@DrSpratticus) May 31, 2026
The PROTEUS trial results are now online...buckle up as we wait to see the full presentation. This is going to be a trial that is likely highly controversial until the full results are published.
Some may call this a homerun, others may call this the largest negative…
Thought experiment:
— Sean McBride (@seanmmcbride) May 31, 2026
Let's take a very simple hypothetical trial involving 100 patients in the APA arm and 100 patients in the ADT alone arm. Pulling from PROTEUS EFS data, assume that, by 5 years, 60 patients in the ADT arm have had a BCR compared to 50 in the ADT+APA arm.… pic.twitter.com/WJaiDlJnQs
#ASCO26
— Daniel E Spratt (@DrSpratticus) May 31, 2026
Talk about real-time updates. NEJM paper now online and my predictions and inferences appear true.
Majority of MFS events were by PET not conventional imaging. "Most distant metastases were identified by PSMA PET (53.0% of those in the apalutamide group and 60.7% in the… https://t.co/Yz4myY0flq
2026-05-30 ASCO Annual Meeting 2026
A-DREAM (ALLIANCE mAPMS)
FormHSPC, deep responders: PSA<0.2 after 18-24mo ADT + ≥12mo ARPI
TL;DR41% (32/78) remained treatment-free with eugonadal testosterone at 18mo after interrupting ADT+ARPI in deep-responding mHSPC; primary EP met.
- Intermittent-therapy concept echoes SWOG 9346 (intermittent ADT, mHSPC), but here a deeper-response, post-ARPI-intensification population with both agents interrupted.

+2 more figures


8 details 3 trials watching
- 🔍 Single-arm phase 2 (ALLIANCE A-DREAM); N=78 eligible mHSPC, enrolled 07/2022-03/2024. No randomised continuous-therapy comparator.
- 🔍 Deep-responder selection: PSA<0.2 (stable/falling) after 18-24mo ADT + ≥12mo ARPI; 64.9% low-volume (CHAARTED).
- 🔍 Re-initiation triggers: PSA ≥5 ng/mL, radiographic change (PCWG3), or PrCa-related symptoms.
- 🔍 29.5% received radiation to metastatic sites pre-interruption; 51.3% had prior radiation as local therapy.
- 📊 Disposition at 26.9mo median follow-up
- 30 (38.5%) continuing on treatment interruption
- 29 (37.2%) resumed ADT+ARPI per protocol
- 5 (6.4%) resumed before meeting resumption criteria
- 1 (1.3%) died before next treatment (MI)
- ⚠️ 4 of 29 who resumed ADT+ARPI per protocol later progressed (2 rPD, 1 PDu, 1 PET) and discontinued original ARPI.
- ⚠️ Lenient success bar: primary EP read on 80% CI + one-sided p; ~59% did not achieve treatment-free + T-recovery at 18mo.
- ⚠️ Short FU (26.9mo); OS (4/78 events) and rPFS median NE — durability of the off-treatment interval still unknown.
- Does interruption compromise long-term OS vs continuous ADT+ARPI? active A Study of an Intermittent ADT Approach With Apalutamide Monotherapy in Participants With mCSPC Phase 3n=420 · primary completion 2026-10 · phase 3 intermittent apalutamide, PSA<0.2 respondersrecruiting Optimal PSA Triggered Individual Management of Androgen Sensitive Prostate Cancer Phase 2n=160 · primary completion 2030-10 · intermittent relugolix+ARPI, optimal PSA respondersn=1600 · primary completion 2035-05 · phase 3 intermittent vs continuous ADT+ARPI, OS primary
- Biomarkers predicting which deep responders can safely interrupt
- Durability of the treatment-free interval beyond 2 years
📚 Sources · 🐦 1 tweet
Can treatment be safely stopped in selected patients with mHSPC?
— MJosé Juan (@mjuanfi81) May 30, 2026
Phase II A-DREAM trial, 41% of responders remained treatment-free with testosterone recovery 18m after stopping ADT/ARPI. At a median FU of 21 months, 35% of patients required treatment re-initiation.@OncoAlert pic.twitter.com/iW2VDBWWhN
ARACOG (AFT-47)
ForAdvanced prostate cancer on ARSI (mHSPC, mCRPC, or nmCRPC)
TL;DREnzalutamide drove greater 24-wk cognitive decline than darolutamide (MCCD -36.1 vs -15.8, p=0.009) in advanced prostate cancer.
- Direction aligns with darolutamide's low blood-brain-barrier penetration vs enzalutamide (known pharmacology), giving the divergence a mechanistic basis.

| Arm | MCCD median % change (domain) | p |
|---|---|---|
| Darolutamide (n=48) | -15.8 (PALFAM) | 0.009 |
| Enzalutamide (n=47) | -36.1 (SWM) | 0.009 |
+1 more figure

7 details 1 trial watching
- 🔍 Randomized open-label phase 2 (Alliance, AFT-47), N=111 advanced prostate cancer spanning mHSPC, mCRPC, nmCRPC.
- 🔍 1° EP: Maximally Changed Cognitive Domain (MCCD), % change baseline→24wk across 5 remote CANTAB tests (executive function, visual memory, attention, working memory).
- 🔍 Stratified by age (<65 / 65-80 / >80); darolutamide supplied by study, enzalutamide via standard of care; enrolled 8/2021 to 3/2025.
- ⚠️ MCCD picks each arm's worst-hit domain, so the headline numbers reflect different domains (daro PALFAM, enz SWM), not a like-for-like comparison.
- ⚠️ Open-label design; CANTAB is computerized/objective, but expectancy effects on test effort aren't excluded.
- ⚠️ Cognitive surrogate: CANTAB modules are research tools, not for clinical diagnosis (per slide); link to functional decline unestablished.
- ⚠️ 24-wk analysis: daro n=48, enz n=47 (of 111 randomized); crossover pts scored at crossover within their randomized arm.
- Durability of cognitive divergence beyond 24 weeks
- Confirmation in a larger blinded head-to-head
- Whether MCCD differences translate to functional cognitive outcomes n=102 · primary completion 2026-04 · tracks functional + cognitive outcomes on enza/daro
📚 Sources · 🐦 2 tweets
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 Abstract 5005 | ARACOG / AFT-47
Cognitive effects of darolutamide vs enzalutamide
Presented by Alicia K. Morgans, MD, MPH, FASCO@CaPsurvivorship @OncoAlert@ASCO
In prostate cancer, we often discuss AR pathway inhibitors through the lens… pic.twitter.com/vpZr1w6kc6
ARACOG (AFT-47) met its primary endpoint: enzalutamide caused significantly greater cognitive decline than darolutamide at 24 weeks in advanced prostate cancer.
— Katy Beckermann (@katy_beckermann) May 30, 2026
Randomized open-label phase 2, 111 pts (mHSPC, mCRPC, nmCRPC), DAR vs ENZ.
Cognition was measured with CANTAB, a… pic.twitter.com/kj4vfGRVyp
NRG Clinico-Transcriptomic Risk Stratification
ForNCCN high-risk/very-high-risk localized prostate, RT+ADT candidates
TL;DR~¼ of NCCN high-risk pts reclassified when 22-gene GC added to clinical risk; combined score gates RT+ADT vs RT+ADT+AAP intensification.
The actionable question is systemic intensification on a fixed RT+ADT backbone: layering the 22-gene GC (Decipher) on NCCN clinical risk reclassifies ~¼ of high-risk pts, so clinical staging alone misassigns who gets abiraterone. GC is independently prognostic for MFS, DM, and OS (p<0.001).
- Extends prior VHR framework (Spratt et al, JCO 2018) to the modern very-high-risk population

| Endpoint | HR (95% CI) | p |
|---|---|---|
| MFS | 0.53 (0.44-0.64) | <0.0001 |
| OS | 0.60 (0.48-0.73) | <0.0001 |
+2 more figures


