Bladder
2026-06-29
BART
ForHigh-risk pT3-4/N+/R+ MIBC, post-radical cystectomy + chemo
TL;DR2-yr locoregional FFS 87.1% vs 76.0% (HR 0.43, p=0.04) favoring adjuvant RT post-cystectomy; OS not significant.
Reported via UroToday →
The RT decision is adjuvant pelvic RT for the highest-risk post-cystectomy pts: benefit concentrates in N+ (HR 0.22) and T3+/N+ (HR 0.25), and RT cut isolated locoregional recurrence to zero (LR 8% vs 26%). Technique is standard 50.4 Gy/28 fx stoma-sparing IMRT, transferable; OS gain awaits the MERCY meta-analysis.
12 details 5 trials watching
- 🔍 Phase III RCT, N=153 (RT 77 / obs 76), accrued 2016-2024; largest RCT in this setting, stratified by nodal stage + chemo
- 🔍 High-risk pT3-4/N+/R+ non-metastatic MIBC post-radical cystectomy; 62% pT3-4, 41% pN+, 28% variant histology, median age 57
- 🔍 RT 50.4 Gy/28 fx stoma/bowel-sparing IMRT to cystectomy bed + pelvic nodes (iliac, presacral, obturator), daily IGRT
- 🔍 Chemo neoadjuvant 71%, adjuvant 20%, none 9%; no immunotherapy in either arm
CONSORT flow
- 📊 2-yr outcomes, adjuvant RT vs observation (ITT)
Endpoint (2-yr) RT Obs HR (95% CI) p LRFFS (1°) 87.1% 76.0% 0.43 (0.20-0.96) 0.04 DFS 71.6% 58.7% 0.62 (0.36-1.05) 0.07 BCSS 79.6% 65.0% 0.59 (0.33-1.10) 0.09 OS 70.4% 57.4% 0.78 (0.49-1.26) 0.31 - 📊 Locoregional recurrence 8% (RT) vs 26% (obs), p=0.006; no isolated locoregional recurrences in the RT arm
- 📊 2-yr LRFFS HR by analysis/subgroup (per-protocol 93.2% vs 75.0%)
2-yr LRFFS HR (95% CI) ITT overall 0.43 (0.20-0.96) Per-protocol overall 0.27 (0.10-0.71) T3+ and N+ 0.25 (0.07-0.84) N+ disease 0.22 (0.06-0.75) - 📊 Toxicity, adjuvant RT vs observation
AE RT Obs Late G3+ toxicity 8.4% 10.5% (p=0.60) Acute G3 GI 1.6% 4.1% Acute G2 GI 17.5% 1.4%
- ⚠️ Underpowered ('fell short in sample size goal'); primary LRFFS CI 0.20-0.96 upper bound near 1, p=0.04 marginal
- ⚠️ 14/77 RT-arm pts (refused 8, progressed 4, unfeasible 2) analyzed with observation; per-protocol HR 0.27 vs ITT 0.43
- ⚠️ OS not significant (HR 0.78, p=0.31); benefit is locoregional control, OS awaits MERCY IPD meta-analysis
- ⚠️ No IO tested; adjuvant nivolumab (Bajorin, NEJM 2021) now eligible, untested with/against RT
- OS benefit of adjuvant RT (MERCY IPD meta-analysis pending) n=76 · primary completion 2018-10 · adjuvant EBRT in ≥pT3/margin+/node+ post-cystectomyactive Adjuvant Radiotherapy in Patients With Pathological High-risk Bladder Cancer (GETUG-AFU 30) Phase NAn=81 · primary completion 2027-12 · randomized adjuvant post-cystectomy RT, survival aim
- RT plus immunotherapy with non-overlapping toxicity active Neoadjuvant Sasanlimab With Radiation as an in Situ Vaccine for Cisplatin-ineligible Muscle Invasive Bladder Cancer Phase 2n=33 · primary completion 2025-08 · SBRT + sasanlimab, cisplatin-ineligible MIBCnot yet A Study of Radiation Therapy and Cemiplimab With or Without Fianlimab In People With Bladder Cancer Phase 2n=44 · primary completion 2028-03 · SBRT plus cemiplimab ± fianlimab pre-cystectomy
- Generalizability beyond single high-volume center active Adjuvant Radiotherapy in Patients With Pathological High-risk Bladder Cancer (GETUG-AFU 30) Phase NAn=81 · primary completion 2027-12 · multicentre randomized adjuvant RT trial
📚 Sources · 📄 1 paper
Abstract
2026-06-17
INDIBLADE
ForStage II/III cT2-4aN0-2 MIBC, including node-positive
TL;DR2yr bladder-intact EFS 78% (67-90), OS 96% (91-100) with induction ipi/nivo then chemoRT in cT2-4aN0-2 MIBC.
