Confirmatory
NRG Oncology/RTOG 0848
ForResected pancreatic head adenocarcinoma, progression-free after adjuvant chemo
HR 0.96
90% CI 0.79-1.18, 1-sided P=.38; primary EP not met
TL;DROS primary EP not met (HR 0.96, 90% CI 0.79-1.18) adding adjuvant CXRT to gemcitabine; node-negative subgroup OS benefit on interaction (P=.0063).
The RT read is the node-negative interaction: CXRT improved OS (P=.0063) and DFS (P=.014) in node-negative pts, though the subgroup HR/median isn't in the source text. Unlike ESPAC-1's older 5-FU CXRT, modern CXRT showed no OS harm. Moves selective adjuvant CXRT for node-negative resected head tumors, pending FOLFIRINOX-era confirmation.
This reopens selective adjuvant CXRT in node-negative resected head tumors (OS interaction P=.0063), where modern technique avoided the OS harm ESPAC-1 saw. Cost is doubled grade 3 toxicity (38% vs 19%); dose and target volume aren't in the source, and node-positive pts got no benefit.
Adjuvant gemcitabine-based chemo alone stays the reference: adding CXRT didn't improve OS (HR 0.96) or DFS (HR 0.82, P=.089) overall and raised grade 3 toxicity to 38% vs 19%. The node-negative interaction (P=.0063) would need retesting against FOLFIRINOX before altering adjuvant sequencing.
8 details 3 trials watching
Multicenter phase IIR/III, two-step RCT. Step 1: gemcitabine vs gemcitabine + erlotinib. Step 2 (reported here): random assignment to a sixth chemo cycle ± CXRT after 5 progression-free cycles. N=354 (180 CXRT, 174 chemo).
Curative-intent resected pancreatic head adenocarcinoma, progression-free on adjuvant chemo. Median age 63, 55% male, 56% PS 1.
Fluoropyrimidine-sensitized CXRT added to the sixth cycle. Dose, fractionation, and target volume not stated in the source excerpt.
Primary: overall survival. Secondary: DFS. Powered for HR 0.76 (316 events, 80% power, 1-sided α=.05).
Primary OS not met (HR 0.96). The one positive signal was the treatment-by-nodal-status interaction (OS P=.0063, DFS P=.014) favoring CXRT in node-negative pts; subgroup effect size not in source.
| Endpoint | Chemo + CXRT | Chemo alone |
|---|---|---|
| Median OS | 2.3 yr (2.0-2.6) | 2.6 yr (2.1-3.1) |
| 5-yr OS | 27.9% (22.2-33.6) | 23.1% (17.7-28.6) |
| OS HR (90% CI) | 0.96 (0.79-1.18), P=.38 | ref |
No increase in grade 4/5 toxicity. Grade 3 toxicity higher with CXRT: 38% vs 19% (P<.001).
ESPAC-1's older 5-FU-based CXRT suggested inferior outcomes; here modern CXRT shows no OS harm but no all-comer benefit. Backbone predates FOLFIRINOX-type adjuvant chemo, named in the source as current SOC.
Node-negative benefit rests on a subgroup interaction, not the prespecified primary. Trial underwent multiple mid-course modifications (LAP07, accrual, slow event rate), and no local-control or pattern-of-failure endpoint is reported despite RT's locoregional rationale.
Clean negative primary OS (HR 0.96) reinforces no routine adjuvant CXRT; node-negative benefit is a subgroup interaction needing confirmation; gemcitabine backbone predates FOLFIRINOX.
In resected node-negative pancreatic head adenocarcinoma completing adjuvant gemcitabine, this offers a subgroup signal favoring fluoropyrimidine-sensitized CXRT (OS interaction P=.0063); it does not extend to node-positive pts, where CXRT showed no OS or DFS benefit.
- Does node-negative CXRT benefit hold with mFOLFIRINOX backbone? n=770 · primary completion 2028-06 · phase 3 adjuvant CXRT vs chemo, resected high-risk
- Neoadjuvant vs adjuvant CXRT sequencing in node-negative resected pancreas recruiting Preoperative Stereotactic Body Radiation Therapy in Patients With Resectable Pancreatic Cancer Phase 2n=25 · primary completion 2026-09 · preop SBRT then resection in resectable pancreas
- Local-regional control and pattern of failure with modern CXRT n=30 · primary completion 2028-10 · freedom from local failure at 12mo, SBRT
📚 Sources · 📄 1 paper
Abstract
TROG 08.03 RAVES QOL Substudy
ForPost-RP prostate cancer with adverse pathology or PSA >0.2 ng/ml
TL;DRAt 5yr, 16% vs 2% severe urinary leakage aRT vs no RT (p=0.01); sRT timing had no QOL effect.
The mechanism of sRT's benefit is sparing, not delay: time from RP to RT showed no association with any QOL domain at 3-5 yr (all coefficients ns), and irradiated sRT pts looked like aRT pts. The gain sits entirely with the men who never need RT, so late salvage confers no functional dividend over early salvage.
9 details 4 trials watching
Planned secondary analysis of the TROG 08.03 RAVES randomised trial comparing adjuvant RT with salvage RT delivered at PSA >0.2 ng/ml after radical prostatectomy. Patient-reported QOL collected prospectively across multiple Australian and New Zealand sites.
EORTC QLQ-C30 and QLQ-PR25. The unit of analysis is a minimal clinically important change (MCIC), a decline of >0.5 SD from baseline, in bowel symptoms, urinary symptoms, sexual activity, and sexual functioning.
The aRT arm (n=166) reported more bowel-symptom MCIC at 1-5 yr than sRT pts who never required RT. Against pts in the sRT group who did receive RT, no consistent differences in urinary, bowel, or sexual domains emerged.
| Timepoint | Adjuvant RT | No RT | p |
|---|---|---|---|
| 4 yr | 15/124 (12%) | 1/59 (1.7%) | 0.02 |
| 5 yr | 18/111 (16%) | 1/50 (2%) | 0.01 |
| Domain / timepoint | aRT | sRT | p |
|---|---|---|---|
| Sexual activity MCIC, 3 yr | 32% | 58% | 0.004 |
| Sexual activity MCIC, 4 yr | 43% | 65% | 0.038 |
| Urinary symptom MCIC, 2 yr | 23% | 38% | 0.036 |
| Severe urinary leakage, 5 yr | 16% | 13% | 0.7 |
Dose, fractionation, and target volume are not reported in the source text. Median follow-up from RT was 2.6 yr in the salvage group who received RT (IQR 1.2-5.2), and aRT pts started RT younger (63.9 vs 66.8 yr, p=0.01).
Self-reported QOL in an unblinded trial, so expectancy cuts toward the arm that knows it was irradiated. Denominators thin sharply by 5 yr (23 sRT pts post-RT; 8 in the no-RT sexual-functioning group), and the scattered significant timepoints in the aRT-vs-sRT comparison are fragile at that N.
Reframes the early-salvage rationale: the QOL dividend is sparing roughly the share of men who never trigger RT, not delaying exposure. That matters because delay was the intuitive mechanism, and the regression data do not support it.
Prespecified secondary QOL analysis of a randomised trial; supports the already-guideline-endorsed early-salvage strategy. Small late-timepoint denominators and unblinded self-report temper it.
In post-RP men with adverse pathology deciding adjuvant versus PSA-triggered salvage, this supports counselling that the QOL advantage comes from avoiding RT altogether rather than from postponing it; it does not inform men who already have a rising PSA and will be irradiated either way.
- Does hypofractionated post-prostatectomy RT alter the late incontinence signal? recruiting Hypofractionated Post-prostatectomy Radiotherapy (HYPORT)for Localized Prostate Cancer Phase NAn=428 · primary completion 2026-02 · hypofx vs conventional post-RP RT, safety endpointn=538 · primary completion 2029-09 · phase 3 hypofx vs conventional salvage bed RT
- Does PSMA-guided salvage timing change functional outcomes? recruiting PSMA-PET Guided De-escalation of Salvage Radiation Treatment in Recurrent Prostate Cancer Phase 2n=54 · primary completion 2029-09 · PSMA-guided de-escalated SRT; 1° EP acute G≥2 toxn=380 · primary completion 2032-12 · eSRT at PSA 0.2 vs dSRT 0.4-0.5; safety endpoint
📚 Sources · 📄 1 paper
HYDRA
ForLocalised prostate cancer, definitive EBRT, moderately hypofractionated
TL;DRNo PFS difference vs conventional RT for either MHFRT type, but dose-escalated MHFRT alone raised late G2+ GI + bowel-QoL decrement; isodose 60/20 clean.
The split that matters: dose-escalated MHFRT raised late G2+ GI (OR 1.48, p=0.0035) and patient-reported bowel decrement (OR 1.68, p=0.023), while isodose 60/20 stayed clean on every toxicity and QoL axis at equal PFS. Escalating buys no efficacy, so default to isodose MHFRT.
8 details 5 trials watching
IPD meta-analysis of 7 phase 3 RCTs (MARCAP consortium) of CFRT vs MHFRT. Primary efficacy endpoint PFS; co-primary toxicity late G2+ GU and G2+ GI; co-primary PRO urinary/bowel QoL decrement. Two prespecified strata: isodose vs dose-escalated MHFRT.
Localised prostate cancer. CFRT arm required modern dose (≥70 Gy in 2 Gy equivalents); trials lacking published IPD efficacy or late-toxicity data excluded. 3454 pts across 3 isodose trials, 2426 pts across 4 dose-escalated trials.
Isodose MHFRT exemplified by 60 Gy in 20 fractions; dose-escalated MHFRT schedules pooled (specific fractionations not given in source). Median follow-up 5.4 y (isodose) and 7.1 y (dose-escalated).
Efficacy equivalent to CFRT for both strata. The only toxicity separations were in the dose-escalated arm, late G2+ GI and bowel QoL, not isodose (see table).
Reinforces isodose 60/20 (CHHiP-type) as the standard MHFRT regimen and argues against dose-escalating hypofractionated schedules, which buy no efficacy but cost bowel toxicity.
Physician-scored late toxicity carries grading subjectivity, though PRO data corroborate the bowel signal. Dose-escalated stratum pools heterogeneous fractionation; longer follow-up needed to confirm late-toxicity divergence.
IPD meta-analysis of 7 phase 3 RCTs consolidating isodose 60/20 as standard MHFRT; reinforces current practice, no efficacy gained by dose-escalating.
In localised prostate cancer choosing moderate hypofractionation, this supports isodose 60 Gy/20 fx over dose-escalated hypofractionated schedules; it does not speak to SBRT/ultrahypofractionation or node-positive disease.
- Late-toxicity divergence with follow-up beyond 7 years
- Whether ultrahypofractionation (SBRT) shares the dose-escalation toxicity penalty n=54 · primary completion 2027-02 · 2-fx MR-linac dose de-escalation vs bowel/GU toxicityn=42 · primary completion 2028-01 · 40Gy/5fx SABR, GI/GU vs historical rates
- Optimal dose-escalated schedule if used in higher-risk disease active Comparative Study of Radiotherapy Treatments to Treat High Risk Prostate Cancer Patients Phase 3n=307 · primary completion 2026-12 · HDR boost vs hypofx dose-escalation, high-riskrecruiting Hypofractionated Radiotherapy With a Focal Microboost for High-Risk and Locally Advanced Prostate Cancer Phase 2n=46 · primary completion 2029-01 · hypofx focal microboost, high/very-high riskrecruiting Tumor-directed Radiation Therapy for Patients With the Highest Risk Category of Localized Prostate Cancer Phase NAn=76 · primary completion 2031-09 · ultra-hypofx boost + nodal RT, very high-risk
📚 Sources · 📄 1 paper
Abstract
NRG-GU005
ForLocalized intermediate-risk prostate cancer, definitive RT candidates
HR 1.38
95% CI 0.91-2.09, p=0.13; DFS superiority not met (futility crossed)
TL;DRDFS superiority not met (HR 1.38, futility crossed); SBRT improved 2y bowel QoL (35% vs 44% MCID decline, p=0.034) vs MH-IMRT.
Reported via UroToday →
The urinary-irritation co-primary SBRT was powered for came back flat (35% vs 34%, p=0.68); the QoL edge is bowel and incontinence, not irritation. DFS superiority failed and 3y biochemical failure ran numerically higher on SBRT (8% vs 4%), so the case for 5-fx SBRT is convenience and lower GU/bowel toxicity, not better control.
8 details 3 trials watching
Phase 3, randomized, non-blinded, international; N=698 (SBRT 353 / MH-IMRT 345). Co-primary: disease-free survival (superiority) and EPIC-26 bowel + urinary-irritation QoL at 24 mo. Interim futility analyses prespecified.
Localized intermediate-risk prostate cancer, median age 68. Stratified by Gleason score, PSA, and rectal manipulation (SpaceOAR in ~55%).
SBRT 36.25 Gy/5 fx (7.25 Gy/fx, 2-3×/wk) vs MH-IMRT 70 Gy/28 fx or 60 Gy/20 fx. CTV = prostate ±1 cm proximal SV; SBRT PTV margin 5 mm radial / 3 mm AP. Fiducials, MRI fusion, daily IGRT mandated.
Co-primary DFS powered for a 38% relative improvement (target HR 0.62). Co-primary QoL: absolute reduction in MCID for EPIC bowel (≥4) and urinary irritation/obstruction (≥5) at 24 mo.
DFS superiority not met (futility bound crossed); QoL split, bowel favored SBRT while urinary irritation did not. Effect sizes in the tables above.
| Endpoint | SBRT | MH-IMRT | Effect / p |
|---|---|---|---|
| 5y DFS | 89% (85-92%) | 92% (89-95%) | HR 1.38 (0.91-2.09), p=0.13 |
| 3y cum. biochemical failure | 8% (5.2-11.0) | 4% (2.3-7.0) | p=0.037 |
| 5y OS | 91% (85-95%) | 94% (90-97%) | p=0.66 |
| Domain · MCID decline | SBRT | MH-IMRT | p |
|---|---|---|---|
| Bowel, 2y | 35% | 44% | 0.034 |
| Urinary irritation/obstruction, 2y | 35% | 34% | 0.68 |
| Bowel, 1y | 33% | 46% | 0.002 |
| Sexual, 1y | 34% | 44% | 0.026 |
| Urinary incontinence, 2y | 26% | 35% | 0.023 |
| AE (any grade unless noted) | SBRT | MH-IMRT | p |
|---|---|---|---|
| G≥3 GU | 0.6% | 2.5% | 0.04 |
| Rectal hemorrhage | 10.5% | 17.3% | 0.01 |
| Fatigue | 39.2% | 50.8% | 0.0025 |
Investigator-reported toxicity favored SBRT: fewer G≥3 GU events, less rectal hemorrhage, less fatigue (all p<0.05). Table above.
Consistent with PACE-B: both show lower urinary-incontinence decline with SBRT vs MH-IMRT. MH-IMRT SOC anchored by RTOG 0415.
Non-blinded, so patient-reported QoL endpoints are unblinded. SBRT was designed to prove superiority and failed it; 3y biochemical failure ran numerically higher with SBRT.
Prespecified phase III; SBRT failed DFS superiority (futility crossed) and did not beat MH-IMRT on the urinary-irritation co-primary. Confirms SBRT as a safe equivalent option, not an upgrade.
In localized intermediate-risk prostate cancer weighing definitive RT fractionation, this supports 5-fraction SBRT as a shorter option with comparable disease control and a bowel and GU-toxicity edge over moderate hypofractionation; it does not establish SBRT as more effective.
- Durability of SBRT biochemical control beyond 3 years n=310 · primary completion 2025-12 · phase 3 prostate SBRT, bDFS primary endpoint
- Whether rectal spacer drives the bowel QoL benefit n=150 · primary completion 2027-09 · perirectal spacer efficacy in localized prostate RTn=500 · primary completion 2027-12 · SpaceOAR Vue for late GI toxicity in prostate SBRT
📚 Sources · 📄 2 papers
Abstract
Abstract
EORTC 22033-26033
ForHigh-risk WHO grade 2 low-grade glioma, first-line
No PFS or OS difference between arms
ns regardless of molecular subtype
TL;DRNo PFS/OS difference between first-line RT and TMZ in high-risk WHO grade 2 LGG; only IDH-wildtype favored TMZ (HR 0.47).
Upfront RT (28 × 1.8 Gy) and TMZ were survival-equivalent in every IDH-mutant subtype, including radiosensitive codeleted oligodendroglioma (OS 12.9 vs 14.9 yr, HR 0.88). The lone modality signal favored TMZ in IDH-wildtype (OS 4.7 vs 2.5 yr, HR 0.47), so molecular status, not modality, gates the first-line choice; combined-modality is now standard for IDH-mutant astrocytoma.
6 details 2 trials watching
Phase 3 RCT (EORTC 22033-26033 with NCIC-CTG/TROG/MRC-CTU), N=478 clinical high-risk WHO grade 2 LGG, randomized to RT vs dose-dense TMZ. Mature results, with post-hoc 2021 WHO molecular reclassification in 73% (351/478).
RT 28 × 1.8 Gy, standard fractionation, as the single-modality comparator arm.
Dose-dense TMZ 75 mg/m² once daily, 21 of 28 days, up to 12 cycles.
Primary: progression-free survival; overall survival co-reported. No significant difference in PFS or OS between arms.
Neither PFS nor OS differed by arm overall; molecular-subgroup OS is in the detail table, with only IDH-wildtype favoring TMZ.
| Subgroup (2021 WHO), n | RT OS | TMZ OS | HR (95% CI), p |
|---|---|---|---|
| Astrocytoma IDHmt non-codel, n=178 | 6.6-6.7 yr | 6.6-6.7 yr | HR CI 0.67-1.44, P=.93 |
| Oligo IDHmt codel, n=109 | 12.9 yr (9.4-NR) | 14.9 yr (10.1-NR) | 0.88 (0.52-1.49), P=.63 |
| IDH-wildtype, n=64 | 2.5 yr (1.8-3.3) | 4.7 yr (2.2-7.2) | 0.47 (0.27-0.82), P=.0068 |
Combined-modality (RT + chemo) was not tested here but has since become standard for IDH-mutant astrocytoma (e.g. RTOG 9802, RT+PCV).
Molecular subtypes are post-hoc reclassification (tissue in 73%); the IDH-wildtype subgroup is small (n=64). Combined-modality untested.
Mature phase 3; the null modality comparison confirms combined-modality's rise as SOC. Molecular subgroups reclassified post-hoc, so no single-modality practice change lands.
In high-risk WHO grade 2 IDH-mutant glioma, this supports that first-line RT versus TMZ monotherapy does not change PFS or OS; it does not extend to IDH-wildtype tumors, where a small post-hoc subgroup favored TMZ.
- Combined-modality vs single-modality first-line in IDH-mutant low-grade glioma active Radiation Therapy With or Without Temozolomide in Treating Patients With Low-Grade Glioma Phase 3n=540 · primary completion 2026-12 · phase 3 RT vs RT+TMZ, grade 2 glioma
- Does temozolomide outperform RT in IDH-wildtype grade 2 glioma? recruiting Chemotherapy and Radiation Therapy for the Treatment of IDH Wildtype Gliomas or Non-histological (Molecular) Glioblastomas Phase 2n=40 · primary completion 2026-12 · TMZ+RT in IDH-wildtype lower-grade glioma
📚 Sources · 📄 1 paper
Abstract
ENZARAD (ANZUP 1303)
ForHigh-risk clinically-localized/locally-advanced prostate, EBRT + 2yr ADT
8yr 74% vs 72%, HR 0.88
95% CI 0.67-1.15, p=0.34; 1° endpoint not met
TL;DRMFS 8yr 74% vs 72%, HR 0.88 (0.67-1.15) p=0.34; enza on an RT+ADT backbone missed 1° endpoint, benefit isolated to cN1/pelvic-RT.
Reported via UroToday →
The intensification benefit tracks the pelvic-RT-planned subgroup (MFS HR 0.47, OS HR 0.53), but that arm was enriched for cN1 (28% vs 0%), so nodal burden, not the RT field itself, likely drives it. Planning whole-pelvis RT for cN1 disease is where adding enzalutamide over 6mo NSAA earns its place; cN0 pts gained nothing.
8 details
Phase 3 open-label RCT, N=802 across 8 countries (2014-2018), median follow-up 8 years. Primary: metastasis-free survival (switched from OS mid-trial for fewer-than-expected deaths). Enzalutamide 160mg × 24mo vs conventional NSAA × 6mo, both on 24mo LHRH agonist + EBRT.
High-risk clinically-localized or locally-advanced prostate, EBRT-suitable. 90% Gleason 8-10, 36% PSA >20, 12% cN1 by conventional imaging. 40% planned pelvic RT, 8% brachytherapy boost.
Prostate to 78Gy, or 46Gy + brachy boost. Pelvic nodal RT 46Gy elective + boost to gross nodes, required for cN1, optional (pre-declared) for cN0. Intensive QA: credentialing, real-time review of first 5 plans per site, 20% sampling thereafter.
Primary MFS not met; PFS positive, OS neutral; benefit isolated to the cN1 and pelvic-RT-planned subgroups (see tables).
| Endpoint | Enza | Control | HR (95% CI), p |
|---|---|---|---|
| MFS (1°) | 74% | 72% | 0.88 (0.67-1.15), p=0.34 |
| PFS | 67% | 62% | 0.78 (0.61-0.99), p=0.044 |
| OS | 83% | 80% | 0.87 (0.63-1.20), p=0.40 |
| Subgroup | MFS HR (95% CI) | OS HR (95% CI) |
|---|---|---|
| cN1 nodal | 0.43 (0.20-0.92) | 0.46 (0.17-1.26) |
| Pelvic RT planned | 0.47 (0.29-0.76) | 0.53 (0.30-0.95) |
| Very high-risk | 0.85 (0.64-1.13) | 0.81 (0.57-1.13) |
| STAMPEDE | ENZARAD | |
|---|---|---|
| cN1 | 39% | 11% |
| Median PSA | 35 ng/ml | 14 ng/ml |
| cT3-4 | 92% | 47% |
| Overall MFS HR | 0.53 | 0.88 |
The cN1 MFS benefit mirrors STAMPEDE abiraterone; the weaker overall effect reflects ENZARAD's more favorable baseline risk (lower cN1 fraction, lower PSA, less cT3-4).
Active NSAA control (not placebo) narrows the measured enzalutamide effect. Subgroup benefits are prespecified but hypothesis-generating, and the pelvic-RT arm is confounded by nodal enrichment. Primary endpoint switched from OS to MFS mid-trial.
Phase 3, prespecified MFS primary, 8yr f/u, active-NSAA control; negative overall reinforces restrained intensification, cN1/pelvic-RT benefit mirrors STAMPEDE. Subgroups prespecified, not practice-defining alone.
In high-risk localized prostate with cN1 disease or planned pelvic-nodal RT, the data support enzalutamide intensification over 6mo NSAA; it does not extend to cN0 pts, who showed no MFS benefit.
- Which pelvic-RT subgroups drive the enzalutamide benefit
- Biomarkers to identify who needs treatment intensification
- Does nodal RT sterilization enable enzalutamide's distant-metastasis benefit
📚 Sources · 📄 1 paper
Abstract
RADIOSA NCT03940235
ForMetachronous oligorecurrent HSPC, ≤3 lesions, post-radical local tx
TL;DRmcPFS 32.2 vs 15.1mo, HR 0.43 (0.26-0.72), p=0.001 adding 6mo ADT to metastasis-directed SBRT in oligorecurrent HSPC.