7 details 1 trial watching
- 🔍 Clinico-transcriptomic system layers a 22-gene GC (Decipher) on NCCN risk in ≥high-risk localized prostate; RT+ADT is the uniform backbone
- 🔍 Combined score gates systemic intensification on the RT+ADT backbone
- CT HR, ≤2 points: RT+ADT
- CT VHR, ≥3 points: RT+ADT+AAP (abiraterone intensification)
- 📊 22-gene GC independently prognostic for MFS, DM, and OS beyond clinical variables alone (p<0.001)
- 📊 ~¼ of the ≥high-risk population has discordant clinical vs biomarker risk
- 📊 STAMPEDE AAP absolute benefit grows over time: up to ~20% MFS, ~13% OS (Attard, Lancet 2022)
- ⚠️ GC shown prognostic, not predictive: per-stratum AAP benefit is inferred from STAMPEDE, not randomized within GC-defined groups
- ⚠️ Retrospective biomarker model; CT classification not prospectively validated for the intensification decision itself
- Does GC-high risk predict abiraterone benefit, not just prognosis?
- Prospective validation of the clinico-genomic intensification thresholds recruiting Treatment of High-Risk Prostate Cancer Guided by Novel Diagnostic Radio- and Molecular Tracers Phase 2/3n=493 · primary completion 2030-07 · phase 3 RT+ADT±darolutamide intensification by risk
- Can GC-low very-high-risk pts safely omit abiraterone?
📚 Sources · 🐦 2 tweets
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 Abstract 5000 | High-risk prostate cancer
Clinico-transcriptomic risk stratification to guide abiraterone intensification
Presented by Krishnan R. Patel, MD, MHS@Krishnan_Patel@OncoAlert@ASCO
In high-risk localized prostate cancer,… pic.twitter.com/pZSCiTyGB8
#ASCO26 Dr. Patel presented a clinically practical framework integrating NCCN clinical risk + a 22-gene genomic classifier to guide treatment intensification in high-risk localized prostate cancer.
— Julian Chavarriaga (@chavarriagaj) May 30, 2026
Key findings:
🔹 The genomic classifier independently improved prognostic… pic.twitter.com/fRcdTmfBec
GU Biomarkers in Clinical Practice
TL;DRDecipher/clinical-risk discordant in 24% of events; genomic classifiers validated pre-ARPI may not transfer to current ARPI-based SOC.
ENZAMETCHARTED
The portability caveat is the read for anyone using Decipher: it disagreed with clinical risk in 24% of events and was derived in pre-ARPI, tissue-selected subsets (n=427 of 3816). Weigh that before trusting a genomic classifier to gate intensification in current ARPI-based practice.
+1 more figure
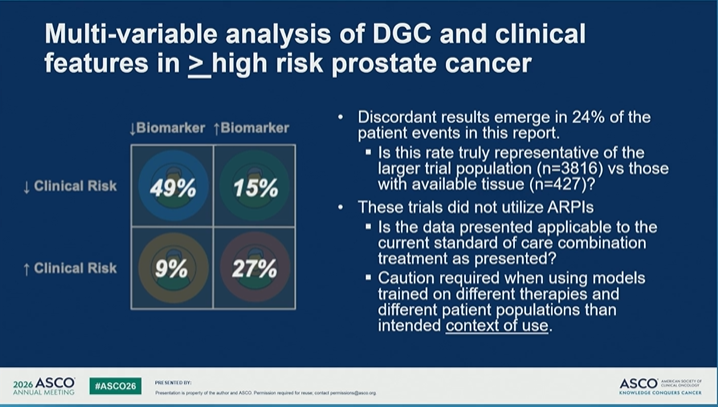
9 details
- 💊 Biomarker-gated therapy fractions, advanced prostate (2026 landscape)
- PARP inhibitors ~10-20% (HRR loss)
- Lu-177 PSMA ~90% (PSMA-avid)
- Pembrolizumab ~3% (MSI-H/dMMR)
- 💊 Tissue panel testing for HRR + tumor-suppressor loss is SOC; 'genomics is not genetics'
- 🔍 ENZAMET biomarker cohort attrition (specimen dropout)
- Enrolled N=1,125
- Consented for biomarker N=1,071
- GEP in CLIA lab N=764
- Final biomarker cohort N=634 (56% of enrolled)
- ADT+enza+docetaxel subcohort N=320
- 🔍 Docetaxel not randomized; protocol amended after 88 pts to allow it per CHARTED
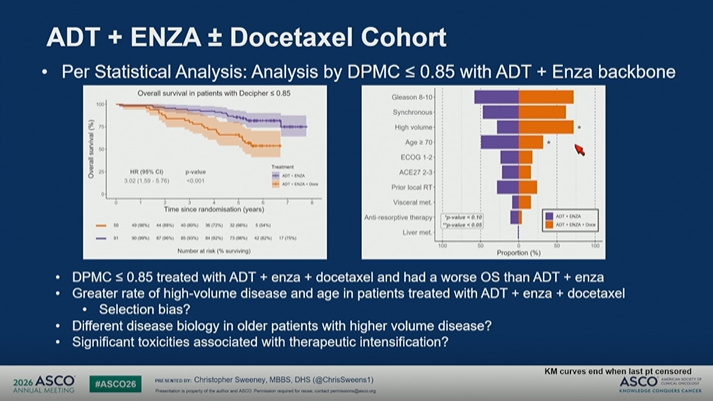
- 📊 Decipher ≤0.85 subgroup: ADT+enza+docetaxel had worse OS than ADT+enza
- ⚠️ Decipher vs clinical risk discordant in 24% of patient events
- ⚠️ Tissue-availability bias: biomarker cohort n=427 vs full trial n=3816
- ⚠️ Docetaxel subgroup confounded: more high-volume disease + older age → selection bias
- 🔬 Theme: applying genomic biomarkers to therapy selection in advanced prostate; only as good as the validation population
- Do genomic classifiers validated pre-ARPI transfer to current ARPI-based SOC?
- Optimal genomic biomarker for systemic intensification in mHSPC
- Does the Decipher ≤0.85 docetaxel-harm signal survive selection-bias adjustment?
📚 Sources · 🐦 1 tweet
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 Precision Oncology: How to Apply New Biomarkers in Clinical Practice
Excellent discussion by Joshua M. Lang, MD, MS@JoshLangMD@OncoAlert@ASCO
This session captured the real challenge of precision oncology in GU cancers:
A biomarker is only… pic.twitter.com/ubfk49XPiM
ENZAMET + Decipher
ForMetastatic hormone-sensitive prostate cancer, Decipher-tested
TL;DRDocetaxel-by-Decipher interaction p=0.04: triplet helps high-Decipher (>0.85) pts (OS HR 0.75) but not low-Decipher (≤0.85, HR 1.94) in mHSPC.
- Decipher >0.85 prognostic for worse OS on ADT+ENZA alone (HR 3.02, 1.50-5.76)
- Framed Level 1B, consistent with CHAARTED and STAMPEDE docetaxel data

| Decipher (doce vs no-doce) | Unweighted HR | IPTW-weighted HR |
|---|---|---|
| ≤0.85 | 2.78 (1.49-5.21), p=0.001 | 1.94 (0.95-3.96), p=0.07 |
| >0.85 | 1.13 (0.71-1.79), p=0.60 | 0.75 (0.43-1.33), p=0.33 |
| Interaction p | 0.02 | 0.04 |
+1 more figure

