Retrospective
ctDNA and Local Regrowth/Distant Mets in Nonoperative Management of Stage II-III Rectal Cancer
ForMSS stage II-III rectal adenoca in cCR/nCR on watch-and-wait after TNT
TL;DRctDNA sensitivity 41% for local regrowth vs 74% for distant mets; positive result predicts both but can't replace endoscopy/MRI surveillance in rectal NOM.
The asymmetry is the actionable read: ctDNA caught only 41% of local regrowths vs 74% of distant mets, so for post-TNT organ-preservation surveillance it flags distant-met risk but can't replace endoscopy/MRI. ctDNA+ at regrowth also tracked more advanced ypT3-4 salvage pathology (75% vs 21%).

7 details 1 trial watching
Prospective single-center cohort (MD Anderson INTERCEPT program), N=110, 2020-2024. Serial tumor-informed ctDNA (Signatera Exome), 669 samples; median follow-up 25 mo (IQR 18-37).
MSS stage II-III rectal adenocarcinoma in cCR (69) or nCR (41) after NAT, managed non-operatively. Median age 56; cT3 in 72 and cN1-2 in 60 of 110; NAT almost entirely TNT (104/110).
Regrowth-free and distant-metastasis-free survival by longitudinal and first-post-NAT ctDNA; per-sample diagnostic accuracy (±90d of each draw); salvage-surgery pathology by ctDNA status. No registered primary endpoint (observational).
Local regrowth in 23 (21%), distant mets in 12 (11%). Ever-positive ctDNA tracked worse regrowth-free and distant-met-free survival (log-rank p=0.0002 and p<0.0001). Per-sample sensitivity 41% local regrowth vs 74% distant mets.
| Endpoint | Sensitivity | Specificity | Accuracy |
|---|---|---|---|
| Local regrowth | 41% (12/29) | 94% (480/509) | 91% (492/538) |
| Distant metastasis | 74% (31/42) | 97% (611/627) | 96% (642/669) |
Consistent with the emerging ctDNA-as-prognostic signal in rectal NOM, but quantifies a sensitivity ceiling (41%) that limits its use for local-regrowth surveillance.
Single-center, N=110 with only 29 regrowth- and 42 distant-met-associated samples driving diagnostic estimates. Assay-specific (Signatera tumor-informed); no comparison vs imaging-alone surveillance.
Single-center prospective cohort (N=110), no interventional comparator; prognostic association consistent with emerging ctDNA-in-NOM data and reaffirms imaging/endoscopy surveillance can't be replaced.
Applies to the MSS stage II-III rectal pt in cCR/nCR pursuing watch-and-wait after TNT, in whom a negative ctDNA still can't exclude local regrowth; it does not extend to MSI-H tumors or pts not pursuing organ preservation.
- Does ctDNA-guided surveillance improve organ-preservation outcomes vs imaging alone n=100 · primary completion 2025-12 · candidate match
- Can serial ctDNA kinetics raise local regrowth sensitivity above 41%
- Generalizability beyond single-center tumor-informed Signatera cohort
📚 Sources · 🐦 1 tweet
Important study re: ctDNA for non-op surveillance in rectal ca.
— Dr. Nina Niu Sanford (@NiuSanford) June 1, 2026
Pos ctDNA associated w regrowth (60%) & distant mets (60%), but neg ctDNA doesn't exclude local regrowth (sensitivity only 41%)
ctDNA good for risk stratification but not surveillance replacement #ASCO26 @OncoAlert pic.twitter.com/UQQub5QfNB
Genomic Classifier + NCCN Risk Stratification (Abstract 5000)
ForNCCN high-risk/very-high-risk localized prostate cancer
TL;DR22-gene GC independently prognostic (MFS/DM/OS, p<0.001); combined NCCN+GC score reclassifies ~¼ of high-risk pts to gate AAP intensification on an RT+ADT backbone.
~¼ of NCCN ≥HR pts are clinical/GC-discordant, so the 22-gene GC reclassifies who reaches CT-VHR (≥3 pts) and has AAP added onto the fixed RT+ADT backbone. The intensification it triggers carries STAMPEDE M0 magnitude (MFS HR 0.53, OS HR 0.60). It sharpens the intensification decision, not RT dose or target.

