Prostate
Two opposing prostate RT questions answered: ultrahypofx holds (HEAT), elective pelvic nodal escalation doesn't (PEACE 2).
PEACE 2
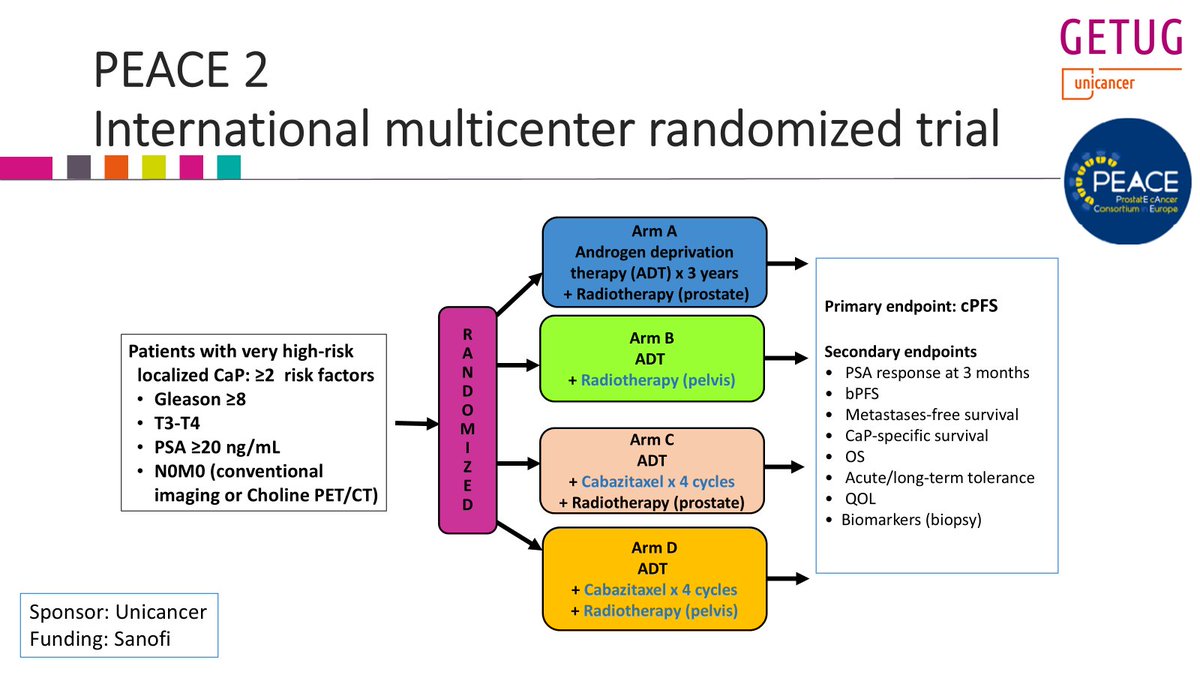
ForVery high-risk localized N0M0 prostate, conventional/choline staging, ≥2 risk fa
TL;DRPelvic RT missed 1° EP cPFS (HR 0.81, p=0.088) in very high-risk N0M0 prostate; no MFS, OS, or PCSS benefit.
The decision is elective pelvic nodal coverage in conventionally-staged very-high-risk N0M0 disease: don't add it. The non-significant cPFS trend (p=0.088) rests on the softest endpoint while MFS, OS, and PCSS are flat. Staging was conventional/choline, not PSMA, so PSMA-selected pts (cf. POP-RT) stay an open question.