6 details
- 🔍 Post-hoc Decipher biomarker analysis of ENZAMET; ADT+ENZA+docetaxel cohort N=320, DPMC cutoff 0.85
- 🔍 Docetaxel investigator-allocated within ENZAMET, not randomized; compared by propensity-score (IPTW) weighted MVA
- 📊 Docetaxel benefit confined to high-Decipher (>0.85); low-Decipher pts show none, supporting docetaxel omission
- 📐 MVA covariates: tumor volume, Gleason, synchronous vs metachronous, ECOG, age
- ⚠️ Within-group docetaxel HRs non-significant (CIs cross 1); read rests on the interaction test, not a positive arm
- ⚠️ Residual imbalance after propensity scoring per authors; observational, non-randomized docetaxel comparison
- Prospective validation of Decipher-guided docetaxel intensification in mHSPC
- Whether docetaxel can be safely omitted in low-Decipher pts
📚 Sources · 🐦 1 tweet
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 ENZAMET + Decipher | Part 2
Can genomics guide docetaxel intensification in mHSPC?
Outstanding presentation by @ChrisSweeney1.@OncoAlert@ASCO
After Part 1, the key question was:
➡️ Can a genomic classifier identify which patients with… pic.twitter.com/nJYMxuXelV
TALAPRO-3
For1L metastatic HRR-deficient prostate cancer, castration-sensitive
TL;DR3-yr rPFS 77% vs 56%, HR 0.48 (95% CI 0.36-0.65), p<0.001, adding talazoparib to enza+ADT in HRR-deficient mHSPC.
- vs TALAPRO-2 (1L mCRPC): same talazoparib+enza doublet, now moved earlier into HRR-deficient disease

| Subgroup | Tala 3y rPFS | Placebo 3y rPFS | HR (95% CI) |
|---|---|---|---|
| ITT | 77% (67-85) | 56% (50-62) | 0.48 (0.36-0.65) |
| BRCA | 76% (69-82) | 49% (38-59) | 0.37 (0.22-0.61) |
| Non-BRCA | — | 60% (52-67) | 0.57 (0.39-0.82) |
5 details 1 trial watching
- 🔍 Phase 3 RCT: talazoparib+enza vs placebo+enza, both with ADT; 1L metastatic HRR-deficient prostate cancer; N=599 ITT
- 🔍 Effect gradient by genotype: deepest in BRCA, attenuated but still positive in non-BRCA HRR (CI excludes 1)
CONSORT flow
- 📊 ITT median rPFS NC vs 45.8mo (37.7-NC); 67/300 vs 126/299 events
- ⚠️ rPFS is the surrogate 1° EP; OS not reported in source, follow-up immature (tala median NC in every subgroup)
- ⚠️ Added PARP toxicity (anemia, fatigue) not reported in source; gates the risk/benefit in an earlier, less-symptomatic population
- OS benefit beyond rPFS surrogate
- Benefit by individual non-BRCA HRR gene
- Risk/benefit of added PARP toxicity in HSPC recruiting Presurgical Phase II Study of Talazoparib in Combination With Enzalutamide in Prostate Cancer Phase 2n=30 · primary completion 2026-12 · isolates adding talazoparib to ADT+enza in HSPC
📚 Sources · 🐦 1 tweet
JUST In: TALAPRO-3 published in @NEJM
— Toni Choueiri, MD (@DrChoueiri) May 30, 2026
Adding #talazoparib to enzalutamide/ADT
=>3-year rPFS: 77% vs 56% in HRR-deficient metastatic prostate cancer !
Looking forward to full presentation by @neerajaiims who keeps changing SOC, one trial at a time. @ASCO #ASCO26 @OncoAlert pic.twitter.com/nXiPk4DIXg
2026-05-22
PEACE V–STORM NCT03569241
ForPelvic nodal oligorecurrent prostate ca (≤5 nodes), post radical Rx
TL;DR4yr MFS 76% vs 63% favouring whole-pelvis ENRT over MDT, HR 0·62 (80% CI 0·44–0·86), p=0·063, in nodal oligorecurrence.
Target volume is the decision: whole-pelvis ENRT beat focal MDT on 4-yr MFS (76% vs 63%, HR 0·62), arguing microscopic nodal disease extends beyond the PET-visible node. The cost was modest, G3 urinary incontinence 10% vs 6%. Reason to elect pelvic nodal coverage over node-only SBRT, pending phase 3.
- First RCT in this setting; STOMP/ORIOLE tested MDT vs surveillance, not wider ENRT vs focal MDT
8 details
- 🔍 Phase 2, open-label, randomised 1:1, N=196 (MDT 99 / ENRT 97), 190 evaluable; 21 sites, 6 countries
- 🔍 Population: PET-detected pelvic nodal oligorecurrence (≤5 nodes) post radical local Rx, WHO PS 0–1
- 🔍 ENRT arm: 45 Gy/25 fx to pelvis + SIB 65 Gy to PET-positive nodes (or salvage LND), + 6mo ADT
- 🔍 MDT arm: SBRT 30 Gy/3 fx every other day (or salvage LND), + 6mo ADT
CONSORT flow
- 📊 1° EP metastasis-free survival, ENRT vs MDT
Endpoint MDT ENRT HR (ENRT vs MDT) 4-yr MFS 63% (80% CI 56–69) 76% (80% CI 69–81) 0·62 (80% CI 0·44–0·86), p=0·063 - 📊 Most common grade 3 AEs, MDT vs ENRT — comparison values omitted (cell value "9" not verified in source)
- ⚠️ p=0·063 by conventional two-sided test; positive only under the trial's phase-2 80% CI design. Authors await phase 3
- ⚠️ Both arms permitted salvage LND as the local option, folding surgery into the RT comparison and blurring a clean ENRT-vs-MDT contrast
- Phase 3 confirmation of ENRT MFS benefit over MDT
- OS and long-term QoL of whole-pelvis ENRT vs MDT
- Does PSMA-PET selection change the ENRT vs MDT result
📚 Sources · 📄 1 paper
2026-05-19
ePLND vs PSMA PET staging in prostate cancer (AUA 2026)
TL;DRPSMA PET/CT (NPV ~96%) may safely omit ePLND for nodal staging; ePLND's therapeutic benefit unproven and its morbidity compounds with pelvic RT.
The RT read is compounded morbidity: lymphedema runs 19-29% after PLND plus salvage pelvic RT (2-22% also genital) vs 0-9% for nodal RT alone. With PSMA PET NPV ~96%, omitting ePLND when pelvic nodal RT is anticipated spares that additive toxicity without losing staging confidence.
- RT-relevant: PSMA-PET staging can route to post-op pelvic nodal RT, sparing ePLND and its additive morbidity, especially with no prior eLND (Roberts, PCAN 2024)