Surfaced from a review's discussed trials
Both arms get ablative SBRT (30 Gy/3fx, BED >100 Gy) to all sites, so the trial isolates the 6-mo ADT add-on, not SBRT's own contribution (no observation arm). The decision it moves: whether to layer short ADT onto metastasis-directed SBRT. SBRT alone still gave 15.1-mo cPFS in selected pts.
Also covered May 17
8 details 2 trials watching
Single-centre, randomised, open-label phase 2 (European Institute of Oncology, Milan). N=105 randomised 1:1 (52 SBRT alone, 53 SBRT+ADT); modified ITT, 51/arm analysed. Median follow-up 31 mo.
Metachronous oligorecurrent hormone-sensitive prostate cancer after radical local treatment; ≤3 lesions (pelvic/extra-regional nodal or bone) on PSMA-PET or MRI; ECOG 0-1; median age 70. Stratified by PSMA-DT (≤3 vs >3 mo), site (node vs bone), imaging.
SBRT 30 Gy in 3 fractions every other day (EQD2 98.6 Gy at α/β 1.5, BED >100 Gy), or equivalent by site. All oligometastatic sites treated in both arms.
The SBRT+ADT arm added 6 months of LHRH-analogue ADT starting within 1 week before SBRT.
Primary: clinical progression-free survival. OS and time-to-CRPC were not the primary read.
Adding short ADT roughly doubled median cPFS; effect sizes in the results table.
Near-absent RT toxicity: 1 G1 GI, 1 G3 GU (left ureter stenosis, SBRT+ADT), no late effects. ADT added 22 G1 AEs, all resolved. No treatment-related deaths.
First RCT of adding short ADT to MDT in metachronous oligorecurrent HSPC. STOMP/ORIOLE established MDT vs observation; RADIOSA instead isolates the ADT add-on onto an SBRT backbone.
Single-centre, open-label, N=105. Primary endpoint is clinical PFS, a surrogate; ADT's own progression-delaying effect confounds the SBRT+ADT arm. Optimal ADT duration untested.
Single-centre open-label phase 2, N=105; 1° EP is clinical PFS (surrogate), not OS. Consistent with STOMP/ORIOLE MDT signals; not definitive enough to change practice.
In metachronous oligorecurrent hormone-sensitive prostate cancer with ≤3 lesions on PSMA-PET, this supports adding 6 mo ADT to metastasis-directed SBRT for longer cPFS; it does not address synchronous or polymetastatic disease, and SBRT alone remains reasonable in carefully selected pts.
- Optimal duration of ADT added to SBRT active Androgen Deprivation Therapy for Oligo-recurrent Prostate Cancer in Addition to radioTherapy Phase 3n=280 · primary completion 2027-10 · phase 3 ADT added to MDRT vs MDRT alonen=532 · primary completion 2031-02 · tests timing of ADT+ARPI added to SBRT in mHSPC
- Biomarkers predicting benefit from SBRT alone
- Whether cPFS gain translates to OS or delayed CRPC
📚 Sources · 📄 1 paper
Abstract
WOLVERINE
ForOligometastatic prostate cancer (≤5 mets), predominantly castration-sensitive
TL;DRPFS HR 0.44, rPFS HR 0.60 favor MDT added to SOC in oligomet prostate; OS HR 0.63 non-sig (p=0.051).
Surfaced from a review's discussed trials
MDT here is predominantly SBRT, and the RT-attributable read is that benefit held in the sensitivity analysis excluding observation-only-SOC trials (PFS HR 0.46, CRFS HR 0.46), so MDT adds on a systemic backbone, not just vs nothing. OS stayed non-significant (HR 0.63, p=0.051): the gain is delaying progression and castration resistance, not proven survival.
7 details 5 trials watching
IPD meta-analysis (PROSPERO CRD42023479078) of 7 phase 2 RCTs; the primary MDT-efficacy analysis pooled 6 trials randomizing 472 men to MDT+SOC (n=248) vs SOC (n=224). Median follow-up 40.7 mo (IQR 25.6-53.7).
Oligometastatic (up to 5 mets) prostate cancer; 65% castration-sensitive (n=375), ARTO entirely CRPC and EXTEND baskets CRPC-enriched. 85.5% (n=491) had prior definitive local therapy; median PSA 1.9 both arms.
MDT is delivered per each component trial (EXTEND, STOMP, ORIOLE, ARTO, COMET-SABR), predominantly SBRT-based. Dose, fractionation, target volume, and modality breakdown are not reported in this meta-analysis, so the technique-transfer question can't be answered from source.
Coprimary: PFS and OS. Secondary: rPFS and castration resistance-free survival (CRFS).
MDT plus SOC improved PFS, rPFS, and CRFS across both trial- and patient-level analyses; overall survival did not reach significance (effect sizes in the table above).
STOMP and ORIOLE (observation-controlled SBRT trials) drove the early MDT signal; this pooled IPD extends the PFS/CRFS benefit across 6 trials and shows it persists on a systemic-therapy backbone in the observation-excluded sensitivity analysis.
All 7 component trials are phase 2 with non-blinded randomization ('some concerns' RoB) and open-label PSA-driven endpoints. OS non-significant (p=0.051). SOC arm slightly older (71 vs 68) and more often on 2nd-gen ARPI (59.8% vs 50.4%).
IPD meta-analysis of 6 phase-2 non-blinded RCTs; PFS/rPFS/CRFS clearly hit but OS non-significant. Reinforces the emerging MDT-for-oligomet signal (STOMP, ORIOLE), doesn't establish survival.
In castration-sensitive oligometastatic prostate cancer, up to 5 mets and mostly post definitive local therapy, the pooled evidence supports MDT plus SOC to delay progression and castration resistance; it does not establish a survival benefit nor extend to the CRPC-predominant setting.
- Does MDT extend overall survival in oligometastatic prostate cancer? active Prostate-cancer Treatment Using Stereotactic Radiotherapy for Oligometastases Ablation in Hormone-sensitive Patients Phase 3n=550 · primary completion 2026-06 · phase 3 SBRT + SOC vs SOC in oligomet HSPCrecruiting Veterans Affairs Seamless Phase II/III Randomized Trial of STAndard Systemic theRapy With or Without PET-directed Local Therapy for Oligometastatic pRosTate Cancer Phase 2/3n=464 · primary completion 2026-09 · phase 2/3 systemic ± PET-directed local therapy
- Optimal MDT (SBRT) target volume and dose across trials recruiting HIghly MetAstatic Life Prolonging Therapy-Resistant Prostate Cancer: Role of Stereotactic Radiotherapy for Bone and Lymph Node Metastases (HIMARS) Phase NAn=18 · primary completion 2028-05 · phase 1 max-tolerated-volume SBRT escalationrecruiting OligoCare TwiCs (Trials Within Cohorts) Trial Comparing Acute Toxicity in Single-fraction vs Multiple-fraction SBRT for Metastasis-directed Treatment (SPRINT) Phase NAn=302 · primary completion 2029-02 · single- vs multi-fraction SBRT for mets
- MDT benefit in CRPC vs castration-sensitive disease recruiting Metastasis-directed Therapy in Oligoprogressive Castration-refractory Prostate Cancer Phase 3n=246 · primary completion 2029-01 · phase 3 MDT in oligoprogressive CRPC
📚 Sources · 📄 1 paper
Abstract
ARTO NCT03449719
ForOligometastatic CRPC, ≤3 nonvisceral mets, first-line abiraterone
92% vs 68.3%
OR 5.34 (95% CI 2.05-13.88), P=.001
TL;DRAdding SBRT to abiraterone lifted 6-mo PSA response to 92% vs 68.3% (OR 5.34) and cut progression (PFS HR 0.35) in oligomet CRPC.
Surfaced from a review's discussed trials
The RT read is total metastatic consolidation: SBRT to all ≤3 CRPC sites concurrent with abiraterone more than doubled complete PSA response (56% vs 23.2%) and cut progression risk (HR 0.35). It pushes MDT beyond hormone-sensitive oligomet (ORIOLE/STOMP) into first-line CRPC, moving the decision to irradiate every lesion, not defer.
Also covered Jul 7
6 details 5 trials watching
Multicenter randomized phase II, 1:1, N=157, enrolled Jan 2019-Sep 2022. Primary: 6-month biochemical response.
Oligometastatic castration-resistant prostate cancer with ≤3 nonvisceral metastatic lesions, in the first-line abiraterone setting.
Both arms received abiraterone acetate + prednisone (AAP). The experimental arm added concomitant SBRT.
SBRT to all sites of disease, concomitant with AAP. Dose/fractionation not reported in source.
Primary: biochemical response (PSA drop ≥50% at 6mo). Secondary: complete BR (PSA <0.2 ng/mL), PFS.
Primary endpoint and PFS both met, favoring the SBRT arm (see results table).
| Endpoint (6mo) | AAP+SBRT | AAP alone | Effect size |
|---|---|---|---|
| Biochemical response (PSA ≥50% drop) | 92% | 68.3% | OR 5.34 (2.05-13.88), P=.001 |
| Complete BR (PSA <0.2 ng/mL) | 56% | 23.2% | OR 4.22 (2.12-8.38), P<.001 |
Extends the metastasis-directed SBRT benefit seen in ORIOLE/STOMP (hormone-sensitive oligomet) into first-line CRPC.
Phase II, N=157. Primary endpoint is a PSA surrogate with no OS reported; dose/fractionation and long-term durability not in source.
Randomized phase II, primary hit, named comparator (AAP alone); primary is a PSA surrogate, so supportive of the emerging oligomet MDT paradigm rather than practice-setting.
In oligometastatic CRPC (≤3 nonvisceral mets) starting first-line abiraterone, this supports adding SBRT to all sites for deeper PSA response and longer PFS; it does not extend to visceral or polymetastatic disease.
- OS benefit of adding SBRT in oligomet CRPC recruiting Metastasis-directed Therapy in Oligoprogressive Castration-refractory Prostate Cancer Phase 3n=246 · primary completion 2029-01 · phase 3 MDT vs SOC in oligoprogressive CRPCrecruiting Treatment With Darolutamide +/- Radiation Therapy for Patients With a Castration Resistant Cancer and Metastases Detected by Functional Imaging Phase 3n=336 · primary completion 2029-10 · phase 3 darolutamide ± SBRT in metastatic CRPC
- Optimal SBRT dose/fractionation for CRPC metastases recruiting OligoCare TwiCs (Trials Within Cohorts) Trial Comparing Acute Toxicity in Single-fraction vs Multiple-fraction SBRT for Metastasis-directed Treatment (SPRINT) Phase NAn=302 · primary completion 2029-02 · single- vs multi-fraction SBRT for oligomets
- Does MDT delay next systemic therapy in CRPC? n=102 · primary completion 2027-04 · SBRT to postpone 2nd-line systemic tx in CRPCn=66 · primary completion 2030-11 · SBRT + darolutamide to defer 2nd-line in M0CRPC
📚 Sources · 📄 1 paper
Abstract
NRG Oncology/RTOG 0848 NCT01013649
ForResected pancreatic head adenocarcinoma, post adjuvant gemcitabine-based chemo
HR 0.96
90% CI 0.79-1.18, p=0.38 (1-sided log-rank); primary OS endpoint not met
TL;DROS HR 0.96 (90% CI 0.79-1.18), p=0.38: adjuvant chemoRT adds no OS benefit over chemo alone after pancreatic head resection.
The RT read is the node-negative subgroup: 5-yr OS 28.6→48.1% and median OS 3.0→3.9 yr with added CXRT (interaction p=0.022), while node-positive pts gained nothing (21.2 vs 20.9%). Subgroup-only (n=91), but it isolates who might still warrant adjuvant CXRT once modern systemic therapy is optimized.
7 details 3 trials watching
RT randomization of NRG/RTOG 0848 phase 3. After curative-intent resection and adjuvant gemcitabine-based chemo without progression, N=354 randomized to no further therapy (n=174) vs fluoropyrimidine-sensitized CXRT (n=180). Primary: overall survival.
Resected pancreatic head adenocarcinoma; mix of N0 (n=91) and N1 (n=263), predominantly T3 (n=288 vs T1/T2 n=66), mostly negative margins (n=295). Only pts completing adjuvant chemo without progression.
Adjuvant systemic backbone gemcitabine-based: gemcitabine alone (n=236), non-oxaliplatin gemcitabine combinations (n=18), gemcitabine+erlotinib (n=100). Added arm was fluoropyrimidine-sensitized CXRT.
CXRT was fluoropyrimidine-sensitized chemoradiotherapy delivered after completion of adjuvant chemo. RT dose, fractionation, and target volume not reported in source text.
Primary: overall survival. Prespecified 5-yr OS subgroup estimates with interaction tests by nodal status, T stage, margins, CA19-9, sex, age, and systemic regimen.
Primary OS negative: HR 0.96 (90% CI 0.79-1.18), p=0.38; median OS 2.6 vs 2.3 yr. Nodal-status interaction p=0.022 with a node-negative gain (see table).
| Nodal status | Chemo 5-yr OS | Chemo+CXRT 5-yr OS |
|---|---|---|
| N0 (n=91) | 28.6% (14.9-42.2) | 48.1% (33.3-62.9) |
| N1 (n=263) | 21.2% (13.8-28.5) | 20.9% (13.8-28.0) |
| Endpoint | Chemo | Chemo+CXRT |
|---|---|---|
| Median OS | 3.0 yr (2.2-4.0) | 3.9 yr (2.5-NR) |
| Median DFS | 1.5 yr (0.8-2.7) | 2.3 yr (1.4-NR) |
Gemcitabine backbone predates FOLFIRINOX-era adjuvant standard; authors note the node-negative signal needs confirmation in trials using FOLFIRINOX/FOLFOXIRI.
Node-negative OS benefit is a subgroup finding (n=91, interaction p=0.022), hypothesis-generating. Dated gemcitabine backbone; RT technique not reported in source.
Prospective phase III, primary OS endpoint not met (HR 0.96); reinforces omitting adjuvant CXRT. Node-negative benefit is subgroup-only (interaction p=0.022), needs independent confirmation.
In resected pancreatic head adenocarcinoma who completed adjuvant gemcitabine-based chemo, this supports omitting fluoropyrimidine-sensitized CXRT overall and in node-positive pts; the node-negative subgroup gain is hypothesis-generating, not yet grounds to add RT.
- Does adjuvant CXRT benefit node-negative resected pancreatic cancer? n=770 · primary completion 2028-06 · phase 3 adjuvant chemoRT vs chemo, resected PDACrecruiting Radiotherapy With GX Regimen as Adjuvant Therapy for High-risk Patients Following Pancreatic Cancer Surgery Phase 3n=288 · primary completion 2029-05 · phase 3 adjuvant RT+chemo vs chemo alone
- Confirmation with modern FOLFIRINOX adjuvant backbone active Testing the Use of the Usual Chemotherapy Before and After Surgery for Removable Pancreatic Cancer Phase 3n=358 · primary completion 2028-12 · peri-op vs adjuvant FOLFIRINOX, resectable PDAC
📚 Sources · 📄 1 paper
RTOG 0539 NCT00895622
ForWHO grade 1-3 meningioma, post-resection, newly diagnosed or recurrent
TL;DR10-yr PFS 72.2% intermediate-risk (54Gy) and 42.5% high-risk (60Gy) meningioma on adjuvant RT; low-risk observed 85.2%.
The RT read is patient selection: low-risk grade 1 (GTR/STR) observed carried only 8.9% 10-yr cumulative progression, backing omission, while intermediate-risk earns 54Gy/30fx adjuvant. High-risk 60Gy still leaves 39.3% 10-yr progression, marking the ceiling of adjuvant RT alone in grade 2/3 disease.
7 details 5 trials watching
Prospective phase 2, multi-institutional (NRG/RTOG), risk-adapted by WHO grade, extent of resection, and recurrence status. 244 consented, 165 protocol-treated. Central pathology review; data cutoff 8/15/2023.
Adults ≥18, Zubrod 0-1, histologically confirmed unifocal WHO grade 1-3 meningioma, any resection extent. Low-risk n=60, intermediate n=52, high-risk n=53.
Intermediate-risk 54 Gy and high-risk 60 Gy, both in 30 fractions, adjuvant. Low-risk received no RT (observation). No hypofractionation or SRS arm.
Primary (3-yr PFS) reported previously. This analysis reports long-term PFS, OS, and cumulative incidence of progression (competing-risk) at ~12-yr median follow-up.
Per-cohort 10-yr PFS, OS, and cumulative-incidence values are in the table above. Median PFS not reached for low- and intermediate-risk.
| Cohort (management) | 10-yr PFS | 10-yr OS | 10-yr cum. incidence progression |
|---|---|---|---|
| Low-risk, observed | 85.2% | 94.1% | 8.9% (3.2-18.2) |
| Intermediate, 54Gy | 72.2% | 84.7% | 21.2% (10.8-33.9) |
| High-risk, 60Gy | 42.5% | 51.1% | 39.3% (25.8-52.5) |
RT-attributable grade 3+ toxicity 9.6% (intermediate, 5/52) and 15.1% (high-risk, 8/53). The observed low-risk cohort carried no RT toxicity.
No randomised RT-vs-observation trial in grade 2 meningioma has reported. ROAM/EORTC-1308 and NRG-BN003 (GTR grade 2) remain open; RTOG 0539 is the prospective benchmark.
Each risk cohort is single-arm, no randomised RT-vs-observation comparison; modest per-cohort N (~50-60); grading predates molecular integration into WHO CNS grading.
Prospective multi-institutional risk-adapted phase 2, 12-yr mature f/u, sets RT patient-selection benchmark. Each cohort single-arm; no randomised RT-vs-observation comparison.
In newly diagnosed grade 1 meningioma after gross or subtotal resection, this supports observation over adjuvant RT; it does not soften the case for 54-60Gy in recurrent grade 1, grade 2, or grade 3 disease.
- Randomised confirmation of RT omission after GTR of grade 2 meningioma not yet Efficacy of Postoperative Radiotherapy for Atypical Meningioma Without Venous Sinus Invasion After Gross-total Resection Phase NAn=140 · primary completion 2028-01 · postop RT need after GTR of atypical WHO II
- Role of dose escalation or systemic therapy for high-risk (grade 3) disease active An Open-Label Phase II Study of Nivolumab or Nivolumab/Ipilimumab in Adult Participants With Progessive/ Recurrent Meningioma Phase 2n=40 · primary completion 2024-12 · nivo/ipi for progressive/recurrent WHO IIIrecruiting Combination of Everolimus and 177Lu-DOTATATE in the Treatment of Grades 2 and 3 Refractory Meningioma: a Phase IIb Clinical Trial Phase 2n=28 · primary completion 2026-03 · everolimus + Lu-DOTATATE, refractory WHO 2/3active A Trial of Increased Dose Intensity Modulated Proton Therapy (IMPT) for High-Grade Meningiomas Phase NAn=21 · primary completion 2027-08 · IMPT dose intensification for high-grade WHO II/IIIn=90 · primary completion 2028-12 · proton dose escalation 68-72 Gy, WHO II/III
- Molecular grading integration to refine risk stratification
📚 Sources · 📄 1 paper
Abstract
MROQC ADT Practice Patterns
ForHigh-risk M0/N0-1 prostate on definitive RT, GG4-5 predominant
TL;DRGuideline-concordant ADT (≥18mo) recommended in 67.0% of high-risk pts on definitive RT; ARPI intensification just 23.2% of STAMPEDE-eligible.
The RT prescriber's read is the adoption gap, not a treatment effect: even in a quality consortium, only 67.0% of high-risk pts on definitive RT are recommended ≥18mo ADT, and just 23.2% of STAMPEDE-eligible get ARPI intensification. Facility-level variability persists on multivariable analysis (P<.0001), so where a man is treated, not only his risk, sets his ADT. Prompts an audit of your own duration and intensification practice.
8 details
Prospective practice-pattern study within the Michigan Radiation Oncology Quality Consortium (MROQC), a statewide RT registry. 553 pts across 26 centers, Jun 2020–Nov 2024. Facility modeled as a random intercept (mixed-effects).
Intact, high-risk M0/N0-1 prostate cancer on definitive RT. GG4-5 75.0%, PSA ≥20 40.0%, cN1 19.9%, cT3/4 13.3%. 27.9% met STAMPEDE M0 intensification criteria.
Primary: intended guideline-concordant ADT (≥18mo). Also assessed: ARPI adoption before vs after STAMPEDE M0 publication, facility-level variability, and multivariable predictors of concordance.
91.3% recommended any ADT, 67.0% guideline-concordant. ARPI intensification among STAMPEDE-eligible rose 0% → 23.2% post-publication. Facility variability persisted on MVA (P<.0001).
| Factor | OR (GC-ADT) | 95% CI |
|---|---|---|
| cN1 | 2.94 | 1.44-5.99 |
| GG4 | 6.23 | 2.85-13.62 |
| GG5 | 9.45 | 4.46-20.06 |
| PSA ≥40 | 3.64 | 1.22-10.87 |
Benchmarks real practice against the 2022 AUA/ASTRO guideline (18-36mo ADT) and STAMPEDE M0 (ARPI for high-burden high-risk). Documents a persistent adoption gap, not a treatment effect.
Captures intended ADT duration and recommendations, not delivered therapy or adherence. Single-state consortium limits generalizability, and there is no efficacy or outcome endpoint.
Descriptive practice-pattern audit (no efficacy endpoint); reinforces AUA/ASTRO ADT guideline and STAMPEDE M0 as benchmark, documenting under-adoption rather than testing a new effect.
In high-risk men (GG4-5, cN1, PSA ≥40, or ≥2 STAMPEDE factors) starting definitive RT, this supports benchmarking ADT to ≥18mo and weighing ARPI intensification when STAMPEDE-eligible; it does not extend to low/intermediate-risk disease or ADT-omission decisions.
- Does intended guideline-concordant ADT translate to delivered treatment and adherence?
- What interventions reduce facility-level variability in ADT recommendations?
- Do Michigan consortium patterns generalize to national practice?
📚 Sources · 📄 1 paper
Abstract
AREST
ForAdequately resected pT1-2N0 oral SCC with ≥1 intermediate-risk feature
HR 0.52
3-yr LRFS 89.2% vs 80.9%, 95% CI 0.30-0.91, p=0.02 (ITT)
TL;DR3-yr LRFS 89.2% vs 80.9%, HR 0.52 (0.30-0.91) p=0.02 favoring adjuvant RT in resected intermediate-risk pT1-2N0 oral SCC; no OS/DFS gain.
The move is observe-vs-treat in adequately resected pT1-2N0 OSCC with one adverse feature: 60Gy/30fx to tumor bed plus at-risk neck cut 3-yr loco-regional failure (HR 0.52), strongest in oral tongue over buccal mucosa (exploratory). The gain is loco-regional only, so weigh it against RT morbidity when baseline LRR risk is low.