+2 more figures

| Endpoint | HR (add AAP) | 95% CI | p |
|---|---|---|---|
| MFS | 0.53 | 0.44-0.64 | <0.0001 |
| OS | 0.60 | 0.48-0.73 | <0.0001 |

7 details
Retrospective validation of the 22-gene GC (Decipher) layered on NCCN clinical risk in NCCN ≥ high-risk localized prostate (NRG cohort), externally benchmarked to STAMPEDE M0 curves (Attard, Lancet 2022). Not a prospective RCT.
NCCN high-risk and very-high-risk localized prostate cancer, all planned for definitive RT+ADT.
CT-HR (≤2 pts) → RT+ADT; CT-VHR (≥3 pts) → RT+ADT+AAP (abiraterone acetate + prednisone) intensification.
GC is independently prognostic for MFS, DM, and OS over clinical variables (multivariable, p<0.001). Roughly one-quarter of NCCN ≥HR pts are clinical/GC-discordant, reclassifying risk band and the intensification call.
| Component | Category | Points |
|---|---|---|
| NCCN clinical | High-risk | +1 |
| NCCN clinical | Very-high-risk | +2 |
| GC (Decipher) | < 0.6 | 0 |
| GC (Decipher) | 0.6-0.85 | +1 |
| GC (Decipher) | > 0.85 | +2 |
AAP intensification magnitude is borrowed from STAMPEDE M0 (Attard, Lancet 2022), not generated here; GC prognostic value aligns with prior Decipher/NRG validation.
Prognostic, not predictive: no randomized biomarker×treatment interaction showing CT-VHR pts gain more from AAP. Intensification benefit imported from an external trial's average effect.
Retrospective GC prognostic validation, not a randomized predictive-biomarker trial; consistent with prior Decipher/NRG data. Intensification benefit borrowed from STAMPEDE, not shown to be GC-predictive.
In NCCN high-risk/very-high-risk localized prostate planned for definitive RT+ADT, this supports GC-informed CT-VHR (≥3 pts) selection for AAP intensification; it does not extend to intermediate-/low-risk disease or change RT dose or target.
- Does GC-guided AAP intensification improve outcomes prospectively?
- Is GC predictive of differential AAP benefit, not just prognostic?
- Optimal AAP intensification threshold in clinical/GC-discordant pts
📚 Sources · 🐦 2 tweets
#ASCO26 Dr. Patel presented a clinically practical framework integrating NCCN clinical risk + a 22-gene genomic classifier to guide treatment intensification in high-risk localized prostate cancer.
— Julian Chavarriaga (@chavarriagaj) May 30, 2026
Key findings:
🔹 The genomic classifier independently improved prognostic… pic.twitter.com/fRcdTmfBec
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 Abstract 5000 | High-risk prostate cancer
Clinico-transcriptomic risk stratification to guide abiraterone intensification
Presented by Krishnan R. Patel, MD, MHS@Krishnan_Patel@OncoAlert@ASCO
In high-risk localized prostate cancer,… pic.twitter.com/pZSCiTyGB8
SWOG S1007
ForHR+/HER2− breast, 1-3 nodes, Oncotype RS ≤25
TL;DR5y LRR 0.55% without RNI vs 0.85% with; IDFS unchanged by RNI (HR 1.03 premenopausal, 0.85 postmenopausal) in RS ≤25 N1 breast.
The RT read: RNI omission after breast conservation carries low locoregional risk, 5y LRR 0.55% without RNI vs 0.85% with, in RS ≤25 N1 disease. Chemo omission alone is not an RNI indication, so this supports withholding RNI in biologically favorable N1, pending randomized confirmation.
6 details 3 trials watching
Secondary analysis of SWOG S1007 (RxPONDER), a phase 3 RCT of chemo omission by 21-gene recurrence score. RNI receipt was prospectively recorded, not randomized. Median follow-up 6.1y; survival landmarked at 1y.
HR+/HER2−, Oncotype RS ≤25, 1-3 positive nodes. 4871 had RT forms; 81% received RT, and 59% of those with target data received RNI (targeting ≥ supraclavicular region).
RNI defined as targeting at least the supraclavicular region. The 59/41 split in RNI use reflects genuine practice equipoise in favorable N1 disease.