+1 more figure

| Setting | Lower-limb lymphedema | Genital lymphedema |
|---|---|---|
| RP + PLND | 0-14% | — |
| Pelvic LN RT | 0-9% | — |
| PLND + salvage pelvic RT | 19-29% | 2-22% |
6 details 4 trials watching
- 🔍 Proposed risk-tiered PLND decision
- Intermediate-risk: omit PLND if PSMA PET LNI-negative; missed LN small, would be missed in ePLND too
- GG3: nomograms add value
- High-risk: individualized; flag that adjuvant/salvage pelvic RT may increase side effects
- 🔍 If PLND is performed, it should be extended (ePLND), per the AUA 2026 message
- 📊 RCTs have not shown consistent BCR improvement from ePLND; provides staging, therapeutic benefit unproven
- 📊 PSMA PET/CT NPV ~96% for nodal disease; a negative scan may safely avoid unnecessary PLND
- ⚠️ PLND morbidity beyond lymphedema: 6-10x increased DVT/PE risk (Tyritzis, 3544 pts RP vs RARP)
- ⚠️ Perspective/review synthesis, not new RCT data; level 1 evidence for ePLND oncological benefit absent
- Oncological benefit of ePLND beyond staging recruiting Extended vs. No Pelvic Lymph Node Dissection During Radical Prostatectomy. DISSECTION 2.0. Phase NAn=400 · primary completion 2027-02 · RCT: extended vs no PLND tests therapeutic benefit
- PSMA PET reliability for nodal staging in high-risk disease recruiting Dutch National Randomized Study: PSMA-PET/CT As a Triage Tool for Pelvic Lymph Node Dissection in Prostatectomy Patients Phase NAn=706 · primary completion 2025-07 · RCT: PSMA PET triages ePLND, comparable prognosisrecruiting Accuracy of 18F-rhPSMA-7.3 PET/ MRI for Prediction of Lymph Node Metastasis in Localized High-Risk Prostate Cancer Phase NAn=50 · primary completion 2027-05 · PSMA PET/MRI accuracy vs PLND for LN mets, high-riskrecruiting Preoperative PSMA PET/CT As Triage for EPLND in Patients Scheduled for RALP (PrePSMA) Phase NAn=600 · primary completion 2029-12 · tests if PSMA PET can replace ePLND for staging
📚 Sources · 🐦 1 tweet
At #AUA2026, the message was clear:⁰📌 ePLND provides staging information, but its therapeutic benefit remains uncertain.⁰📌 RCTs have not shown consistent improvements in BCR outcomes.⁰📌 PSMA PET/CT has a high NPV (~96%) and may safely avoid unnecessary PLND in… pic.twitter.com/7vJFe2hG77
— DR CARVAJAL (@RomanCarvajal) May 17, 2026
2026-05-18
PEACE 2
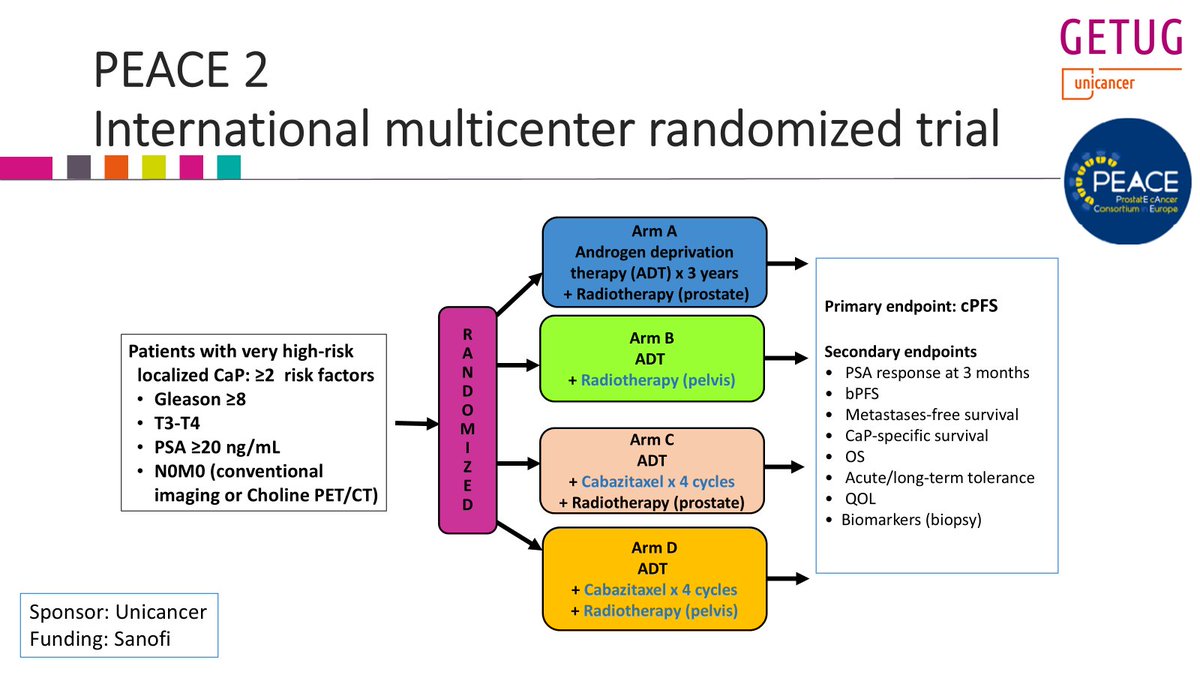
ForVery high-risk localized N0M0 prostate, conventional/choline staging, ≥2 risk fa
TL;DRPelvic RT missed 1° EP cPFS (HR 0.81, p=0.088) in very high-risk N0M0 prostate; no MFS, OS, or PCSS benefit.
The decision is elective pelvic nodal coverage in conventionally-staged very-high-risk N0M0 disease: don't add it. The non-significant cPFS trend (p=0.088) rests on the softest endpoint while MFS, OS, and PCSS are flat. Staging was conventional/choline, not PSMA, so PSMA-selected pts (cf. POP-RT) stay an open question.
- vs POP-RT (JCO 2021): whole-pelvis RT improved biochemical control in high-risk N0; PEACE 2 null. Key difference: POP-RT enriched with PSMA/choline staging and a nodal boost