| Arm | 3-yr LRFS | HR (95% CI) | p |
|---|---|---|---|
| Adjuvant RT | 89.2% (84.3-93.3) | 0.52 (0.30-0.91) | 0.02 |
| Observation | 80.9% (74.6-86.1) | ref | — |
8 details 2 trials watching
Phase 3, open-label, multicenter RCT (India); 1:1 to adjuvant RT vs observation, N=392 (191 RT, 201 observation), stratified by subsite, PNI/LVE, differentiation. Median follow-up 47.2 months.
pT1-2 pN0 OSCC with ≥1 intermediate-risk feature (DOI 5-10mm, PNI, LVE, or poor differentiation), after adequate surgery: margins ≥5mm and ipsilateral level I-III neck dissection with ≥16 nodes.
60Gy in 30 fractions over 6 weeks to the resected tumor bed and at-risk neck nodal region.
Primary: 3-yr loco-regional recurrence-free survival (LRFS), KM with log-rank. Secondary: DFS, OS, and cumulative incidence of loco-regional failure (competing-risk).
Per-protocol LRFS 91.1% vs 80.9%, HR 0.43 (0.23-0.80), p=0.01. DFS and OS not significantly different between arms.
| Analysis | Adjuvant RT | Observation | HR (95% CI), p |
|---|---|---|---|
| ITT | 10.6% (6.1-15.1) | 18.9% (13.3-24.6) | 0.52 (0.30-0.91), p=0.021 |
| Per-protocol | 8.7% (4.3-13.1) | 18.9% (13.3-24.6) | 0.43 (0.23-0.79), p=0.007 |
Prior evidence for adjuvant RT in this pN0 intermediate-risk setting was retrospective (per the abstract); AREST is the first randomized confirmation.
Open-label, abstract-only; benefit is loco-regional control only, no OS/DFS at 47.2-mo median. Observation LRFS (80.9%) exceeded the 70% powering assumption, so the absolute LRFS gain is modest.
First randomized backing for the guideline-listed retrospective signal that RT cuts LRR in adverse-feature pN0 OSCC; loco-regional benefit only, no OS/DFS, open-label abstract.
In an adequately resected pT1-2N0 oral tongue SCC with a single intermediate-risk feature, this supports adjuvant RT for loco-regional control but not survival, and it does not extend to buccal mucosa (weaker signal) or node-positive disease.
- Does loco-regional control benefit translate to survival with longer follow-up? n=85 · primary completion 2026-08 · postop RT vs PD-1 maintenance, survival endpoint
- Optimal adjuvant approach for buccal mucosa vs oral tongue subsites? recruiting A Study of Radiation Therapy After Surgery in People With Oral Tongue Squamous Cell Carcinoma Phase 2n=24 · primary completion 2027-06 · postop IMRT tailored to oral tongue subsite
- Which single intermediate-risk feature drives the RT benefit?
📚 Sources · 🐦 1 tweet · 📄 1 paper
#ASCO26
— Dr Rishabh Jain (@DrRishabhOnco) May 27, 2026
🗣️ The AREST trial tackles one of the biggest gray zones in oral cavity cancer.
After adequate surgery in pT1-2N0 OSCC with intermediate-risk features:
✅ Adjuvant RT improved loco-regional control
❌ No OS benefit observed
3-year LRFS:
🔹 89.2% vs 80.9%
🔹 HR 0.52… https://t.co/qsALPFX032 pic.twitter.com/F4XzTMETih
Abstract
ctDNA and Local Regrowth/Distant Mets in Nonoperative Management of Stage II-III Rectal Cancer
ForMSS stage II-III rectal adenoca in cCR/nCR on watch-and-wait after TNT
TL;DRctDNA sensitivity 41% for local regrowth vs 74% for distant mets; positive result predicts both but can't replace endoscopy/MRI surveillance in rectal NOM.
The asymmetry is the actionable read: ctDNA caught only 41% of local regrowths vs 74% of distant mets, so for post-TNT organ-preservation surveillance it flags distant-met risk but can't replace endoscopy/MRI. ctDNA+ at regrowth also tracked more advanced ypT3-4 salvage pathology (75% vs 21%).