LRR was low across every locoregional approach; only mastectomy without RT reached 1.7%. IDFS did not differ by RNI in either menopausal group (see tables).
| Locoregional therapy | 5y cumulative LRR |
|---|---|
| BCS + RT + RNI | 0.85% |
| BCS + RT, no RNI | 0.55% |
| Mastectomy + PMRT | 0.11% |
| Mastectomy, no RT | 1.7% |
| Menopausal status | IDFS HR | 95% CI | p |
|---|---|---|---|
| Premenopausal | 1.03 | 0.74-1.43 | 0.87 |
| Postmenopausal | 0.85 | 0.68-1.07 | 0.16 |
Consistent with MA.20 / EORTC 22922, where RNI's benefit was concentrated in higher-risk node-positive disease. TAILOR RT (MA.39) is randomizing RNI in exactly this RS-low N1 population.
RNI comparison is non-randomized: confounding by indication (higher-risk pts selected for RNI) can mask a true RNI effect. Landmarking at 1y and diverse-setting RT reporting add noise.
RNI vs no-RNI comparison is non-randomized within RxPONDER; confounding by indication limits the null IDFS and low-LRR read. Randomized RNI trial (TAILOR RT) pending.
In HR+/HER2− breast with 1-3 positive nodes and Oncotype RS ≤25, this supports omitting regional nodal irradiation given low LRR; it does not extend to higher recurrence-score or >3 node disease.
- Randomized confirmation of RNI omission in favorable-risk N1 disease recruiting Evaluating Omitting of Internal Mammary Irradiation Among Early Stage Intermediate Risk (N1) Breast Cancer Phase NAn=214 · primary completion 2025-10 · genomic model omits IMN irradiation in N1recruiting The T-REX Trial: Tailored Regional External Beam Radiotherapy in Clinically Node-negative Breast Cancer Patients With 1-2 Sentinel Node Macrometastases. Phase NAn=1350 · primary completion 2028-12 · RCT omitting regional RT, 1-2 macromets, ER+/HER2-recruiting RecurIndex Guided Avoidance of Regional Nodal Irradiation for Node Positive Breast Cancer Phase NAn=540 · primary completion 2029-08 · RecurIndex-guided RNI avoidance in N1 low-risk
- Durability of low LRR beyond 6 years without RNI
📚 Sources · 📄 1 paper
Abstract
Proton vs Photon PMRT Capsular Contracture
ForPostmastectomy implant-based reconstruction (TE/I or DTI) receiving PMRT
TL;DRProton PMRT trended toward higher capsular contracture vs IMRT photon (univariate HR 2.3; MVA HR 1.76 ns); proton+DTI worst, 50% 2yr CC.
The interaction is the read: DTI reconstruction, not modality, dominates CC risk (HR 3.0), and proton+DTI stacks to 50% 2yr CC vs 12% for photon+TE/I. When proton is chosen for cardiac/pulmonary sparing, reconstruction choice (favor TE/I over DTI) is the modifiable lever.
8 details 2 trials watching
Retrospective, IRB-approved, 2 centers within one institution, Jan 2017 to Dec 2023. N=175 (89 proton, 86 photon). CC estimated by Kaplan-Meier; Cox proportional hazards for HRs, logistic regression to verify. Median follow-up 42 mo (proton), 47 mo (photon).
Breast cancer pts with subpectoral 2-stage tissue expander/implant (TE/I) or direct-to-implant (DTI) reconstruction receiving PMRT. Median age 49 (24-78); 63% Hispanic. All TE/I pts had the expander irradiated. Groups imbalanced on laterality (P<.001) and reconstruction type (P<.001).
PBS proton vs IMRT photon PMRT. Dose and fractionation not reported in source. In TE/I, the tissue expander itself was the irradiated target.
Proton vs photon CC: univariate HR 2.3 (1.26-4.30, P=.007), attenuating to HR 1.76 (0.93-3.32, P=.083, ns) on multivariable. DTI vs TE/I: HR 3.0 (1.7-5.5, P<.001), the dominant driver. Per-group 2yr CC rates in the table.
| Modality + reconstruction | n | 2-yr CC rate |
|---|---|---|
| Proton + DTI | 36 | 50% |
| Photon + DTI | 15 | 35% |
| Proton + TE/I | 53 | 23% |
| Photon + TE/I | 71 | 12% |
Prior proton PMRT evidence centered on improved cardiac and pulmonary dosimetry; head-to-head capsular-contracture data proton vs photon were scarce. This is the largest proton reconstruction cohort reported to date.