Node-positive disease (N1-2) was eligible, so 78% 2yr bladder-intact EFS (67-90) extends the preservation pathway past the usual node-negative trimodality candidate. RT dose, fractionation, and radiosensitizer aren't in the source, so transferability to your CRT protocol is unverifiable. Moves the cystectomy-vs-bladder-preservation decision for IO-eligible MIBC.
8 details 5 trials watching
- 🔍 Induction ipilimumab + nivolumab → concurrent chemoradiation (bladder-preservation intent)
- 🔍 Eligibility: stage II/III cT2-4aN0-2 MIBC, includes N1-2 node-positive
- 🔍 RT dose/fractionation + concurrent radiosensitizer not reported in source
- 📊 1° EP: 2yr bladder-intact EFS 78% (95% CI 67-90%)
- 📊 2yr OS 96% (95% CI 91-100%)
- ⚠️ Single-arm: can't isolate induction IO's contribution over chemoRT alone
- ⚠️ Bladder-intact EFS is a composite surrogate; only 2yr f/u
- ⚠️ N not reported in source tweet
- Durability of bladder preservation beyond 2 years active Treating Muscle-invasive Bladder Cancer With A Non-surgical Method Consisting of Anti-PD-1 Therapy and Chemoradiation Phase 2n=71 · primary completion 2025-12 · anti-PD-1 + chemoRT bladder preservation phase 2recruiting Enfortumab Vedotin in Combination With Pembrolizumab vs. Concurrent Chemoradiotherapy (cCRT) in People With Muscle Invasive Bladder Cancer (EV-309) Phase 3n=390 · primary completion 2030-03 · phase 3 bladder-preservation vs chemoRT
- Induction ipi/nivo + CRT vs standard chemoRT or cystectomy n=50 · primary completion 2024-07 · concurrent nivo±ipi with chemoRT, bladder-sparingn=50 · primary completion 2025-09 · induction ipi/nivo then chemoRT, cT2-4aN0-2n=52 · primary completion 2027-01 · neoadjuvant ipi/nivo then cystectomy, chemo-unfit
📚 Sources · 🐦 1 tweet
‼️ INDIBLADE: stage II/III (cT2-4aN0-2) MIBC -> induction ipilimumab plus nivolumab -> CRT
— NonsparseOncologist (@5_utr) June 17, 2026
2-year bladder-intact event-free survival is 78% (0.67−0.9) 🤩
2-year overall survival was 96% (0.91−1)
Lots of bladders can be potentially spared!https://t.co/LzTe72GYHD
2026-05-30 ASCO Annual Meeting 2026
RAD-IO
ForMuscle-invasive bladder cancer, cT2-T3, 13% node+, 75% prior neoadjuvant chemo
TL;DR12-mo DFS 40/50 (80%) cleared the GO threshold for durvalumab added to 5FU/MMC chemoRT in muscle-invasive bladder, bladder-preservation intent.
RT-relevant extension is nodal coverage: node-positive pts (n=7) received 46Gy/20fx elective nodal RT plus 55Gy/20fx to bladder, pushing chemoRT bladder preservation past its usual node-negative limit. Dose is the hypofractionated BC2001 UK schedule (55Gy/20fx), not conventional fractionation, which gates transferability to US practice. Moves whether to add adjuvant IO and extend preservation to node+ MIBC.