7 details 1 trial watching
Prospective single-center cohort (MD Anderson INTERCEPT program), N=110, 2020-2024. Serial tumor-informed ctDNA (Signatera Exome), 669 samples; median follow-up 25 mo (IQR 18-37).
MSS stage II-III rectal adenocarcinoma in cCR (69) or nCR (41) after NAT, managed non-operatively. Median age 56; cT3 in 72 and cN1-2 in 60 of 110; NAT almost entirely TNT (104/110).
Regrowth-free and distant-metastasis-free survival by longitudinal and first-post-NAT ctDNA; per-sample diagnostic accuracy (±90d of each draw); salvage-surgery pathology by ctDNA status. No registered primary endpoint (observational).
Local regrowth in 23 (21%), distant mets in 12 (11%). Ever-positive ctDNA tracked worse regrowth-free and distant-met-free survival (log-rank p=0.0002 and p<0.0001). Per-sample sensitivity 41% local regrowth vs 74% distant mets.
| Endpoint | Sensitivity | Specificity | Accuracy |
|---|---|---|---|
| Local regrowth | 41% (12/29) | 94% (480/509) | 91% (492/538) |
| Distant metastasis | 74% (31/42) | 97% (611/627) | 96% (642/669) |
Consistent with the emerging ctDNA-as-prognostic signal in rectal NOM, but quantifies a sensitivity ceiling (41%) that limits its use for local-regrowth surveillance.
Single-center, N=110 with only 29 regrowth- and 42 distant-met-associated samples driving diagnostic estimates. Assay-specific (Signatera tumor-informed); no comparison vs imaging-alone surveillance.
Single-center prospective cohort (N=110), no interventional comparator; prognostic association consistent with emerging ctDNA-in-NOM data and reaffirms imaging/endoscopy surveillance can't be replaced.
Applies to the MSS stage II-III rectal pt in cCR/nCR pursuing watch-and-wait after TNT, in whom a negative ctDNA still can't exclude local regrowth; it does not extend to MSI-H tumors or pts not pursuing organ preservation.
- Does ctDNA-guided surveillance improve organ-preservation outcomes vs imaging alone n=100 · primary completion 2025-12 · candidate match
- Can serial ctDNA kinetics raise local regrowth sensitivity above 41%
- Generalizability beyond single-center tumor-informed Signatera cohort
📚 Sources · 🐦 1 tweet
Important study re: ctDNA for non-op surveillance in rectal ca.
— Dr. Nina Niu Sanford (@NiuSanford) June 1, 2026
Pos ctDNA associated w regrowth (60%) & distant mets (60%), but neg ctDNA doesn't exclude local regrowth (sensitivity only 41%)
ctDNA good for risk stratification but not surveillance replacement #ASCO26 @OncoAlert pic.twitter.com/UQQub5QfNB
CAN-2409 NCT01436968
ForIntermediate or high-risk localised prostate cancer, EBRT candidates
TL;DRDFS HR 0.70 (0.52-0.94, p=0.016) adding intraprostatic CAN-2409 to EBRT in intermediate/high-risk localised prostate; OS and PCSM immature.
The RT read is local control: 2yr biopsy positivity fell 36.4% to 19.6% (p=0.0015), comparable to adding ADT (RTOG 9408) but on standard 78Gy without a brachy or SIB boost. Whether it adds over modern dose-intensification plus ADT is the open integration question, since ADT was optional and no boost was used.