- vs POP-RT (JCO 2021): whole-pelvis RT improved biochemical control in high-risk N0; PEACE 2 null. Key difference: POP-RT enriched with PSMA/choline staging and a nodal boost

| Arm | 7yr cPFS | HR (95% CI) | p |
|---|---|---|---|
| Pelvic RT | 67.1% (61.6-72.2) | 0.81 (0.63-1.03) | 0.088 |
| Prostate-only RT | 62.9% (57.4-68.1) | ref | n/a |
+1 more figure
8 details 1 trial watching
- 🔍 Phase III 2×2 factorial (±pelvic RT × ±cabazitaxel); pelvic-RT axis analyzed here, 761 at risk (380 prostate-only vs 381 pelvic)
- 🔍 Pts: very high-risk localized N0M0, ≥2 of Gleason ≥8, T3-T4, PSA ≥20; staged by conventional imaging or choline PET/CT
- 💊 All arms: ADT ×3yr + high-dose prostate RT; the pelvic axis adds elective whole-pelvis nodal volume
- 🔍 Author reports minimal added toxicity from pelvic nodal RT with modern technique (no effect size reported in source)
CONSORT flow
- 📊 1° EP cPFS not met: pelvic RT gave only a non-significant trend (p=0.088)
- ⚠️ No pelvic-RT effect on the hard endpoints MFS, OS, or PCSS (effect sizes not reported in source)
- ⚠️ Even the favorable direction sits on cPFS, the softest endpoint; the clinically meaningful endpoints are flat
- ⚠️ Conventional/choline staging may miss occult PSMA-avid nodal disease, diluting any pelvic-RT signal
- Does whole-pelvis RT benefit PSMA-PET-staged node-negative pts? n=250 · primary completion 2031-05 · WPRT vs prostate-only RT in PSMA-N0M0 high-risk
- Did cabazitaxel add benefit in the factorial's systemic axis?
📚 Sources · 🐦 1 tweet
Yesterday, I presented the @GETUG_Unicancer PEACE 2 trial at #ESTRO26 on the role of pelvic RT in very high risk #prostatecancer pts (staged with conventional imaging).
— Pierre Blanchard, MD (@PBlanchardMD) May 18, 2026
Twittorial below
Key conclusion: pelvic RT did not improve clinical outcomes (cPFS, MFS, PCSS, OS)...
1/n pic.twitter.com/ZKRt2QZzt1
HEAT Trial NCT01794403
ForLocalized low- to intermediate-risk prostate, IPSS <12
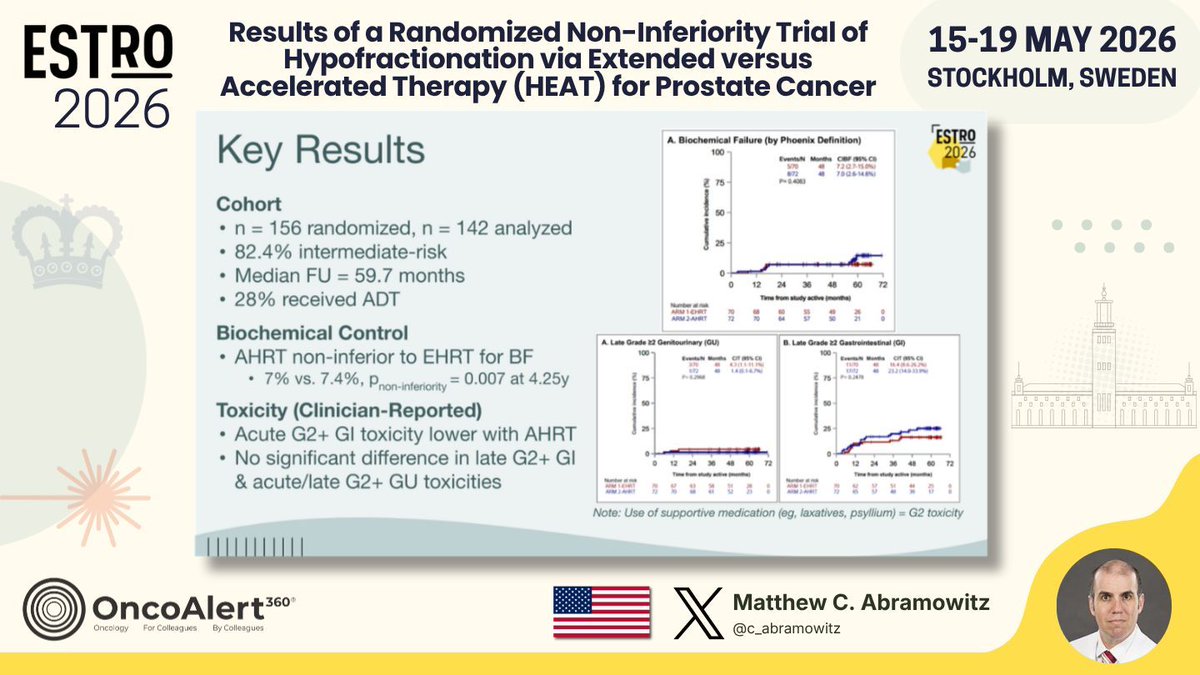
TL;DRAHRT (5 fx SBRT) non-inferior to EHRT (26 fx IMRT) for biochemical failure: 7% vs 7.4%, P=0.007 at 4.25y in localized low-int-risk PCa.