| Arm | 7yr cPFS | HR (95% CI) | p |
|---|---|---|---|
| Pelvic RT | 67.1% (61.6-72.2) | 0.81 (0.63-1.03) | 0.088 |
| Prostate-only RT | 62.9% (57.4-68.1) | ref | n/a |
+1 more figure
8 details 1 trial watching
- 🔍 Phase III 2×2 factorial (±pelvic RT × ±cabazitaxel); pelvic-RT axis analyzed here, 761 at risk (380 prostate-only vs 381 pelvic)
- 🔍 Pts: very high-risk localized N0M0, ≥2 of Gleason ≥8, T3-T4, PSA ≥20; staged by conventional imaging or choline PET/CT
- 💊 All arms: ADT ×3yr + high-dose prostate RT; the pelvic axis adds elective whole-pelvis nodal volume
- 🔍 Author reports minimal added toxicity from pelvic nodal RT with modern technique (no effect size reported in source)
CONSORT flow
- 📊 1° EP cPFS not met: pelvic RT gave only a non-significant trend (p=0.088)
- ⚠️ No pelvic-RT effect on the hard endpoints MFS, OS, or PCSS (effect sizes not reported in source)
- ⚠️ Even the favorable direction sits on cPFS, the softest endpoint; the clinically meaningful endpoints are flat
- ⚠️ Conventional/choline staging may miss occult PSMA-avid nodal disease, diluting any pelvic-RT signal
- Does whole-pelvis RT benefit PSMA-PET-staged node-negative pts? n=250 · primary completion 2031-05 · WPRT vs prostate-only RT in PSMA-N0M0 high-risk
- Did cabazitaxel add benefit in the factorial's systemic axis?
📚 Sources · 🐦 1 tweet
Yesterday, I presented the @GETUG_Unicancer PEACE 2 trial at #ESTRO26 on the role of pelvic RT in very high risk #prostatecancer pts (staged with conventional imaging).
— Pierre Blanchard, MD (@PBlanchardMD) May 18, 2026
Twittorial below
Key conclusion: pelvic RT did not improve clinical outcomes (cPFS, MFS, PCSS, OS)...
1/n pic.twitter.com/ZKRt2QZzt1
HEAT Trial NCT01794403
ForLocalized low- to intermediate-risk prostate, IPSS <12
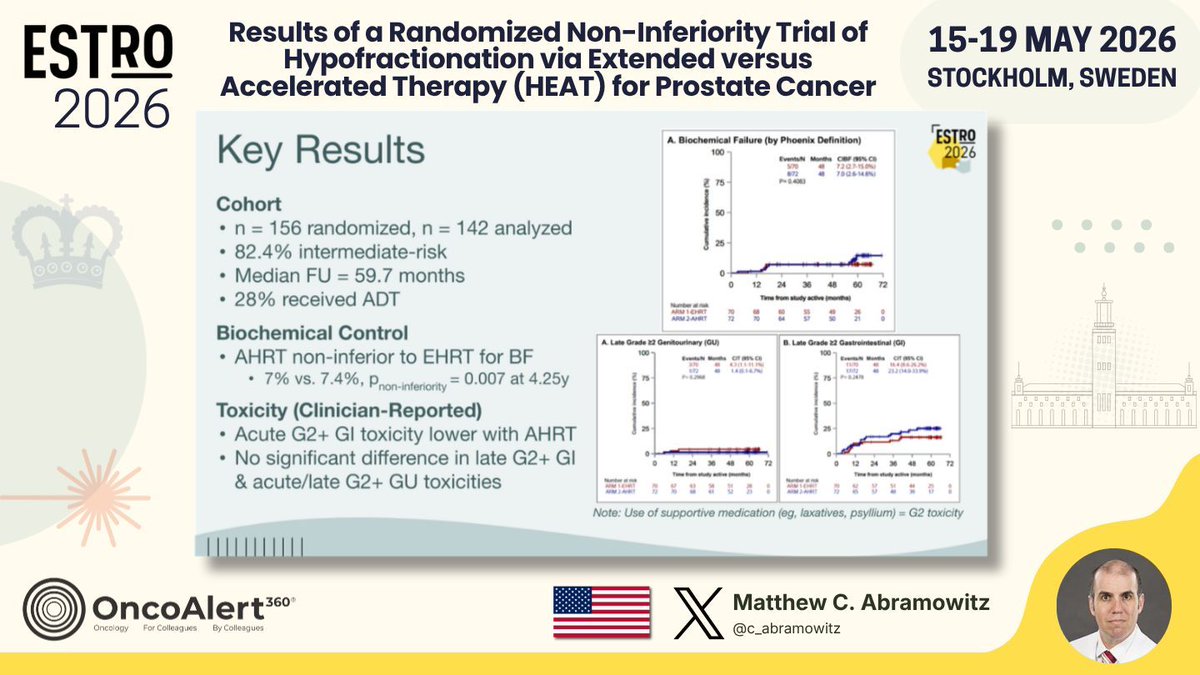
TL;DRAHRT (5 fx SBRT) non-inferior to EHRT (26 fx IMRT) for biochemical failure: 7% vs 7.4%, P=0.007 at 4.25y in localized low-int-risk PCa.
The RT read is toxicity, not just equivalence: acute G2+ GI was lower with 5 fx AHRT despite a GTV SIB to 40 Gy, with no late GI or GU penalty vs 26 fx EHRT. For low- to int-risk PCa weighing 5 vs 26 fractions, this backs SBRT on access without a control or toxicity cost. ADT was permitted (28%), unlike PACE-B and HYPO-RT-PC.
- Unlike HYPO-RT-PC, PACE-B, NRG-GU005 (all barred ADT), HEAT permitted ≤6 mo ADT
| Endpoint | AHRT | EHRT | P (NI) |
|---|---|---|---|
| Biochemical failure, 4.25y | 7% | 7.4% | 0.007 |
+1 more figure
8 details 5 trials watching
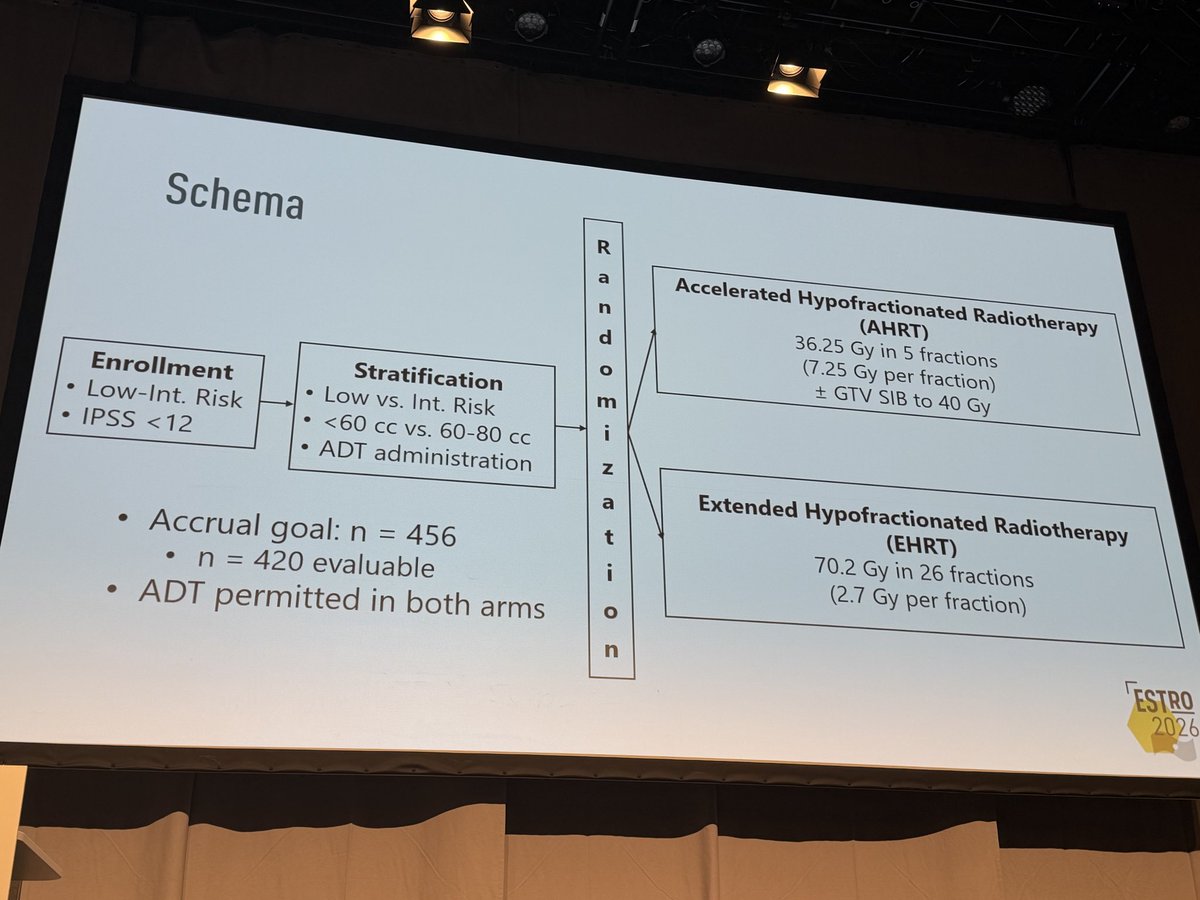
- 🔍 First randomized phase III comparing AHRT (5 fx) vs EHRT (26 fx) head-to-head 1:1, modern IMRT + ADT permitted
- 🔍 Eligibility: localized low- to intermediate-risk PCa, IPSS <12
- 🔍 Cohort characteristics
- 82.4% intermediate-risk
- Median follow-up 59.7 mo
- 28% received ADT (≤6 mo permitted both arms)
- 📊 Acute G2+ GI toxicity lower with AHRT vs EHRT
- 📊 No significant difference in late G2+ GI or acute/late G2+ GU
- ⚠️ Interim analysis: 142 analyzed vs accrual goal 456 (420 evaluable), well short of full accrual
- ⚠️ Supportive meds (laxatives, psyllium) counted as G2 toxicity, inflating reported GI rates
- ⚠️ Wide 12% non-inferiority margin (Phoenix BF) could mask a clinically meaningful difference
- Durability of non-inferiority at full accrual (n=456) and longer follow-up recruiting Two-fraction Versus Five-fraction Stereotactic Radiotherapy for Localized Prostate Cancer Phase NAn=562 · primary completion 2027-12 · RCT 2-fx vs 5-fx SBRT, low/fav int-risk localized
- Generalizability to high-risk or larger-volume (>80cc) prostate recruiting Standard Moderately Hypofractionated RT vs. Ultra-hypofractionated Focal Lesion Ablative Microboost in Prostate Cancer Phase NAn=484 · primary completion 2032-01 · RCT ultra-hypofx vs moderate, int/high-riskn=49 · primary completion 2032-05 · SBRT+ADT cohort, organ-confined high-risk PCarecruiting Androgen Suppression Combined With Nodal Irradiation and Dose Escalated Prostate Treatment Phase 3n=710 · primary completion 2032-10 · phase 3 SBRT vs brachy boost, unfavourable riskrecruiting Phase III Adaptive Adaptive Stereostactic Body Radiotherapy (SBRT) With Dose Escalation for High-Risk Prostate Cancer Phase NAn=390 · primary completion 2033-04 · phase 3 SBRT dose escalation, high-risk PCa
📚 Sources · 🐦 2 tweets
Day FOUR of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 18, 2026
Results of a Randomized Non-Inferiority Trial of Hypofractionation via Extended versus Accelerated Therapy (HEAT) for Prostate Cancer Presented by Matthew C. Abramowitz🇺🇸 #RadOnc ☢️ #ProstateCancer
HEAT is an international phase… pic.twitter.com/IkSTgQHwXK
The HEAT trial is another randomized demonstration of the safety & efficacy of SBRT compared to hypofractionted RT in #prostatecancer at #ESTRO26 pic.twitter.com/c9sNb3KOqo
— Pierre Blanchard, MD (@PBlanchardMD) May 18, 2026
2026-05-17
PRIME Trial NCT03561961
ForHigh-risk or node-positive non-metastatic prostate cancer, long-course ADT
TL;DRInterim 1-2y: 5fx SBRT (36.25Gy) shows no inferiority signal vs 25fx (68Gy), both with whole-pelvis RT + ADT; G3+ tox <1% both arms.
The novel move is whole-pelvis nodal RT compressed to 5 fractions (25 Gy/5fx, SIB to involved nodes) in node+/high-risk disease, where HYPO-RT-PC stopped at prostate-only node-negative. Interim grade 3+ GU/GI <1% is the reassuring safety read; BFFS is too immature to commit to nodal SBRT yet.
- vs HYPO-RT-PC: PRIME extends 5fx ultra-hypofx to node+ disease with whole-pelvis RT + ADT; HYPO-RT-PC was node-neg, prostate-only, no ADT