| Endpoint | CAN-2409 | Placebo | HR / p |
|---|---|---|---|
| DFS median | NR | 86.1 mo | HR 0.7 (0.52-0.94), p=0.0155 |
| 2yr biopsy pCR | 80.4% | 63.6% | n/a |
| 2yr local recurrence | 19.6% | 36.4% | p=0.0015 |
+1 more figure

| Trial | Intensifier | Local endpoint: control → intensified |
|---|---|---|
| RTOG 9408 | +4mo ADT | 2yr biopsy+ 40% → 20% |
| ASCENDE-RT | LDR brachy boost | 10y local failure 7.1% → 1.5% |
| FLAME | SIB 95Gy | Crude local failure 7.7% → 2.7% |
| CAN-2409 | +CAN-2409 | 2yr biopsy+ 36.4% → 19.6% |
8 details
Phase 3, double-blind, placebo-controlled RCT, 2:1 randomisation, N=745 across 51 US and Puerto Rico centres. Median follow-up 50.3 mo.
Intermediate or high-risk localised prostate cancer, ECOG 0-2, planned for EBRT. Stratified by risk category and ADT use. 79% White, 16% Black.
EBRT 78 Gy/2 Gy, or hypofractionated 60 Gy/3 Gy or 70 Gy/2.5 Gy. ADT optional. No dose-escalation or brachytherapy boost mandated.
Three intraprostatic aglatimagene injections (5×10^11 viral particles) plus valacyclovir prodrug, versus placebo plus valacyclovir.
Primary: disease-free survival (recurrence or death, ITT). Secondary/exploratory: OS, PCSM, 2-year post-RT biopsy pathologic response.
Primary met: DFS favoured aglatimagene; OS and PCSM immature, not significantly different. Arm-by-endpoint values in the results figure.
| Event (G3+) | Aglatimagene | Placebo |
|---|---|---|
| Any TEAE | 8% (40/479) | 7% (17/232) |
| Acute kidney injury | 2% (9/479) | 2% (4/232) |
| Serious AEs | 6% (28/479) | 7% (17/232) |
Grade 3+ TEAEs 8% vs 7%; most common acute kidney injury (2% both arms). Serious AEs 6% vs 7%. No treatment-related deaths.
Discussant benchmarked the biopsy-positivity gain against ADT (RTOG 9408), brachytherapy boost (ASCENDE-RT), and SIB (FLAME) as established local-control intensifiers.
DFS is a composite surrogate; OS and PCSM immature. ADT optional, no boost mandated, confounding added value over modern intensification. Accrual (2012-2021) predates PSMA staging.
Positive phase 3 primary (DFS) but on a surrogate/composite; OS and PCSM immature (1 event/arm). Additive benefit over modern dose-intensification plus ADT unproven.
In intermediate or high-risk localised prostate cancer planned for definitive EBRT, this informs whether an added intraprostatic biologic could improve local control; it does not extend to post-prostatectomy, salvage, or metastatic settings.
- Does the local-control gain add over modern dose-escalation and ADT?
- Do DFS and pCR gains translate to overall or cancer-specific survival?
- Optimal ADT and RT-intensification pairing with intraprostatic CAN-2409
📚 Sources · 🐦 1 tweet · 📄 1 paper
🗣️Prostate Oral Abstract #ASCO25
— Michael Serzan, MD (@MikeSerzanMD) June 3, 2025
👉Dr @angela_jia_ discusses "Better Treatments, Better Selection: Improving Patient Outcomes in Localized Prostate Cancer"
🔑 KEY TAKE AWAYS
- #CAN2409 improves DFS and 2yr PathCR however PCSM and OS remain immature.
❓How to integrate with… pic.twitter.com/WamsneYBI1
Abstract
Genomic Classifier + NCCN Risk Stratification (Abstract 5000)
ForNCCN high-risk/very-high-risk localized prostate cancer
TL;DR22-gene GC independently prognostic (MFS/DM/OS, p<0.001); combined NCCN+GC score reclassifies ~¼ of high-risk pts to gate AAP intensification on an RT+ADT backbone.
~¼ of NCCN ≥HR pts are clinical/GC-discordant, so the 22-gene GC reclassifies who reaches CT-VHR (≥3 pts) and has AAP added onto the fixed RT+ADT backbone. The intensification it triggers carries STAMPEDE M0 magnitude (MFS HR 0.53, OS HR 0.60). It sharpens the intensification decision, not RT dose or target.