Retrospective, single-institution, N=175, with groups imbalanced on reconstruction type and laterality. The proton effect lost significance after adjustment (P=.083), so residual confounding (reconstruction type driving both proton selection and CC) cannot be excluded.
The modifiable variable is reconstruction, not beam: DTI carries roughly 3x the CC hazard, and proton stacked on DTI reaches 50% 2yr CC. Where proton is chosen for heart or lung sparing, staged TE/I may blunt the CC penalty; a prospective comparison is needed to confirm.
Retrospective single-institution cohort; groups imbalanced on reconstruction type and laterality; proton effect lost significance on multivariable (HR 1.76, P=.083). Signal, not confirmation.
In a postmastectomy pt weighing DTI vs staged TE/I reconstruction who will receive proton PMRT, the CC signal is concentrated in DTI (proton+DTI 50% vs proton+TE/I 23% 2yr); it does not resolve proton vs photon overall, which was ns on multivariable.
- Prospective proton vs photon PMRT capsular contracture comparison
- Whether staged TE/I reconstruction mitigates proton capsular contracture risk n=300 · primary completion 2023-08 · 2-stage expander/implant, capsular contracture EPrecruiting Breast Reconstruction and Radiotherapyn=750 · primary completion 2027-08 · recon timing + type vs RT complication risk
- Mechanism: proton dose distribution vs selection bias driving contracture
📚 Sources · 📄 2 papers
Abstract
Multicenter TMT Bladder Preservation Analysis (n=369)
ForMuscle-invasive bladder, cT2-T4aN0M0, median age 76
TL;DRCLR 63.7% in 369 MIBC pts on definitive TMT; 5-FU-based CRT and better image guidance predicted higher complete local response.
The two modifiable levers here are RT delivery and chemo backbone, both in the radonc's hands: 5-FU-based CRT predicted higher CLR (OR 4.9) and weekly portal imaging lower CLR (OR 0.35, p<0.001), favoring daily volumetric IGRT. Technique, not just patient selection, moved local control.
8 details 4 trials watching
Multicenter retrospective cohort, Spain 2010-2022, N=369 treated with definitive TMT (maximal TURBT + concurrent chemoRT). Multivariable logistic regression for predictors of complete local response.
cT2-T4aN0M0 muscle-invasive bladder. Median age 76, 85.1% male. Node-positive and metastatic disease excluded by staging.
Image-guidance quality tracked with local control: weekly portal imaging predicted lower CLR (OR 0.35, p<0.001), favoring daily volumetric IGRT; VMAT showed a non-significant favorable trend. RT dose/fractionation not reported in source.
Concurrent chemoradiotherapy. 5-FU-based CRT predicted higher CLR (OR 4.9, 95% CI 1.1-22.1, p=0.038).
Primary: complete local response (CLR). Secondary: OS, CSS, recurrence patterns, salvage cystectomy.
CLR 63.7%. Disease progression 28.8% (local 10.1%, systemic 10.7%, combined 8.7%). Salvage cystectomy 9.7%.
Retrospective, non-randomised; CLR predictors exploratory and confounded by treatment era. No head-to-head vs radical cystectomy; RT technique detail and CLR-survival effect sizes absent from source.
Retrospective real-world European cohort; no randomised TMT-vs-cystectomy comparator. Reinforces guideline-recognized bladder preservation; predictor findings exploratory.
In cT2-T4aN0M0 MIBC pts already committed to bladder-preserving TMT, this favors daily volumetric IGRT and 5-FU-based chemoRT for local control; it does not inform the upstream TMT-versus-radical-cystectomy choice or node-positive/metastatic disease.
- Optimal concurrent chemoradiotherapy regimen for bladder preservation active Treating Muscle-invasive Bladder Cancer With A Non-surgical Method Consisting of Anti-PD-1 Therapy and Chemoradiation Phase 2n=71 · primary completion 2025-12 · adds toripalimab to concurrent chemoRTrecruiting Enfortumab Vedotin in Combination With Pembrolizumab vs. Concurrent Chemoradiotherapy (cCRT) in People With Muscle Invasive Bladder Cancer (EV-309) Phase 3n=390 · primary completion 2030-03 · phase 3 EV+pembro vs concurrent chemoRT
- Whether daily volumetric IGRT improves local control vs weekly imaging n=345 · primary completion 2021-12 · adaptive tumour-focused vs whole-bladder RTnot yet Evaluation of the Clinical Utility of Online Adaptive Radiotherapy in Bladder Cancer (BLADAPT-GETUG V11) Phase NAn=120 · primary completion 2029-01 · randomised online-adaptive vs standard RT in TMT
- Randomised TMT vs radical cystectomy comparison
📚 Sources · 🐦 1 tweet
📢 Presentamos en #ESTRO26 nuestro análisis multicéntrico sobre preservación vesical en cáncer vesical músculo-invasivo tratado con TMT.