- Contextual benchmark BC2001 (JCO 2016), DFS by chemo randomisation: HR 0.78 (0.60-1.02), p=0.07

+1 more figure

8 details 5 trials watching
- 🔍 Single-arm multi-stage feasibility/safety trial, N=55 (54 treated), MIBC, definitive bladder-preservation intent (Abstract 4504, ND James)
- 🔍 RT: 55Gy/20fx to bladder; node-positive pts add 46Gy/20fx elective nodal RT (Stage 1 expansion, first 6 node+ pts)
- 💊 ChemoRT backbone: concurrent 5-FU + mitomycin C (BC2001 regimen)
- 💊 Durvalumab neoadjuvant, synchronous with chemoRT, then adjuvant for 12 months
- 🔍 Population (n=55)
- cT2 44/55 (80%), cT3 11/55 (20%)
- Node+ 7 (13%): N1 4, N2 3
- Prior neoadjuvant chemo 41 (75%)
- Age 69 (IQR 62-76), male 45/55 (82%)
- 📊 1° outcome: 12-mo DFS 40/50 (80%), 95% CI 0.67-0.89, cleared pre-set GO threshold (≥75%) for further evaluation
- ⚠️ Single-arm, benchmarked vs historical BC2001; no contemporaneous chemoRT-alone or durvalumab-omission arm, so the IO contribution can't be isolated
- ⚠️ 12-mo DFS is an early surrogate; bladder-intact survival, OS, and late GU/GI toxicity not reported in source
- Randomised durvalumab vs chemoRT-alone comparison needed n=11 · primary completion 2026-02 · randomizes chemoRT ± durvalumab in MIBC
- Durability of bladder-intact survival and DFS beyond 12 months recruiting Risk-stratification Based Bladder-sparing Modalities for Muscle-invasive Bladder Cancer Phase 2n=30 · primary completion 2024-09 · bladder-sparing MIBC, durable control endpointn=80 · primary completion 2028-08 · tetra-modal MIBC: maintenance IO vs W&Wnot yet Probiotics Combined With Targeted Therapy Plus Immunotherapy in Bladder-Preserving Setting for Patients With MIBC Phase 2n=146 · primary completion 2031-03 · 1° EP: duration of bladder preservation interval
- Bladder-preservation outcomes in node-positive MIBC n=11 · primary completion 2026-02 · chemoRT ± durvalumab in node+ (N1) bladder
📚 Sources · 🐦 3 tweets
RAD-IO at #ASCO26: durvalumab added to chemoradiation in muscle-invasive bladder cancer cleared its efficacy bar in a bladder-preservation approach. Single-arm, benchmarked against prior CRT data.
— Katy Beckermann (@katy_beckermann) May 30, 2026
Durvalumab given before, during, and 12 months after chemoRT (55Gy/20Fr +… pic.twitter.com/UXxwoZzaMC
#ASCO26 🔬 Abstract 4504 | RAD-IO
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
Durvalumab + chemoradiotherapy in muscle-invasive bladder cancer
Presented by Nicholas D. James, PhD, MBBS, FRCP@OncoAlert@ASCO
Bladder preservation in MIBC remains one of the most important curative-intent questions in GU oncology.
The key… pic.twitter.com/W6JqzTVsJ3
RAD-IO: chemoradiation (5FU+MMC) + Durva in MIBC. #ASCO26 pic.twitter.com/yTyhkdjCox
— Álvaro Pinto (@dralvaropinto) May 30, 2026
Perioperative MIBC: Management Post-pCR
TL;DR85% 5-yr OS with pT0 (SWOG 8710) makes pCR strongly prognostic, yet sandwich IO regimens continue planned adjuvant therapy regardless of response.