+1 more figure

8 details 5 trials watching
- 🔍 Phase III open-label non-inferiority, N≈434, randomized 1:1 stratified by risk group + nodal status (Tata Memorial Centre)
- 🔍 Eligibility: high-risk, very-high-risk and/or node-positive non-metastatic prostate cancer; ECOG 0-2; PSMA PET/CT staging allowed
- 🔍 Both arms: prostate + whole-pelvis (elective nodal) RT plus long-course ADT (~2y); SIB to involved nodes allowed in SBRT arm
- 📊 Dose / fractionation by arm (both deliver whole-pelvis RT)
Arm Prostate Pelvic nodes Schedule SBRT 36.25 Gy/5fx (7.25 Gy/fx) 25 Gy/5fx every other day Mod hypo ~68 Gy/25fx (2.7 Gy/fx) 25 Gy/5fx ~5 wks, 5 fx/wk - 📊 1° EP BFFS (Phoenix nadir+2): interim 1-2y shows no inferiority signal for SBRT; mature 4-5y data pending
- 📊 MFS and OS: no difference in early analysis, both immature
- 📊 Toxicity (Grade ≥2) by arm, interim — all differences NS
Toxicity G≥2 SBRT 5fx Mod 25fx Acute GU ~5.4% ~4.0% Acute GI ~2.2% ~3.7% Late GU 10-12% 9-11% Late GI 5-7% 4-6% Grade 3+ GU/GI <1% <1%
- ⚠️ Interim safety/early-efficacy only; non-inferiority NOT established with 1-2y f/u and immature BFFS curves
- Mature 4-5y BFFS non-inferiority of 5-fraction SBRT n=120 · primary completion 2027-12 · randomized conventional pelvic IMRT vs SBRT, high-riskrecruiting Androgen Suppression Combined With Nodal Irradiation and Dose Escalated Prostate Treatment Phase 3n=710 · primary completion 2032-10 · phase 3 SBRT vs EBRT+brachy boost, +nodal RT/ADT
- Late GU/GI toxicity of nodal SBRT beyond 2 years recruiting A Trial of 5 Fraction Prostate SBRT Versus 5 Fraction Prostate and Pelvic Nodal SBRT Phase 3n=1128 · primary completion 2028-06 · 5fx: pelvic nodal vs prostate-only SBRT, safety
- Optimal pelvic nodal dose and SIB in 5-fraction regimens n=28 · primary completion 2025-10 · whole-pelvis SBRT + SIB, grade≥3 GU/GI endpointrecruiting A Trial of 5 Fraction Prostate SBRT Versus 5 Fraction Prostate and Pelvic Nodal SBRT Phase 3n=1128 · primary completion 2028-06 · 5fx ± pelvic nodal SBRT, isolates nodal dose
📚 Sources · 🐦 1 tweet
PRIME trial
— Rohit Malde (@roxboxfix) May 18, 2026
Can we safely deliver ultra-short SBRT including pelvic nodal irradiation in biologically aggressive disease treated with ADT?
With Pelvic RT
Moderate hypofractionation:
~68 Gy/25#/5w
Vs
Extreme hypofractionation/SBRT:
36.25 Gy / 5 # /1-2w
Compare HYPO RT PC pic.twitter.com/7NABknLsD5
PIVOTALboost
ForLocalised prostate cancer, high-risk predominant
TL;DRLate G2+ bowel 6.5% with pelvic-node RT + focal boost vs 8.2% prostate-only (20fx IMRT); early bowel excess resolved by 18wk.
Reassurance sits in the nodal arm: whole-pelvis RT + focal boost in 20fx gave late G2+ bowel 6.5%, bladder 16.5%, the lowest of three arms, not a penalty. The early nodal-RT bowel excess resolved by 18wk. Toxicity no longer gates adding elective nodal coverage; the biochemical-control primary endpoint is still pending.
- vs FLAME (JCO 2021): focal boost improved biochemical control without added late toxicity in conventional fractionation; PIVOTALboost tests the same boost concept in 20fx
- vs POP-RT (JCO 2021): prophylactic whole-pelvis RT improved bPFS in high-risk prostate; here the added pelvic RT looks tolerable at 2yr