+2 more figures

| Endpoint | HR (add AAP) | 95% CI | p |
|---|---|---|---|
| MFS | 0.53 | 0.44-0.64 | <0.0001 |
| OS | 0.60 | 0.48-0.73 | <0.0001 |

7 details
Retrospective validation of the 22-gene GC (Decipher) layered on NCCN clinical risk in NCCN ≥ high-risk localized prostate (NRG cohort), externally benchmarked to STAMPEDE M0 curves (Attard, Lancet 2022). Not a prospective RCT.
NCCN high-risk and very-high-risk localized prostate cancer, all planned for definitive RT+ADT.
CT-HR (≤2 pts) → RT+ADT; CT-VHR (≥3 pts) → RT+ADT+AAP (abiraterone acetate + prednisone) intensification.
GC is independently prognostic for MFS, DM, and OS over clinical variables (multivariable, p<0.001). Roughly one-quarter of NCCN ≥HR pts are clinical/GC-discordant, reclassifying risk band and the intensification call.
| Component | Category | Points |
|---|---|---|
| NCCN clinical | High-risk | +1 |
| NCCN clinical | Very-high-risk | +2 |
| GC (Decipher) | < 0.6 | 0 |
| GC (Decipher) | 0.6-0.85 | +1 |
| GC (Decipher) | > 0.85 | +2 |
AAP intensification magnitude is borrowed from STAMPEDE M0 (Attard, Lancet 2022), not generated here; GC prognostic value aligns with prior Decipher/NRG validation.
Prognostic, not predictive: no randomized biomarker×treatment interaction showing CT-VHR pts gain more from AAP. Intensification benefit imported from an external trial's average effect.
Retrospective GC prognostic validation, not a randomized predictive-biomarker trial; consistent with prior Decipher/NRG data. Intensification benefit borrowed from STAMPEDE, not shown to be GC-predictive.
In NCCN high-risk/very-high-risk localized prostate planned for definitive RT+ADT, this supports GC-informed CT-VHR (≥3 pts) selection for AAP intensification; it does not extend to intermediate-/low-risk disease or change RT dose or target.
- Does GC-guided AAP intensification improve outcomes prospectively?
- Is GC predictive of differential AAP benefit, not just prognostic?
- Optimal AAP intensification threshold in clinical/GC-discordant pts
📚 Sources · 🐦 2 tweets
#ASCO26 Dr. Patel presented a clinically practical framework integrating NCCN clinical risk + a 22-gene genomic classifier to guide treatment intensification in high-risk localized prostate cancer.
— Julian Chavarriaga (@chavarriagaj) May 30, 2026
Key findings:
🔹 The genomic classifier independently improved prognostic… pic.twitter.com/fRcdTmfBec
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 Abstract 5000 | High-risk prostate cancer
Clinico-transcriptomic risk stratification to guide abiraterone intensification
Presented by Krishnan R. Patel, MD, MHS@Krishnan_Patel@OncoAlert@ASCO
In high-risk localized prostate cancer,… pic.twitter.com/pZSCiTyGB8
ARACOG (AFT-47)
ForAdvanced prostate cancer (mHSPC/mCRPC/nmCRPC) starting an ARSI
TL;DRMCCD -36.1 (enza) vs -15.8 (daro), P=0.009 at 24 wk: enzalutamide worse for cognition; randomized open-label phase 2, N=111 advanced prostate.
In advanced prostate cancer pts where cognitive tolerability drives ARSI selection, this randomized head-to-head supports darolutamide over enzalutamide for cognitive sparing; it does not address efficacy or compare against apalutamide or abiraterone.

| Arm (N) | Max-changed domain | Median % change | P |
|---|---|---|---|
| Darolutamide (48) | PALFAM (visual mem/exec) | -15.8 | 0.009 |
| Enzalutamide (47) | SWM (working mem/exec) | -36.1 | n/a |
+1 more figure

7 details 2 trials watching
Randomized open-label phase 2, N=111, darolutamide vs enzalutamide, stratified by age (<65, 65-80, >80). US academic centers only; enrolled 8/2021 to 3/2025, crossover permitted.
Advanced prostate cancer across mHSPC, mCRPC, and nmCRPC. Required acceptable enzalutamide co-pay; predominantly White, with most non-White pts randomized to enzalutamide.
Darolutamide provided by the study vs enzalutamide through standard of care, an asymmetry that could bias crossover and adherence.
Primary: between-arm % change from baseline to 24 wk in Maximally Changed Cognitive Domain (MCCD), from 5 remotely delivered CANTAB tests. Crossovers scored at crossover in their randomized arm.
MCCD median change -36.1 (enza, N=47) vs -15.8 (daro, N=48), P=0.009: greater cognitive decline on enzalutamide.
First randomized head-to-head of cognition for these two ARSIs; direction fits darolutamide's minimal blood-brain-barrier penetration vs enzalutamide's CNS exposure.
Open-label with a functional endpoint; enzalutamide via standard of care may have altered crossover. CANTAB is a research tool, not a clinical diagnostic; small N and race-by-arm imbalance limit inference.
Randomized head-to-head met its prespecified cognitive endpoint; aligns with darolutamide's known low CNS penetration. Phase 2, open-label, small N keep it below practice-changing.
- Does the cognitive advantage translate to functional outcomes or efficacy? n=102 · primary completion 2026-04 · tracks functional status + cognition on ARPIs
- Darolutamide vs apalutamide or abiraterone on cognition? n=102 · primary completion 2026-04 · cognitive outcomes across daro/apa/abi ARPIs
- Durability of the cognitive difference beyond 24 weeks
📚 Sources · 🐦 2 tweets
ARACOG (AFT-47) met its primary endpoint: enzalutamide caused significantly greater cognitive decline than darolutamide at 24 weeks in advanced prostate cancer.
— Katy Beckermann (@katy_beckermann) May 30, 2026
Randomized open-label phase 2, 111 pts (mHSPC, mCRPC, nmCRPC), DAR vs ENZ.
Cognition was measured with CANTAB, a… pic.twitter.com/kj4vfGRVyp
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 Abstract 5005 | ARACOG / AFT-47
Cognitive effects of darolutamide vs enzalutamide
Presented by Alicia K. Morgans, MD, MPH, FASCO@CaPsurvivorship @OncoAlert@ASCO
In prostate cancer, we often discuss AR pathway inhibitors through the lens… pic.twitter.com/vpZr1w6kc6
TALAPRO-3
ForHRR-deficient metastatic prostate cancer
HR 0.48
95% CI 0.36-0.65, P<0.001; 3yr rPFS 77% vs 56% (ITT)
TL;DR3yr rPFS 77% vs 56%, HR 0.48 (0.36-0.65), adding talazoparib to enzalutamide/ADT in HRR-deficient metastatic prostate cancer.
In HRR-deficient metastatic prostate cancer, this supports intensifying enzalutamide/ADT with talazoparib, benefit steepest in the BRCA subgroup; it does not extend to HRR-intact disease.

| Population | HR (95% CI) | Median rPFS, mo |
|---|---|---|
| ITT | 0.48 (0.36-0.65) | NC vs 45.8 |
| BRCA | 0.37 (0.22-0.61) | NC vs 35.1 |
| Non-BRCA | 0.57 (0.39-0.82) | NC vs NC |
6 details 2 trials watching
Randomized, placebo-controlled trial: talazoparib+enzalutamide vs placebo+enzalutamide, 300 vs 299 pts. Published NEJM May 30, 2026.
HRR-deficient metastatic prostate cancer, enzalutamide/ADT backbone both arms. Prespecified BRCA (104/103) and non-BRCA HRR (196/196) strata.
Talazoparib (PARP inhibitor) added to enzalutamide plus ADT; control substituted placebo for talazoparib on the same ARSI backbone.
Primary: imaging-based (radiographic) PFS. OS and other secondaries not reported in source.
ITT 3yr rPFS 77% vs 56%, P<0.001; per-population HRs and medians in the figure. Benefit concentrated in the BRCA subgroup.
Extends PARP+ARSI combinations (TALAPRO-2, PROpel, MAGNITUDE) that established the class in HRR-altered mCRPC toward the enzalutamide/ADT-backbone metastatic setting.
Primary endpoint is rPFS, a surrogate; OS not reported in source. Non-BRCA benefit is modest, so the HRR-wide result leans on BRCA. Talazoparib medians not reached, so follow-up is immature.
Randomized phase 3, rPFS primary hit (HR 0.48); but rPFS is a surrogate and OS not reported. Aligns with PARP+ARSI direction (TALAPRO-2, PROpel, MAGNITUDE).
- Overall survival benefit, given rPFS is the surrogate primary endpoint n=1054 · primary completion 2022-10 · mature phase 3, same combo vs enza, mCRPC
- Whether non-BRCA HRR alterations derive benefit comparable to BRCA recruiting A Study of Talazoparib With or Without Enzalutamide in People With Prostate Cancer Who Have Previously Received Abiraterone Acetate Phase 2n=126 · primary completion 2029-03 · talazoparib in broad HRR-mutant mCRPC
📚 Sources · 🐦 1 tweet
JUST In: TALAPRO-3 published in @NEJM
— Toni Choueiri, MD (@DrChoueiri) May 30, 2026
Adding #talazoparib to enzalutamide/ADT
=>3-year rPFS: 77% vs 56% in HRR-deficient metastatic prostate cancer !
Looking forward to full presentation by @neerajaiims who keeps changing SOC, one trial at a time. @ASCO #ASCO26 @OncoAlert pic.twitter.com/nXiPk4DIXg
PREPEC
ForSkin/nipple-sparing mastectomy, implant reconstruction, prevention/therapeutic
Δ4.8 pts (79.2 vs 74.3)
95% CI 1.0-8.7, p=0.01; 24mo, pre- vs sub-pectoral
TL;DRPre-pectoral implant improved 2yr chest well-being +4.8 pts (BREAST-Q, p=0.01) vs sub-pectoral, but more unplanned implant loss (21% vs 15%).
In pts undergoing skin- or nipple-sparing mastectomy (therapeutic or risk-reducing) who choose implant reconstruction, this supports pre-pectoral placement for better 2yr patient-reported chest well-being, weighed against numerically higher unplanned implant loss (21% vs 15%).

| Endpoint (24mo) | Pre-pectoral (N=191) | Sub-pectoral (N=189) | Difference |
|---|---|---|---|
| Physical well-being, chest (BREAST-Q) | 79.2 (75.5-82.8) | 74.3 (70.7-78.0) | 4.8 (1.0-8.7), p=0.01 |
+1 more figure

| Unplanned implant loss/replacement (24mo) | Pre-pectoral | Sub-pectoral | Adj. difference (95% CI) |
|---|---|---|---|
| Crude % (n/N) | 21.1% (41/194) | 14.5% (27/186) | 5.7% (-2.4 to 13.8) |
8 details 3 trials watching
International randomized phase 3 trial (OPBC-02): pre- vs sub-pectoral implant reconstruction after skin- or nipple-sparing mastectomy. Open-label; patient-reported primary endpoint analyzed by multiple imputation and linear mixed models.
Women undergoing skin- or nipple-sparing mastectomy for cancer treatment or risk reduction, opting for implant reconstruction. Primary QoL analysis N=191 pre- vs 189 sub-pectoral.
Primary: long-term patient-reported physical well-being (chest), BREAST-Q, at 24 months. Main secondary safety: unplanned loss or replacement of expander/implant.
BREAST-Q chest well-being 79.2 vs 74.3 at 24mo, difference 4.8 (95% CI 1.0-8.7, p=0.01), favoring pre-pectoral. Longitudinal completion 83-95%.
Point estimate showed more implant loss with pre-pectoral (21.1% vs 14.5%), failing the trial's non-inferiority safety hypothesis; the adjusted-difference 95% CI (-2.4 to 13.8) crosses zero.
Open-label with a patient-reported primary endpoint, so awareness of implant type could bias PROs. The 4.8-point gain is significant but modest, and the safety signal trended against pre-pectoral.
A major RCT in an area of genuine equipoise. It supports pre-pectoral for patient-reported chest well-being while flagging a higher implant-loss signal, so the choice reads as a real trade-off, not a clean win.
Randomized phase 3, primary endpoint met, but a modest patient-reported surrogate and an unmet non-inferiority safety endpoint keep it short of practice-changing.
- Durability of the QoL benefit and implant-loss gap beyond 24 months n=300 · primary completion 2024-12 · prepectoral vs subpectoral head-to-head, n=300n=88 · primary completion 2025-03 · prepectoral vs subpectoral breast satisfaction
- Do outcomes differ in patients receiving post-mastectomy radiation? n=104 · primary completion 2027-03 · prepectoral recon in adjuvant RT patients
- Which patients accept higher implant-loss risk for better chest well-being?
📚 Sources · 🐦 1 tweet
📌 Surgical de-escalation of implant-based breast reconstruction after mastectomy for breast cancer treatment or prevention: The international randomized phase I|I
— Elisabetta Bonzano MD, PhD (@to_be_elizabeth) May 30, 2026
PREPEC trial (ОРBC-02).
Presented by Walter Weber ✨#ASCO26 @OncoAlert #OncoAlertAF #BreastCancer pic.twitter.com/WE20JcBQG0
Wait or Treat? NCT05236946
ForAsymptomatic brain mets, EGFR/ALK-mutant metastatic NSCLC, on TKI + chemo
Sub-HR 0.35
95% CI 0.21-0.59, p<0.001; favors upfront RT
TL;DRUpfront cranial RT cut 2y intracranial progression (21.7% vs 50%, sub-HR 0.35) but no OS gain; survival numerically favored delayed (HR 1.45).
The primary endpoint actually favored upfront RT (2y intracranial progression 21.7% vs 50%, sub-HR 0.35), yet OS trended toward delayed (2y 48% vs 60%) with 6% radiation necrosis vs none. Better CNS control bought no survival and added toxicity, so upfront cranial RT can be safely deferred to intracranial progression.