The RT read is toxicity, not just equivalence: acute G2+ GI was lower with 5 fx AHRT despite a GTV SIB to 40 Gy, with no late GI or GU penalty vs 26 fx EHRT. For low- to int-risk PCa weighing 5 vs 26 fractions, this backs SBRT on access without a control or toxicity cost. ADT was permitted (28%), unlike PACE-B and HYPO-RT-PC.
- Unlike HYPO-RT-PC, PACE-B, NRG-GU005 (all barred ADT), HEAT permitted ≤6 mo ADT
| Endpoint | AHRT | EHRT | P (NI) |
|---|---|---|---|
| Biochemical failure, 4.25y | 7% | 7.4% | 0.007 |
+1 more figure
8 details 5 trials watching
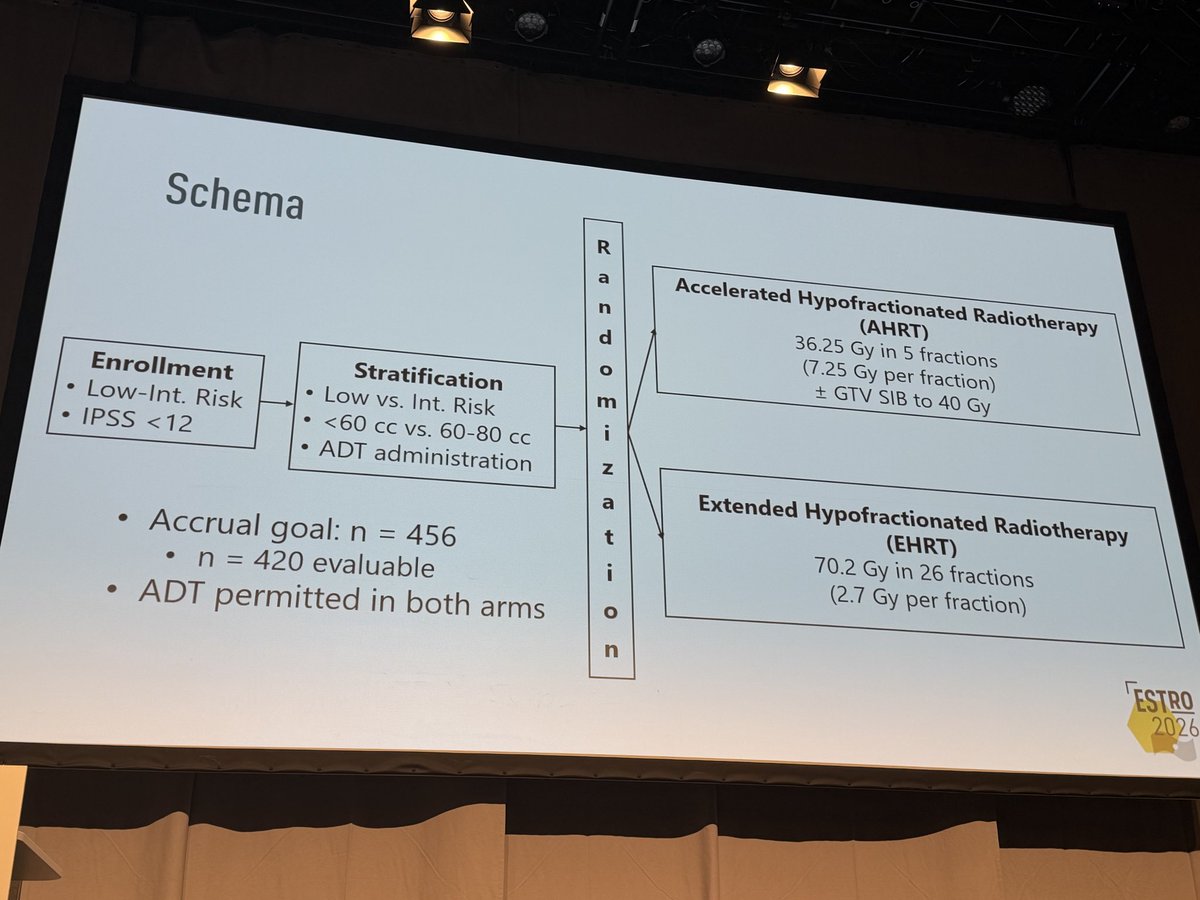
- 🔍 First randomized phase III comparing AHRT (5 fx) vs EHRT (26 fx) head-to-head 1:1, modern IMRT + ADT permitted
- 🔍 Eligibility: localized low- to intermediate-risk PCa, IPSS <12
- 🔍 Cohort characteristics
- 82.4% intermediate-risk
- Median follow-up 59.7 mo
- 28% received ADT (≤6 mo permitted both arms)
- 📊 Acute G2+ GI toxicity lower with AHRT vs EHRT
- 📊 No significant difference in late G2+ GI or acute/late G2+ GU
- ⚠️ Interim analysis: 142 analyzed vs accrual goal 456 (420 evaluable), well short of full accrual
- ⚠️ Supportive meds (laxatives, psyllium) counted as G2 toxicity, inflating reported GI rates
- ⚠️ Wide 12% non-inferiority margin (Phoenix BF) could mask a clinically meaningful difference
- Durability of non-inferiority at full accrual (n=456) and longer follow-up recruiting Two-fraction Versus Five-fraction Stereotactic Radiotherapy for Localized Prostate Cancer Phase NAn=562 · primary completion 2027-12 · RCT 2-fx vs 5-fx SBRT, low/fav int-risk localized