| Arm (2yr G2+) | Bowel | Bladder |
|---|---|---|
| Prostate (n=281) | 8.2% (5.7-11.7) | 19.5% (15.5-24.4) |
| Prostate+Boost (n=345) | 8.7% (6.3-12.1) | 24.1% (20.2-28.7) |
| Prostate+Nodes+Boost (n=347) | 6.5% (4.5-9.5) | 16.5% (13.1-20.6) |
6 details 5 trials watching
- 🔍 Phase 3 RCT, N=1465 randomised at 39 UK centres; 3 arms, all 20-fraction IMRT
- P: prostate IMRT alone (388 received)
- P+B: + focal prostate boost (464 received)
- PPN+B: + pelvic-node IMRT + focal boost (462 received)
- 🔍 20-fraction moderately hypofractionated IMRT with focal boost to the dominant intraprostatic lesion; dose in Gy not reported in source
- 📊 Pelvic-node RT raised early (<18wk) bowel side effects; the excess resolved by 18 weeks post-RT
- 📊 Late (2yr) G2+ bowel and bladder not increased by nodal RT or boost; PPN+B arm numerically lowest of the three
- ⚠️ Toxicity-only secondary analysis; primary endpoint (biochemical/clinical failure) not reported here, so efficacy of boost + nodal RT stays unproven
- ⚠️ 'Preliminary' late data: only 973/1314 (74%) have ≥2yr follow-up; late toxicity could still rise with maturity
- Does focal boost + pelvic-node RT improve biochemical control in 20-fraction prostate RT? n=18 · primary completion 2026-08 · 20fx pelvic nodal RT + prostate SIB boostrecruiting High-dose Brachytherapy Boost With Stereostatic Body Radiation Therapy to Intermediate or Higher Risk Prostate Cancer Phase NAn=53 · primary completion 2026-10 · HDR brachy boost + SBRT to prostate + pelvic nodesrecruiting Tumor-directed Radiation Therapy for Patients With the Highest Risk Category of Localized Prostate Cancer Phase NAn=76 · primary completion 2031-09 · ultra-hypofx boost + pelvic node RT, high-riskrecruiting Standard Moderately Hypofractionated RT vs. Ultra-hypofractionated Focal Lesion Ablative Microboost in Prostate Cancer Phase NAn=484 · primary completion 2032-01 · 20fx standard vs focal microboost, efficacyrecruiting Androgen Suppression Combined With Nodal Irradiation and Dose Escalated Prostate Treatment Phase 3n=710 · primary completion 2032-10 · phase 3 dose-escalated boost + nodal RT
- Durability of late GU/GI toxicity beyond 2 years
📚 Sources · 🐦 1 tweet
Day THREE of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 17, 2026
Moderately fractionated prostate radiotherapy with a focal boost: acute and preliminary late side effects from the phase 3 PIVOTALboost trial Presented by Isabel Syndikus 🇬🇧 #RadOnc ☢️
In the PIVOTALboost trial, we treated 1314… pic.twitter.com/cGuR1j2Qos
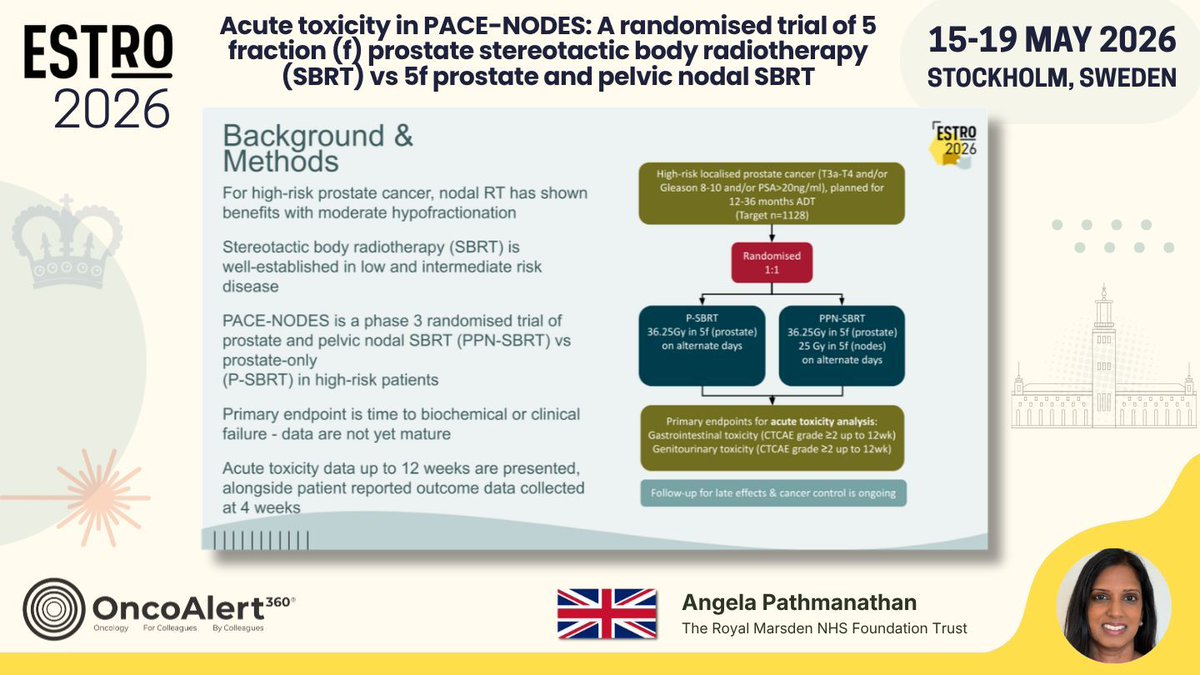
PACE-NODES
ForHigh-risk localised prostate (T3a-T4, Gleason 8-10, or PSA>20), 12-36mo ADT
TL;DRAcute GI CTCAE ≥2 28% vs 21% adding pelvic-nodal vs prostate-only 5fx SBRT, transient; no GU difference; efficacy not yet mature.
The deliverability signal gates adoption: 11% of PPN-SBRT pts didn't receive their allocation (vs 4% prostate-only), mostly unmet dose constraints, so 5fx whole-pelvis SBRT isn't a drop-in for every high-risk case. The GI excess (28% vs 21%) was transient and GU was untouched, but cancer-control data remain pending before adding nodal coverage at this fractionation.
- Nodal RT benefit shown with moderate hypofractionation (POP-RT); PACE-NODES tests whether 5fx nodal SBRT delivers it as safely

| Arm | GI CTCAE ≥2 (12wk) |
|---|---|
| PPN-SBRT | 28% |
| P-SBRT | 21% |
+1 more figure
| Arm | Prostate | Nodes |
|---|---|---|
| P-SBRT | 36.25Gy/5f | — |
| PPN-SBRT | 36.25Gy/5f | 25Gy/5f |
7 details 4 trials watching
- 🔍 Phase 3 RCT, 1166 randomised 1:1 (target 1128), UK multicentre
- 🔍 Eligibility: high-risk localised (T3a-T4, Gleason 8-10, or PSA>20), planned 12-36mo ADT
- 📊 EPIC-26 bowel domain worse with PPN at 4wk, PRO mirrors the clinician GI signal
- 📊 No difference in acute GU toxicity, clinician- or patient-reported
- ⚠️ GI excess was transient: resolved by 12wk, no between-arm difference at that timepoint
- ⚠️ Feasibility gap: 11% PPN-SBRT vs 4% P-SBRT unallocated, mostly unmet dose constraints
- ⚠️ Acute-toxicity readout only; 1° efficacy endpoint (time to biochemical/clinical failure) not yet mature
- Does adding pelvic nodal SBRT improve biochemical/clinical failure? recruiting A Trial of 5 Fraction Prostate SBRT Versus 5 Fraction Prostate and Pelvic Nodal SBRT Phase 3n=1128 · primary completion 2028-06 · phase 3 prostate vs prostate+nodal 5fx, efficacy EPrecruiting PRO-BOOST-N: Prostate-First Versus Combined Prostate and Nodal Dose Escalation in PSMA PET-Staged Node-Positive Prostate Cancer Phase 2/3n=1600 · primary completion 2033-12 · cN1: prostate-only vs added nodal dose escalation
- Late GI/GU toxicity of 5-fraction nodal SBRT not yet Weekly Online CT or MR Adaptive Definitive SBRT for Very High Risk Localized or Regionally Metastatic Prostate Cancer Phase NAn=54 · primary completion 2028-07 · 5x5Gy prostate + elective pelvic nodes, cN0/cN1n=90 · primary completion 2029-04 · 1° EP digestive+urinary toxicity, pelvic 5fx
- Nodal dose constraints driving unmet allocation in PPN arm
📚 Sources · 🐦 1 tweet
Day THREE of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 17, 2026
Acute toxicity in PACE-NODES: A randomised trial of 5 fraction (f) prostate stereotactic body radiotherapy (SBRT) vs 5f prostate and pelvic nodal SBRT
Presented by Angela Pathmanathan 🇬🇧 #RadOnc ☢️ #ProstateCancer
PACE-NODES is a… pic.twitter.com/z9bAOiKSIy
PEACE-2
ForVery high-risk localized prostate (N0M0), ≥2 of Gleason ≥8/T3-T4/PSA ≥20
TL;DRWhole-pelvis RT null vs prostate-only in very high-risk N0M0: cPFS HR 0.81 (p=0.088), bPFS HR 0.97, MFS HR 0.93, no added toxicity.
The WPRT decision: PEACE-2 is null on cPFS (67.1% vs 62.9% at 7y, HR 0.81, p=0.088), bPFS and MFS, where POP-RT was strongly positive. With 3yr ADT, dose-escalated IMRT and modern staging, the incremental value of elective pelvic nodal RT looks small and non-significant, reopening whether routine whole-pelvis RT is needed in N0M0 very-high-risk disease.
- Why PEACE-2 diverges from POP-RT (where WPRT was significantly positive)