SWOG 8710ABACUSCHECKMATE-274KEYNOTE-905VOLGANIAGARAVESPERKEYNOTE-B15
- High-risk staging (≥ypT2/N1) after neoadjuvant chemo is an adjuvant indication (CHECKMATE-274)
+1 more figure

8 details 4 trials watching
- 🔍 pCR is registrational only as a phase 3 co-primary; standalone use limited to phase 2 signal-seeking
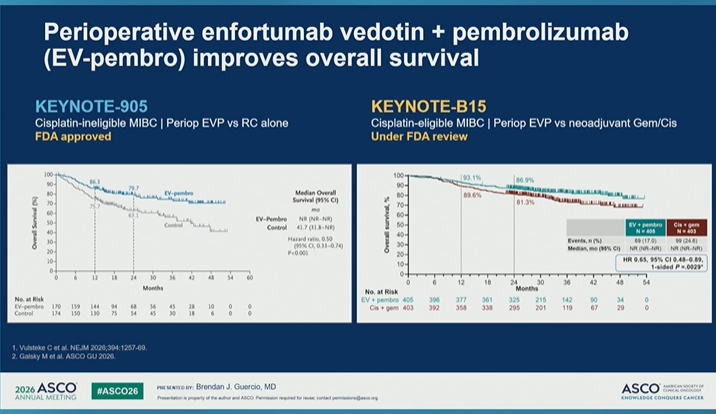
- 🔍 KEYNOTE-905 schedule: 3 cycles EVP, cystectomy, then 6 cycles EV + 14 cycles pembro
- 💊 For sandwich IO regimens, planned adjuvant therapy continues regardless of pathologic response
- 💊 Post-pCR adjuvant continuation by regimen
- NIAGARA: resume durvalumab for 8 months post-cystectomy
- Periop EVP: resume EVP post-cystectomy
- Cisplatin chemo alone: surveillance after pCR is standard
- 📊 pCR (pT0N0) after neoadjuvant chemo is strongly prognostic: SWOG 8710 shows 85% 5-yr OS if pT0
- 📐 Meta-analysis: pooled RR 0.19 for RFS favoring pCR
- 📊 Perioperative regimens by cisplatin-eligibility
Trial Setting Key result KEYNOTE-905 Cis-ineligible, periop EVP vs RC alone OS HR 0.50; now standard (FDA approved) VOLGA Cis-ineligible, preop EV + periop durva/treme Improved EFS (press release) NIAGARA Cis-eligible, preop Gem/Cis + periop durva 24-mo OS 82.2% vs 75.2% VESPER Cis-eligible, ddMVAC vs Gem/Cis 5-yr OS 66% vs 57%; more toxicity KEYNOTE-B15 Cis-eligible, periop EVP vs Gem/Cis Improved OS; under FDA review
- ⚠️ Not all pts in perioperative trials completed adjuvant therapy, sometimes due to toxicity
- Relative contribution of pre- vs postoperative regimen components
- Can adjuvant therapy be de-escalated based on pCR or biomarkers active Treatment Of Metastatic Bladder Cancer at the Time Of Biochemical reLApse Following Radical Cystectomy Phase 2n=154 · primary completion 2024-08 · atezo deferred to molecular relapse post-cyston=761 · primary completion 2025-06 · adjuvant atezo only if ctDNA+ post-cystectomyrecruiting Surveillance of the Genetic Signature in Circulating Tumor DNA for Guiding Adjuvant Chemotherapy in Urothelial Carcinoma Phase 2n=20 · primary completion 2025-09 · ctDNA guides adjuvant gem/cis in urothelialn=992 · primary completion 2030-09 · ctDNA test selects pts for adjuvant nivo/rela
📚 Sources · 🐦 1 tweet
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 Management in Bladder Cancer After Pathologic Complete Disease Response
Presented by Brendan J. Guercio, MD@OncoAlert@ASCO
In muscle-invasive bladder cancer, pCR after neoadjuvant therapy is one of the most powerful prognostic signals we… pic.twitter.com/sMd2In7X3p
GU Curative Intent: Living Longer, Living Better
TL;DRDiscussant roundup balancing cure vs function: durvalumab+chemoRT kept full bladder RT delivery; EV+pembro bladder-sparing (EV309 vs chemoRT) and ctDNA RCC selection maturing.
EV209EV309RAMPART
The radonc read is bladder preservation under competition: durvalumab added to 55Gy/20fx MMC/5-FU chemoRT kept full RT delivery in 54/54 pts (87% without delay), but EV309 now randomizes EV+pembro against chemoradiotherapy itself. If systemic bladder-sparing matures, trimodality's role narrows.