| Endpoint | Upfront RT | Delayed RT |
|---|---|---|
| Events | 20 | 47 |
| 1-yr intracranial PD | 8.7% (2.9-14.5) | 25.7% (16.8-34.7) |
| 2-yr intracranial PD | 21.7% (12.6-30.8) | 50% (39.2-60.9) |
| Sub-HR (95% CI) | 0.35 (0.21-0.59), p<0.001 | ref |
8 details 4 trials watching
Phase 3 open-label RCT, 1:1, N=208 (105 upfront cranial RT vs 103 delayed) at a single center (Tata Memorial). Median follow-up 30.6 mo; stratified by GPA and synchronous vs metachronous BM.
Metastatic EGFR- or ALK-mutant NSCLC with radiologically measurable, completely asymptomatic brain metastases, ECOG 0-2. Both arms received TKI + chemotherapy.
Delayed arm held cranial RT until intracranial progression or patient request, with MRI brain q3mo for year 1 then q6mo. RT dose, fractionation, and technique (SRS vs WBRT) not reported in source.
Primary: intracranial PFS. Secondary: OS, PFS, toxicity, ORR, neurocognition, PROM.
Primary endpoint met for intracranial control but did not translate to survival; the OS trend and radiation-necrosis signal both favored deferral. See the intracranial-progression figure and survival table for effect sizes.
First randomized evidence on RT timing in this population. Consistent with the CNS-active TKI era (osimertinib, alectinib, lorlatinib), where strong systemic intracranial control supports deferring RT.
Open-label and single-institution. Powered for intracranial PFS, not OS, so the survival and necrosis signals favoring deferral are secondary. RT technique not reported.
Randomized phase 3, primary intracranial-PFS endpoint met, but no OS benefit and less necrosis with deferral; backs the emerging TKI-first, defer-RT approach in oncogene-driven NSCLC.
In asymptomatic brain metastases from EGFR/ALK-mutant metastatic NSCLC on TKI plus chemo, this supports deferring cranial RT until intracranial progression; it does not extend to symptomatic brain mets or oncogene-negative NSCLC.
- Neurocognition and PRO outcomes by RT timing (not reported in source)
- Does RT technique (SRS vs WBRT) change the deferral tradeoff? n=115 · primary completion 2026-07 · randomizes SRT vs hippocampal-sparing WBRT
- Durability of TKI-first intracranial control beyond 2 years n=162 · primary completion 2024-12 · osi alone vs early SRS, asymptomatic BMactive Study of Osimertinib + SRS vs Osimertinib Alone for Brain Metastases in EGFR Positive Patients With NSCLC Phase 2n=40 · primary completion 2025-04 · osimertinib-alone arm tests TKI-first controlrecruiting Early or Delayed Intervention of Brain Radiotherapy Combined With Almonertinib in EGFR Mutated NSCLC With Brain Metastases Phase 3n=232 · primary completion 2028-12 · randomizes early vs delayed RT on EGFR-TKI
📚 Sources · 🐦 3 tweets
#ASCO26 | Wait or Treat? Brain RT in EGFR/ALK+ NSCLC
— OncLive.com (@OncLive) May 29, 2026
Presented by Dr Anil Ramakant Tibdewal.
A landmark Phase III randomized trial from @TataMemorial addressed a long-standing question: should asymptomatic brain metastases in oncogene-driven NSCLC receive upfront cranial RT or… pic.twitter.com/lRy9CfyQ8r
Should asymptomatic brain mets await systemic response in front line within EGFR/ALK context? I think yes. Despite reducing icPD, delayed brain RT OS looked better and radiation necrosis didn’t occur vs 6% #ASCO26 pic.twitter.com/O6d7GrvtU4
— Dr Riyaz Shah (@DrRiyazShah) May 29, 2026
No improvement in survival with up front radiation. OS favored delayed radiation with 2y OS 48% with early radiation vs 60% in late (OS HR 1.45). Also, radiation necrosis less common and less severe in delayed arm. Each case unique but delayed approach appealing #ASCO26 pic.twitter.com/wIhjqxhSaq
— Stephen V Liu, MD (@StephenVLiu) May 29, 2026
SENOMAC NCT02240472
ForcN0 T1-T3 breast cancer, 1-2 sentinel-node macrometastases
HR 0.89
95% CI 0.66-1.19, NI met (margin 1.44); primary OS not yet reported
TL;DR5-yr RFS 89.7% vs 88.7%, HR 0.89 (0.66-1.19): omitting completion ALND noninferior, with nodal RT given in ~90% of both arms.
Nodal RT with nodal target volumes reached ~90% in both arms (89.9% vs 88.4%), so SENOMAC validates dropping completion ALND within regional nodal irradiation, not omitting axillary treatment. For the RT reader it positions nodal RT as the axillary treatment when SNB shows 1-2 macromets; it does not test omitting both surgery and RT.
8 details 4 trials watching
Phase 3 noninferiority RCT, 1:1, N=2766 enrolled (2540 per-protocol), 67 sites across 5 countries; median follow-up 46.8 mo. Reports the prespecified secondary RFS; primary OS not yet reported.
cN0 T1-T3 breast cancer with 1-2 sentinel-node macrometastases (>2mm). Extends eligibility beyond Z0011 to mastectomy, T3, extracapsular extension, and men.
Nodal RT including nodal target volumes reached 89.9% (SNB-only) and 88.4% (cALND). ALND omission was therefore tested within regional nodal irradiation, not as omission of axillary treatment.
Primary: overall survival (not reported in source). This analysis: prespecified secondary recurrence-free survival, per-protocol and modified ITT.
Noninferiority met: the upper confidence bound stayed below the prespecified 1.44 margin (P<0.001) across 191 recurrence-or-death events.
| Endpoint | SNB only | cALND |
|---|---|---|
| 5-yr RFS | 89.7% (87.5-91.9) | 88.7% (86.3-91.1) |
| HR recurrence/death | 0.89 (0.66-1.19) | ref |
Consistent with Z0011 (breast-conserving + whole-breast RT) and AMAROS (axillary RT replacing ALND), both null for ALND benefit at 10 yr. SENOMAC adds the macromet-only, mastectomy/T3/ECE/male groups in a larger cohort.
This is the secondary RFS endpoint, not the OS primary, at a 46.8-mo median follow-up short for ER+ biology. The HR 1.44 noninferiority margin is generous, and ~90% nodal RT confounds attribution to surgical omission alone.
Randomised phase 3 noninferiority; prespecified secondary RFS met, extends Z0011/AMAROS de-escalation to mastectomy/T3/ECE/men. Primary OS not yet reported.
In cN0 breast cancer with 1-2 sentinel-node macrometastases who receive regional nodal RT, this supports omitting completion ALND, including mastectomy, T3, extracapsular extension, and men; it does not extend to patients treated without nodal radiotherapy.
- Overall survival (primary endpoint) result still pending
- Can nodal RT be omitted alongside ALND in this population? recruiting Evaluating Omitting of Internal Mammary Irradiation Among Early Stage Intermediate Risk (N1) Breast Cancer Phase NAn=214 · primary completion 2025-10 · randomized omit internal mammary RT in N1active Postmastecomy Internal Mammary Nodal Irradiation for High-risk Breast Cancer Patients Phase 3n=2400 · primary completion 2025-11 · phase 3 IMN RT vs no IMN RT, DFS endpointrecruiting The T-REX Trial: Tailored Regional External Beam Radiotherapy in Clinically Node-negative Breast Cancer Patients With 1-2 Sentinel Node Macrometastases. Phase NAn=1350 · primary completion 2028-12 · omit regional RT, 1-2 SN macromets, ER+/HER2-recruiting RecurIndex Guided Avoidance of Regional Nodal Irradiation for Node Positive Breast Cancer Phase NAn=540 · primary completion 2029-08 · RecurIndex-guided RNI avoidance in N1
- Durability beyond 5 years in ER+ disease
📚 Sources · 📄 1 paper
SWOG/NRG S1914 NCT04214262
ForEarly-stage inoperable/surgery-declined NSCLC (T1-3N0M0 ≤7cm), ≥1 risk factor
HR 1.15
95% CI 0.65-2.01, p=0.63; did not meet primary
TL;DROS HR 1.15 (0.65-2.01), p=0.63: adding atezolizumab to SBRT did not improve survival in early-stage inoperable NSCLC; futility-stopped, excess toxicity.
Local control got worse with IO, not better: local failures 13% vs 7% adding atezolizumab, alongside null OS/PFS and a former/never-smoker harm signal (OS HR 2.50). SBRT alone stays standard for inoperable early-stage NSCLC, closing the add-IO-to-SBRT question negatively.
6 details
Phase 3 open-label RCT, 1:1, SWOG/NRG; N=403 eligible (201 S / 202 AS). Stopped at first interim for futility on OS and PFS. Median follow-up 12 mo (0.03-49).
T1-3N0M0 NSCLC ≤7cm, medically inoperable or declined surgery, ≥1 recurrence risk factor (diameter ≥2cm, SUV ≥6.2, moderate/poor/undifferentiated). Median age 73, median tumor 2.3cm, 89% ECOG 0-1.
SBRT both arms (SoC backbone): 3-8 fractions, BED ≥100 Gy. Stratified by central vs peripheral, <4 vs ≥4cm, PS 0-1 vs 2.
Atezolizumab 1200mg IV Q3wk ×8 (neoadjuvant, concurrent, adjuvant); SBRT initiated at cycle 3.
Primary: overall survival. Secondary: PFS, failure patterns, toxicity, QoL. 1-sided stratified log-rank at 2.5%.
G≥3 AEs 12% AS (21 G3, 1 G4, 1 G5 respiratory-failure death) vs 2% S. Excess toxicity with no efficacy gain.
Prior randomized phase 2 (**PMID 37478883, I-SABR, nivolumab+SBRT) suggested benefit adding IO; S1914 with atezolizumab does not confirm** and shows harm signals.
Open-label; stopped early at interim (median f/u 12mo, only 49 deaths). Former/never-smoker harm is an exploratory subgroup; central review of local recurrence ongoing.
| Endpoint | S | AS | HR (95% CI), p |
|---|---|---|---|
| 2yr OS | 82% | 80% | 1.15 (0.65-2.01), p=0.63 |
| 2yr PFS | 71% | 60% | 1.35 (0.89-2.06), p=0.16 |
| Failure | S | AS |
|---|---|---|
| Local | 7% | 13% |
| Regional | 2% | 3% |
| Distant | 4% | 5% |
| Endpoint (never/former smokers) | HR (95% CI), p |
|---|---|
| OS | 2.50 (1.11-5.59), p=0.03 |
| PFS | 2.16 (1.15-4.04), p=0.01 |
Phase 3 stopped for futility; adding IO to SBRT gave no OS/PFS benefit and excess toxicity, reaffirming SBRT-alone SOC and not confirming the prior phase 2 signal.
In medically inoperable or surgery-declined early-stage (T1-3N0) NSCLC treated with definitive SBRT, this argues against adding atezolizumab, and does not extend to node-positive or locally advanced disease.
- Biomarker/PD-L1 subset that benefits from adding IO to SBRT
- Whether excess local failures with IO hold on central review
- Reconciling harm signal with prior phase 2 IO+SBRT benefit
📚 Sources · 📄 1 paper
Abstract
DBCG IMN2 NCT06549920
ForNode-positive breast cancer, incl. 1-3 positive nodes; no neoadjuvant therapy
HR 0.85
95% CI 0.76-0.94, p=0.0016; 15yr OS 65.0% vs 60.8%
TL;DR15yr OS 65.0% vs 60.8% with IMNI, adjusted HR 0.85 (0.76-0.94); benefit persists under modern systemic therapy and 3D RT.
The 1-3 positive-node subgroup is the RT read: IMNI benefit held at the lowest nodal burden, no subgroup found for omission, moving elective IMN coverage where guidelines diverge. Reassuring on toxicity too: 15yr ischemic/valvular cardiac death 0.2% (right/IMNI) vs 0.7% (left) under 3D planning.
8 details 4 trials watching
Prospective nationwide population-based cohort, N=4541, 6 RT centres, treated 2007-14. IMNI assigned by tumour laterality: right-sided → IMNI, left-sided → no IMNI. Median follow-up 13.7 yr.
Node-positive breast cancer, including the 1-3 positive-node low-burden group. Excluded prior malignancy, bilateral cancer, neoadjuvant systemic therapy, pre-RT recurrence, non-standard RT.
Modern systemic backbone: taxane chemotherapy, trastuzumab, aromatase inhibitors, the era hypothesized to shrink absolute IMNI gain.
3D-based RT. IMNI delivered to right-sided tumours only; laterality allocation balances cardiac dose. Dose/fractionation not reported in source.
Primary: overall survival. Secondary: breast cancer mortality, distant metastasis.
IMNI improved all three endpoints (see table). Absolute 15yr OS gain 4.2% (65.0% vs 60.8%).
| Endpoint | Adjusted HR (95% CI) | p |
|---|---|---|
| Overall survival | 0.85 (0.76-0.94) | 0.0016 |
| Breast cancer mortality | 0.84 (0.74-0.95) | 0.0077 |
| Distant metastasis | 0.87 (0.78-0.98) | 0.026 |
| Study | Design | Signal |
|---|---|---|
| DBCG IMN1 (2003-07) | prospective cohort, n=3089 | +4.7% abs OS, f/u 14.8yr |
| EBCTCG meta-analysis | n=12,167 | +3% abs 15yr survival, regional node RT |
| Korean KROG 06-08 | 3D-RT, modern systemic | negative for IMNI |
Confirms DBCG IMN1 (+4.7% abs OS at 14.8 yr) and the EBCTCG meta-analysis (+3% abs 15yr survival, regional node RT); contradicts the negative Korean KROG 06-08 in the modern-therapy era.
Non-randomized: IMNI assigned by tumour laterality rather than randomization, so residual confounding is possible despite balanced baseline characteristics.
Large prospective laterality-allocated cohort, not randomized; confirms IMN1 + EBCTCG that IMNI benefit persists with modern systemic therapy. Non-random design caps it below practice-changing.
In node-positive breast cancer treated with upfront surgery then modern systemic therapy, especially 1-3 positive nodes, this supports including internal mammary nodes in the RT target; it does not extend to neoadjuvant-treated pts, who were excluded.
- Randomized confirmation of IMNI benefit in 1-3 node patients active Postmastecomy Internal Mammary Nodal Irradiation for High-risk Breast Cancer Patients Phase 3n=2400 · primary completion 2025-11 · phase 3 randomizing IMNI vs none, DFS endpoint
- IMNI value in neoadjuvant-treated patients (excluded here) recruiting Internal Mammary Lymph Nodes Irradiation in High-risk Breast Cancer After Neoadjuvant Chemotherapy Phase 3n=722 · primary completion 2032-07 · phase 3 IMNI vs none in post-NACT ypN+ pts
- IMNI cardiac safety with modern breath-hold or proton planning recruiting Robustness Evaluation of Deep Inspiration Breath-Hold (DIBH) Plans in Internal Mammary Irradiationn=25 · primary completion 2026-12 · DIBH plan OAR dose in IMN irradiationn=750 · primary completion 2027-12 · IMPT vs IMRT toxicity, heart among key OARs
📚 Sources · 📄 1 paper
Multicenter TMT Bladder Preservation Analysis (n=369)
ForMuscle-invasive bladder, cT2-T4aN0M0, median age 76
TL;DRCLR 63.7% in 369 MIBC pts on definitive TMT; 5-FU-based CRT and better image guidance predicted higher complete local response.
The two modifiable levers here are RT delivery and chemo backbone, both in the radonc's hands: 5-FU-based CRT predicted higher CLR (OR 4.9) and weekly portal imaging lower CLR (OR 0.35, p<0.001), favoring daily volumetric IGRT. Technique, not just patient selection, moved local control.
8 details 4 trials watching
Multicenter retrospective cohort, Spain 2010-2022, N=369 treated with definitive TMT (maximal TURBT + concurrent chemoRT). Multivariable logistic regression for predictors of complete local response.
cT2-T4aN0M0 muscle-invasive bladder. Median age 76, 85.1% male. Node-positive and metastatic disease excluded by staging.
Image-guidance quality tracked with local control: weekly portal imaging predicted lower CLR (OR 0.35, p<0.001), favoring daily volumetric IGRT; VMAT showed a non-significant favorable trend. RT dose/fractionation not reported in source.
Concurrent chemoradiotherapy. 5-FU-based CRT predicted higher CLR (OR 4.9, 95% CI 1.1-22.1, p=0.038).
Primary: complete local response (CLR). Secondary: OS, CSS, recurrence patterns, salvage cystectomy.
CLR 63.7%. Disease progression 28.8% (local 10.1%, systemic 10.7%, combined 8.7%). Salvage cystectomy 9.7%.
Retrospective, non-randomised; CLR predictors exploratory and confounded by treatment era. No head-to-head vs radical cystectomy; RT technique detail and CLR-survival effect sizes absent from source.
Retrospective real-world European cohort; no randomised TMT-vs-cystectomy comparator. Reinforces guideline-recognized bladder preservation; predictor findings exploratory.
In cT2-T4aN0M0 MIBC pts already committed to bladder-preserving TMT, this favors daily volumetric IGRT and 5-FU-based chemoRT for local control; it does not inform the upstream TMT-versus-radical-cystectomy choice or node-positive/metastatic disease.
- Optimal concurrent chemoradiotherapy regimen for bladder preservation active Treating Muscle-invasive Bladder Cancer With A Non-surgical Method Consisting of Anti-PD-1 Therapy and Chemoradiation Phase 2n=71 · primary completion 2025-12 · adds toripalimab to concurrent chemoRTrecruiting Enfortumab Vedotin in Combination With Pembrolizumab vs. Concurrent Chemoradiotherapy (cCRT) in People With Muscle Invasive Bladder Cancer (EV-309) Phase 3n=390 · primary completion 2030-03 · phase 3 EV+pembro vs concurrent chemoRT
- Whether daily volumetric IGRT improves local control vs weekly imaging n=345 · primary completion 2021-12 · adaptive tumour-focused vs whole-bladder RTnot yet Evaluation of the Clinical Utility of Online Adaptive Radiotherapy in Bladder Cancer (BLADAPT-GETUG V11) Phase NAn=120 · primary completion 2029-01 · randomised online-adaptive vs standard RT in TMT
- Randomised TMT vs radical cystectomy comparison
📚 Sources · 🐦 1 tweet
📢 Presentamos en #ESTRO26 nuestro análisis multicéntrico sobre preservación vesical en cáncer vesical músculo-invasivo tratado con TMT.
— URONCOR (@URONCOR) May 19, 2026
🔎 En 369 pacientes, la respuesta completa clínica se asoció a menor recurrencia local y mejor supervivencia!@fcounago #NicoFeltes pic.twitter.com/aQjjkcHGP4
TORPEdO
ForOropharyngeal SCC requiring bilateral-neck concurrent chemoradiotherapy
No between-arm difference
No effect size reported in source; assessed at 3/12/24mo post-RT
TL;DRUW-QoL physical composite similar IMPT vs IMRT at 3/12/24mo in OPSCC; no proton QoL-toxicity benefit (no effect size reported in source).
The proton premise, less QoL toxicity, didn't show: UW-QoL physical composite tracked identically IMPT vs IMRT from 6 weeks through 24 months, both arms at 70/56 Gy in 33fx. That undercuts routing OPSCC pts to protons for QoL benefit, though identical planning constraints and novel UK proton centres may have capped IMPT's achievable dosimetric edge.