| Endpoint | Prostate-only | Pelvic RT | HR (95% CI), p |
|---|---|---|---|
| 7yr cPFS | 62.9% (57.4-68.1) | 67.1% (61.6-72.2) | 0.81 (0.63-1.03), p=0.088 |
+2 more figures

| Endpoint | POP-RT HR (95% CI), p | PEACE-2 HR (95% CI), p |
|---|---|---|
| bFFS/bPFS | 0.50 (0.42-0.61), p<0.001 | 0.97 (0.81-1.16), p=0.73 |
| cFFS/cPFS | 0.74 (0.61-0.90), p=0.002 | 0.81 (0.63-1.03), p=0.09 |
| MFS | 0.72 (0.58-0.89), p=0.002 | 0.93 (0.74-1.17), p=0.54 |

7 details 1 trial watching
- 🔍 Phase III RCT, 2×2 factorial (±cabazitaxel × prostate-only vs pelvic RT); this readout = the pelvic-RT axis only, cabazitaxel axis not reported in source
- 🔍 Eligibility: very high-risk localized N0M0, ≥2 of Gleason ≥8 / T3-T4 / PSA ≥20; staged by conventional imaging or choline PET/CT
- 🔍 RT: dose-escalated IMRT, whole pelvis + prostate boost (prostate 78 Gy EQD2) vs prostate-only IMRT
- 💊 3yr ADT (GnRH analog + antiandrogen) across all arms
- 📊 No additional toxicity with whole-pelvis RT; comparable grade ≥2 GU between arms
- ⚠️ Source labels this an interim analysis (~5.5yr median f/u); cPFS p=0.088 is borderline and could shift with longer follow-up
- ⚠️ Investigators: <1 in 10 men died of prostate cancer in decade 1, challenging the 'very high-risk' label, esp. with negative modern imaging
- Does longer follow-up change the borderline cPFS signal?
- Biomarkers to select very-high-risk men benefiting from pelvic nodal RT
- Does the cabazitaxel axis alter the pelvic RT benefit? active A Phase III of Cabazitaxel and Pelvic Radiotherapy in Localized Prostate Cancer and High-risk Features of Relapse Phase 3n=761 · primary completion 2025-12 · phase 3 cabazitaxel x pelvic RT, 2x2 factorial
📚 Sources · 🐦 2 tweets
POP RT Vs PEACE II
— Rohit Malde (@roxboxfix) May 18, 2026
2 years ADT + WPRT
Vs 3 years ADT + Prostate Only RT
Tough to choose or you already have a choice ?? pic.twitter.com/42kdSKQYKW
📣@PBlanchardMD shows #ESTRO26 that pelvic #radiotherapy in high risk #prostatecancer does not have a large improve in outcomes.
— Shankar Siva (@_ShankarSiva) May 17, 2026
- With only 1 in 10 dying of prostate cancer in 10 years, are these patients truly “high risk”? #pcsm #radonc pic.twitter.com/D0XrGD6iNX
RADIOSA
ForOligorecurrent hormone-sensitive prostate cancer, SBRT candidate
TL;DR61% lower metastatic-progression risk with SBRT + 6-mo ADT vs SBRT alone (HR 0.39, 95% CI 0.22-0.69) in oligorecurrent prostate; mMFS 16.6mo vs not reached.
The additive read is eugonadal MFS: the benefit persisted after testosterone recovery (p<0.05), so the 61% MFS gain (HR 0.39) outlasts pharmacologic castration rather than being a transient on-treatment ADT effect. Moves the decision to add 6-mo ADT to metastasis-directed SBRT in oligorecurrent prostate cancer.
- STOMP/ORIOLE established MDT delays progression vs surveillance; RADIOSA tests adding short-term ADT to SBRT

| Arm | Met progression | Median MFS |
|---|---|---|
| SBRT (A) | 32/51 (62.7%) | 16.6 mo (95% CI 12.83-NA) |
| SBRT + ADT (B) | 19/51 (37.3%) | Not reached |
7 details 3 trials watching
- 🔍 Phase II RCT, N=102 randomized 1:1; oligorecurrent prostate cancer; Arm A SBRT alone vs Arm B SBRT + 6-mo ADT
- 🔍 Median f/u (reverse KM) 49.23 mo (95% CI 42.47-54.8)
CONSORT flow
- 📐 HR 0.3894 (95% CI 0.2201-0.6888), p=0.00119; log-rank p=0.00079 (61% lower metastatic-progression risk)
- 📊 Eugonadal MFS (from testosterone recovery) longer in Arm B (p<0.05); all but 2 Arm B pts recovered testosterone
- ⚠️ Post-hoc analysis; MFS and eugonadal MFS were not the trial's prespecified primary endpoint
- ⚠️ MFS is a surrogate, not OS; N=102 phase II, underpowered for a definitive MFS effect
- ⚠️ Eugonadal MFS is a non-standard, post-hoc-defined endpoint; 'durable synergy' read is hypothesis-generating
- Does the MFS benefit translate to overall survival?
- Optimal ADT duration added to metastasis-directed SBRT recruiting Duration of Androgen Receptor Pathway Inhibitor and ADT With Metastasis Directed Therapy in Oligometastatic Cancer of the Prostate (DIRECT) Phase 2n=132 · primary completion 2031-02 · ARPI duration added to MDT + ADT, randomized
- Phase III confirmation in oligorecurrent prostate cancer active Prostate-cancer Treatment Using Stereotactic Radiotherapy for Oligometastases Ablation in Hormone-sensitive Patients Phase 3n=550 · primary completion 2026-06 · phase 3 randomized SBRT in oligomet HSPCrecruiting Metastasis Directed Stereotactic Body Radiotherapy for Oligo Metastatic Hormone Sensitive Prostate Cancer Phase NAn=118 · primary completion 2031-12 · phase 3 MD-SBRT vs standard, recurrent HSPC
📚 Sources · 🐦 1 tweet
Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 16, 2026
Post-hoc analysis of metastasis-free survival (MFS) and Eugonadal MFS in the RADIOSA phase II randomized trial Presented by Giulia Marvaso 🇮🇹 #RadOnc ☢️ @giuliamarvaso84
Post-hoc analysis of RADIOSA shows SBRT plus short-term ADT… pic.twitter.com/1zpiChkUgA