- Adjuvant RCC ctDNA (Choueiri, ASCO 2026): ctDNA status refines selection beyond pathologic features; ctDNA-positive pts had substantially shorter DFS

| RT/chemo delivery | n (%) |
|---|---|
| Full 55 Gy/20 fx RT | 54 (100) |
| No RT extension/delay | 47 (87) |
| 5-FU week 4 administered | 42 (78) |
| Chemo discontinued early | 12 (22) |
| Durvalumab completed | 33 (61) |
| Durvalumab discontinued early | 21 (39) |
+1 more figure

8 details 4 trials watching
- 🔍 ASCO 2026 GU discussant summary (Brian Rini): curative-intent bladder + RCC, framed as improving cure while preserving function/QoL
- 🔍 EV+pembrolizumab bladder-sparing trials in MIBC (EVP)
EV209 EV309 Population Cystectomy-eligible Cystectomy-ineligible/refusing Stage cT2-4a MIBC cT2-4a MIBC N 240 390 Regimen 9 cycles EV + 1 yr pembrolizumab 9 cycles EV + 1 yr pembrolizumab Design single-arm randomized vs chemoradiotherapy Endpoints cCR, 2 yr BIEFS BIEFS, OS
- 📊 Bladder preservation arm: durvalumab added to 55 Gy/20 fx chemoRT (mitomycin C + 5-FU backbone)
- 📊 Per Rini: durvalumab didn't compromise RT delivery, and chemo delivery not significantly compromised
- ⚠️ Deliverability-only readout (N=54); long-term bladder preservation, function, symptom burden, safety and QoL still require follow-up (Rini)
- ⚠️ EV309 randomizes EV+pembrolizumab against chemoradiotherapy, directly pitting systemic bladder-sparing against trimodality
- ⚠️ RAMPART non-clear cell RCC subgroups: few pts/events, wide CIs, point estimates unstable; central pathology review ongoing
- ⚠️ Adjuvant IO has no proven benefit in non-clear cell RCC (per Rini)
- Long-term bladder function and QoL with durvalumab-added chemoRT n=11 · primary completion 2026-02 · durvalumab added to chemoRT in node+ bladder
- Can EV+pembro bladder-sparing match trimodality chemoRT outcomes recruiting A Study to Find Out if Enfortumab Vedotin Given With Pembrolizumab Helps People With Muscle-invasive Bladder Cancer Keep Their Bladder Phase 2n=240 · primary completion 2027-11 · EV+pembro bladder preservation, n=240not yet Neoadjuvant Enfortumab Vedotin Plus Pembrolizumab in Muscle-Invasive Bladder Cancer and Upper Tract Urothelial Carcinoma Phase 2n=39 · primary completion 2029-02 · neoadjuvant EV+pembro, bladder-sparingrecruiting Enfortumab Vedotin in Combination With Pembrolizumab vs. Concurrent Chemoradiotherapy (cCRT) in People With Muscle Invasive Bladder Cancer (EV-309) Phase 3n=390 · primary completion 2030-03 · phase 3 EV+pembro vs concurrent chemoRT
- ctDNA-guided patient selection for adjuvant RCC immunotherapy
📚 Sources · 🐦 1 tweet
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 Living Longer, Living Better: Can We Have It All?
Discussant: Brian I. Rini, MD, FASCO@OncoAlert@ASCO
This GU session captured one of the central tensions in curative-intent oncology:
Can we improve cure rates while preserving quality of… pic.twitter.com/AMwrRZZM2Q
2026-05-21
Bladder Adjuvant Radiotherapy Phase III
ForHigh-risk MIBC post-cystectomy (T3-4, N+, margin+, or ≤10 nodes)
TL;DR2yr LRFS 87.1% vs 76.0%, HR 0.43 (0.20-0.96) p=.04 favoring adjuvant pelvic IMRT in high-risk MIBC post-cystectomy.
Actionable RT detail is technique: stoma-sparing IG-IMRT 50.4Gy/28fx to bed + pelvic nodes delivered the locoregional gain with no added severe toxicity, so it transfers cleanly. The gradient matters: DFS, BCSS, and OS all favored RT yet none reached significance (N=153), moving the offer-adjuvant-RT decision short of a proven survival benefit.