— URONCOR (@URONCOR) May 19, 2026
🔎 En 369 pacientes, la respuesta completa clínica se asoció a menor recurrencia local y mejor supervivencia!@fcounago #NicoFeltes pic.twitter.com/aQjjkcHGP4
Single-fraction SABR for primary NSCLC and lung oligomets (pooled, n=1687)
ForPrimary NSCLC or pulmonary oligometastases, SABR candidates
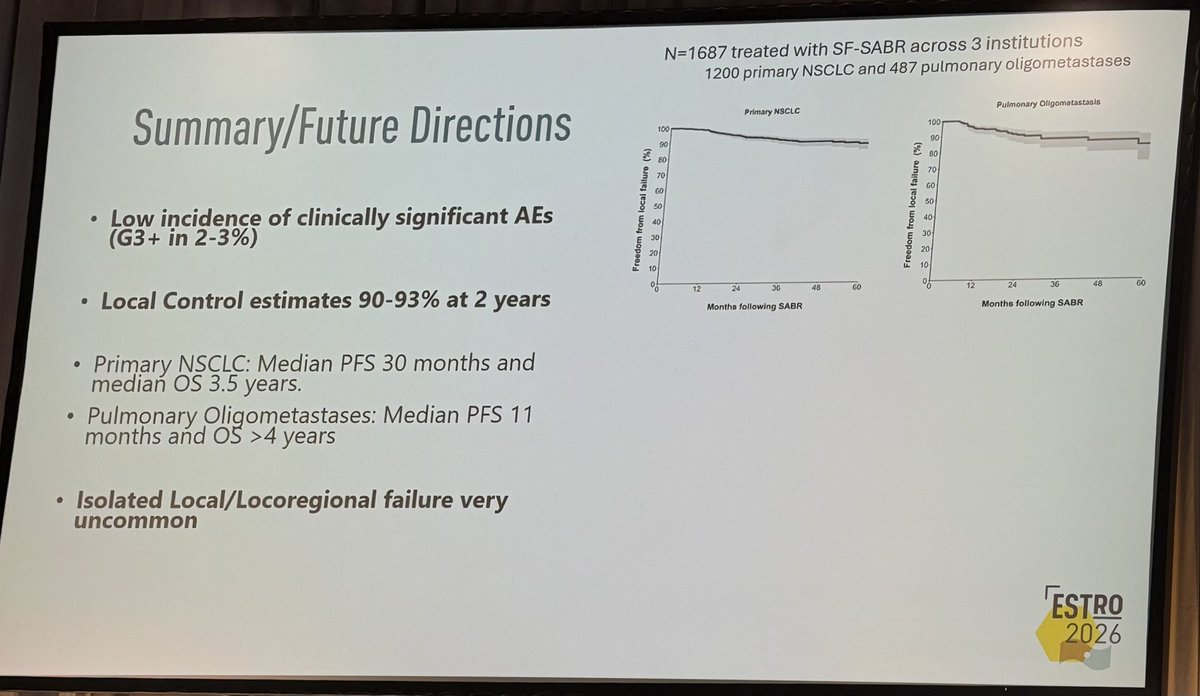
TL;DR2-yr local control 90-93% and G3+ AEs 2-3% across 1687 pts (1200 primary NSCLC, 487 oligomets) treated with single-fraction SABR.
The transfer gate is the fraction size the source omits: outcomes are labeled single-fraction but no Gy dose is given, so you cannot map this 2y LC of 90-93% onto a specific regimen before offering one visit instead of a multi-fraction course. Toxicity (G3+ 2-3%) comes from 2 of 3 sites only. Moves the single- vs multi-fraction choice for lung SABR.