- Generalizability to high-risk or larger-volume (>80cc) prostate recruiting Standard Moderately Hypofractionated RT vs. Ultra-hypofractionated Focal Lesion Ablative Microboost in Prostate Cancer Phase NAn=484 · primary completion 2032-01 · RCT ultra-hypofx vs moderate, int/high-riskn=49 · primary completion 2032-05 · SBRT+ADT cohort, organ-confined high-risk PCarecruiting Androgen Suppression Combined With Nodal Irradiation and Dose Escalated Prostate Treatment Phase 3n=710 · primary completion 2032-10 · phase 3 SBRT vs brachy boost, unfavourable riskrecruiting Phase III Adaptive Adaptive Stereostactic Body Radiotherapy (SBRT) With Dose Escalation for High-Risk Prostate Cancer Phase NAn=390 · primary completion 2033-04 · phase 3 SBRT dose escalation, high-risk PCa
📚 Sources · 🐦 2 tweets
Day FOUR of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 18, 2026
Results of a Randomized Non-Inferiority Trial of Hypofractionation via Extended versus Accelerated Therapy (HEAT) for Prostate Cancer Presented by Matthew C. Abramowitz🇺🇸 #RadOnc ☢️ #ProstateCancer
HEAT is an international phase… pic.twitter.com/IkSTgQHwXK
The HEAT trial is another randomized demonstration of the safety & efficacy of SBRT compared to hypofractionted RT in #prostatecancer at #ESTRO26 pic.twitter.com/c9sNb3KOqo
— Pierre Blanchard, MD (@PBlanchardMD) May 18, 2026