- vs Zaghloul (Egypt NCI RCT): prior adjuvant-RT benefit was in an SCC/bilharzial-enriched cohort; this trial extends the signal to urothelial with modern IMRT
8 details 3 trials watching
- 🔍 Phase III multicenter RCT, N=153 (RT=77, Obs=76); stratified by nodal status + chemo timing
- 🔍 RT: stoma-sparing IG-IMRT 50.4Gy/28fx to cystectomy bed + pelvic nodes
- 🔍 Eligibility: high-risk post-RC (any of T3-4, N1-3, margin+, ≤10 nodes dissected); 62% pT3-4, 41% pN+
- 💊 >90% had perioperative chemo (71% neoadjuvant, 20% adjuvant); none received immunotherapy
- 🔍 RT contribution is clean: both arms had RC + perioperative chemo, so RT vs observation isolates the radiation effect
CONSORT flow
- 📊 Outcomes by arm (RT vs Obs), median f/u 47mo
Endpoint RT Obs HR (95% CI) LRFS (2yr) 87.1% 76.0% 0.43 (0.20-0.96), p=.04 DFS 71.6% 58.7% 0.62 (0.36-1.05) BCSS 79.6% 65.0% 0.59 (0.33-1.10) OS 70.4% 57.4% 0.78 (0.49-1.26) - 📊 No additional severe toxicity with RT; late GU/GI grades not detailed in source
- ⚠️ Underpowered for survival: every secondary (DFS, BCSS, OS) favored RT but all CIs cross 1
- Does locoregional benefit translate to a survival gain in a larger trial active Adjuvant Radiotherapy in Patients With Pathological High-risk Bladder Cancer (GETUG-AFU 30) Phase NAn=81 · primary completion 2027-12 · randomized adjuvant pelvic RT, LRC + survival
- Role of adjuvant RT after adjuvant immunotherapy (none enrolled received IO) recruiting Adjuvant Concurrent Immunotherapy and Radiotherapy for the Treatment of Bladder Cancer Phase 1n=10 · primary completion 2027-04 · adjuvant concurrent IO + RT, urothelial bladder
- Which high-risk subgroup (pN+, margin+, pT3-4) benefits most n=76 · primary completion 2018-10 · adjuvant EBRT, enrolls pT3+/margin+/node+
📚 Sources · 📄 1 paper
Abstract
2026-05-19
Bladder-preserving TMT for MIBC (ESTRO 2026)
ForNon-metastatic MIBC (cT2-T4a N0M0), median age 76
TL;DRCLR 63.7% with trimodality therapy in MIBC; complete local response linked to lower local recurrence and better survival in a 369-pt Spanish cohort.
Image guidance and chemo regimen, not just patient selection, move local control: weekly portal imaging (older 2D IGRT) cut CLR odds (OR 0.35, p<0.001) while 5-FU-based CRT raised them (OR 4.9, p=0.038), VMAT trending favorable. For an RT reader, this argues for conformal daily-IGRT delivery and a 5-FU backbone when offering bladder-preserving TMT.
- No randomised comparator vs radical cystectomy; authors frame survival as comparable to international TMT series
8 details 2 trials watching
- 🔍 Multicenter retrospective cohort, Spain 2010-2022; N=369 cT2-T4a N0M0 MIBC, median age 76, 85.1% male
- 🔍 TMT = maximal TURBT + concurrent chemoRT; 1° EP complete local response (CLR), predictors by multivariable logistic regression
- 🔍 VMAT trended toward favorable outcomes (not statistically significant)
- 📊 CLR 63.7%
- 📊 Disease progression 28.8%, by pattern
- Local 10.1%
- Systemic 10.7%
- Combined 8.7%
- 📊 Salvage cystectomy 9.7%
- 📐 Predictors of CLR (multivariable logistic regression) — comparison values omitted (cell value "0.038" not verified in source)
- ⚠️ Key caveats
- Retrospective: TMT-selected pts likely fitter / lower-burden than RC candidates (selection bias)
- CLR is a surrogate; OS/CSS listed as secondary but no effect size in source
- Randomised TMT vs radical cystectomy in MIBC not yet Radical CystEctomy or RaDio-chEMotherapy as Preferred Treatment for invasivE blaDder Cancer Phase NAn=336 · primary completion 2031-12 · randomised chemoRT vs cystectomy, MFS non-inferiority
- Does daily IGRT improve local control vs weekly portal imaging
- Optimal concurrent chemo regimen for bladder TMT recruiting Adaptive RADiation Therapy With Concurrent Sacituzumab Govitecan (SG) for Muscle Invasive Bladder Cancer Phase 1n=20 · primary completion 2026-06 · concurrent sacituzumab govitecan + adaptive RT
📚 Sources · 🐦 1 tweet
📢 Presentamos en #ESTRO26 nuestro análisis multicéntrico sobre preservación vesical en cáncer vesical músculo-invasivo tratado con TMT.
— URONCOR (@URONCOR) May 19, 2026
🔎 En 369 pacientes, la respuesta completa clínica se asoció a menor recurrencia local y mejor supervivencia!@fcounago #NicoFeltes pic.twitter.com/aQjjkcHGP4