+2 more figures
| Endpoint | Primary NSCLC | Oligomets |
|---|---|---|
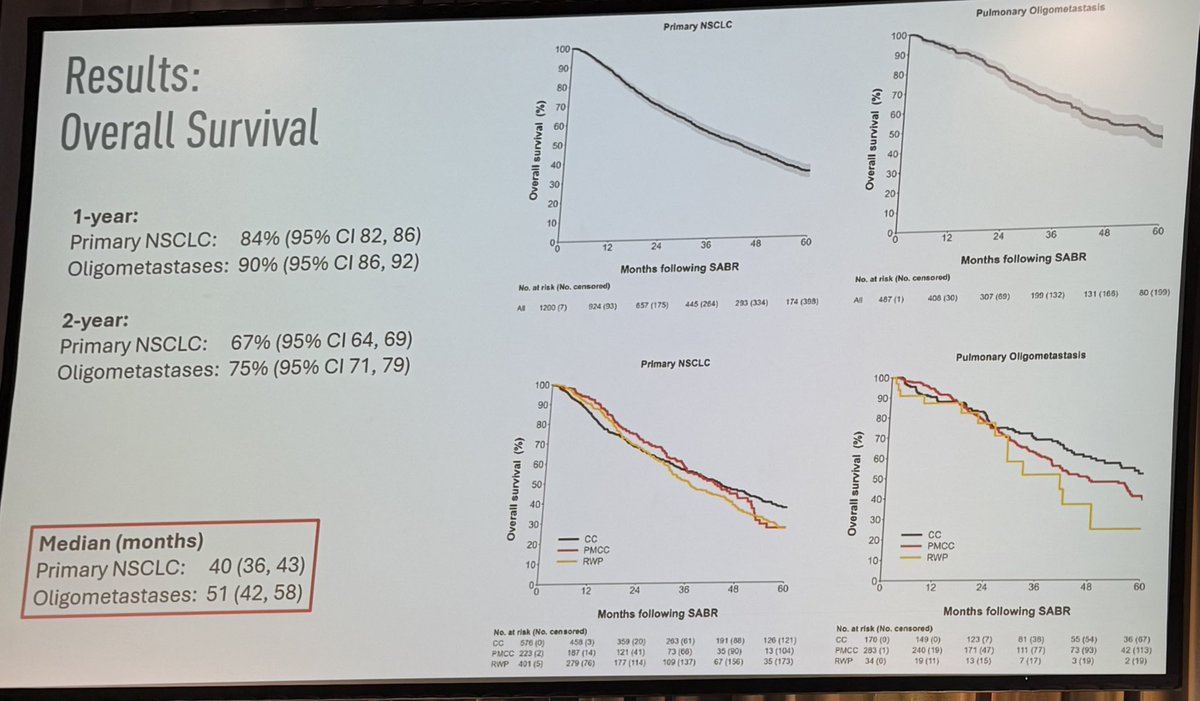
| 1-yr OS | 84% (82-86) | 90% (86-92) |
| 2-yr OS | 67% (64-69) | 75% (71-79) |
| Median OS | 40 mo (36-43) | 51 mo (42-58) |
7 details 1 trial watching
Pooled retrospective analysis of 3 institutions (Peter MacCallum, Cleveland Clinic, Roswell Park). N=1687 (1200 primary NSCLC, 487 pulmonary oligometastases). No randomisation, no comparator arm; survival curves out to 60 months.
Primary NSCLC (n=1200) and pulmonary oligometastases (n=487) treated with single-fraction SABR. Stage, tumour location, and specific eligibility criteria not reported in source.
Single-fraction SABR across all pts. The Gy dose is not reported in source (single fraction only), so the specific regimen behind these outcomes is unknown, gating whether the result transfers to a given practice.
No prespecified primary endpoint stated. Reported: local control, overall survival, PFS, and adverse events.
2y local control 90-93%; isolated local/locoregional failure very uncommon. Median PFS 30 mo (NSCLC) vs 11 mo (oligomets). OS by cohort shown in the figure.
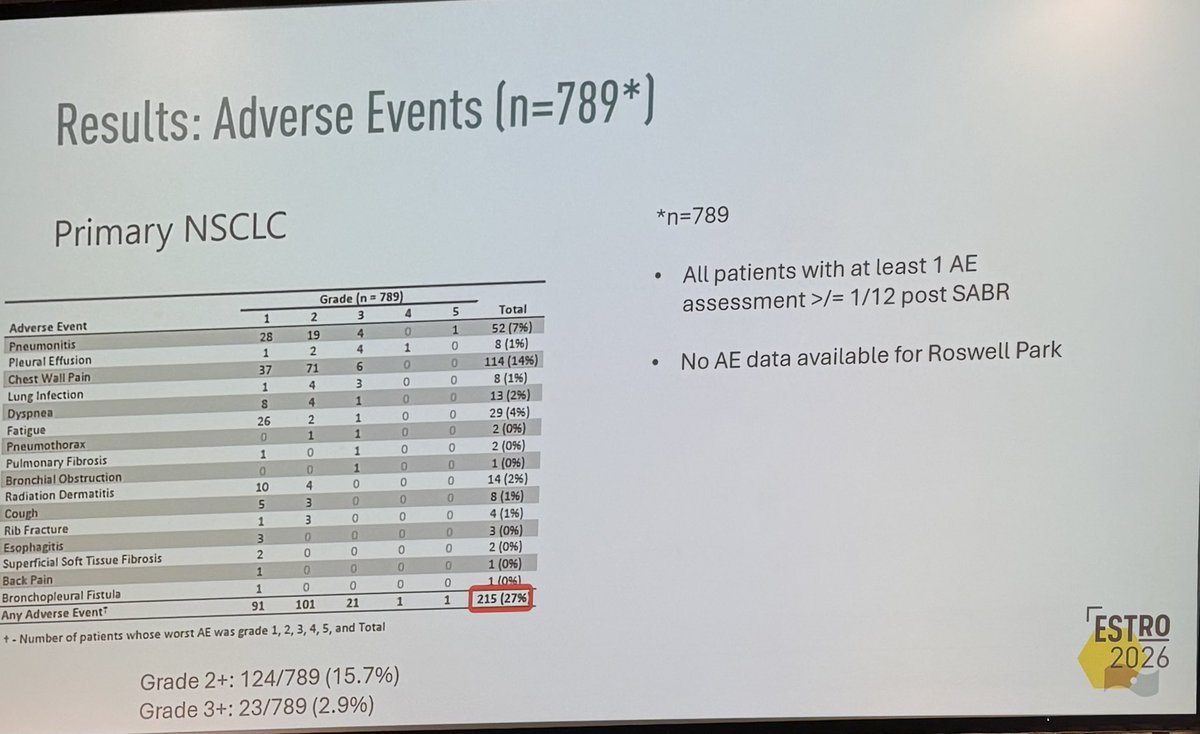
G3+ AEs 2-3% (23/789, 2.9% in the assessed NSCLC subset); G2+ 124/789 (15.7%), any AE 215/789 (27%). AE data from 2 of 3 sites only (no Roswell Park).
Consistent with SAFRON II (TROG 13.01) and RTOG 0915 supporting single-fraction lung SABR, but those were randomised; this pooled cohort carries no comparator.
Retrospective, no randomised/matched comparator. Single-fraction Gy dose unstated. AE denominator excludes one of three sites (n=789 of 1687).
Pooled retrospective single-arm cohort, no randomised or matched comparator vs multi-fraction SABR; single-fraction Gy dose unstated. Consistent with SAFRON II / RTOG 0915.
In pts with primary NSCLC or a pulmonary oligometastasis being considered for SABR, this supports single-fraction delivery as a lower-visit option with high local control; it does not establish it over a multi-fraction schedule, which this cohort did not compare against.
- Single-fraction vs multi-fraction SABR in a randomised comparison active A Pilot Study of Single Fraction Stereotactic Body Radiation Therapy (SBRT) in Central Non-Small Cell Lung Cancer Phase NAn=30 · primary completion 2028-03 · single-fx vs multi-fx SBRT in central NSCLC
- Optimal single-fraction dose across primary NSCLC and pulmonary oligometastases
📚 Sources · 🐦 1 tweet
👏🏽👏🏽👏🏽@neildwallaceie at #ESTRO26 - 1687 patients receiving single fraction SABR for #lungcancer and pulmonary oligomets, @PeterMacRadOnc / @ClevelandClinic / @RoswellPark. Fantastic local control, and low adverse rates. Should we be using “one stop” SABR more often #radonc ? pic.twitter.com/w2IlGKRU5o
— Shankar Siva (@_ShankarSiva) May 18, 2026