+1 more figure

9 details 2 trials watching
Phase 3 multicentre RCT (CRUK/18/010), N=205 oropharyngeal SCC, 2:1 IMPT:IMRT, stratified by T-stage, N-stage, p16 status, and smoking history.
Oropharyngeal SCC requiring concurrent chemoradiotherapy with bilateral neck treatment. p16 status was a stratification factor, so both HPV-associated and HPV-independent disease are included.
70 Gy / 56 Gy in 33 fractions over 6.5 weeks, identical for both arms; IMPT vs IMRT is the only difference. Identical planning constraints applied across modalities.
Concurrent cisplatin 100 mg/m² on D1 and D22.
Co-primary PRO: UW-QoL physical composite at 12mo (saliva, taste, chewing, swallowing, appearance, speech). Co-primary clinician: CTCAE grade 3 weight loss (≥20% from baseline) or gastrostomy dependence at 12mo.
No between-arm difference in UW-QoL physical composite at 3/12/24mo, similar from 6 weeks post-CRT, with similar trajectories across multiple PRO questionnaires. No effect size reported in source.
Support for protons in OPSCC has rested on dosimetric and single-institution toxicity data; this randomised HR-QoL readout does not confirm a patient-reported advantage for IMPT.
Only the HR-QoL co-primary is presented; the clinician co-primary (weight loss/gastrostomy) and 5yr late-effects follow-up are unreported. No effect sizes or CIs given. Novel UK proton centres and identical constraints may cap IMPT's achievable edge.
Randomised co-primary QoL null (IMPT≈IMRT), consistent with IMRT-based CRT remaining standard. Only HR-QoL co-primary shown; clinician co-primary and 5yr late effects still maturing.
In oropharyngeal SCC planned for definitive cisplatin chemoradiotherapy, these HR-QoL data give no patient-reported reason to prefer IMPT over IMRT; they don't address the clinician co-primary (weight loss/gastrostomy) or unilateral-neck cases that could still differ.
- Does IMPT reduce 5-year late effects vs IMRT? recruiting Comparing an Investigational Scan (F-18 NaF PET/CT) to Standard of Care Imaging (F-18 FDG PET/CT) for Evaluating Vascular Complications in Patients Receiving Radiation Therapy for Head and Neck Cancer Phase Early 1n=20 · primary completion 2026-08 · candidate match
- Clinician co-primary (weight loss/gastrostomy at 12mo) result?
- Does IMPT advantage emerge only at high-experience proton centres? n=7 · primary completion 2024-11 · candidate match
📚 Sources · 🐦 2 tweets
Day FOUR of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 18, 2026
Health-related quality of life in the phase III trial of Toxicity Reduction using Proton Beam Therapy for Oropharyngeal Cancer (TORPEdO;CRUK/18/010) Presented by Matthew Tyler🇬🇧 #RadOnc ☢️
TORPEdO, a multicentre phase 3… pic.twitter.com/ZP6yK7RThL
TORPEdO. Misma planificación + constraints idénticas y centros UK noveles probablemente limitaron el potencial de #IMPT.
— Amadeo Wals (@AmadeoWals) May 18, 2026
Centros con alta experiencia se siguen viendo ventajas clínicas . La QA rigurosa del UK es una fortaleza, pero no maximiza la diferencia.#ESTRO26 #HNCSM https://t.co/rASp3QDIk1
Multinational HCC EBRT IPD Cohort
ForVery early / early-stage HCC (BCLC-0 to A), Child-Pugh A predominant
TL;DRMedian OS 6.8y BCLC-0 and 4.6y BCLC-A across 4,913 EBRT-treated HCC pts, comparable to resection/ablation.
The treatment-naive BCLC-0 arm is the RT-relevant cell: median OS not reached (95% CI 8.6 to NR), i.e. first-line EBRT in a truly untreated very-early cohort, not salvage after failed ablation. Ablative dose independently predicted lower mortality, so this moves the dose-selection and BCLC-algorithm-placement decisions.
9 details 3 trials watching
Systematic review (search date December 15, 2022) of EBRT series meeting prespecified HCC technical standards and reporting OS, followed by individual patient data solicitation from corresponding authors. Kaplan-Meier OS and RMST stratified by BCLC stage and treatment status; random-effects Cox for covariates.
N=4,913 EBRT-treated HCC pts across a multinational author network, median follow-up 5.0 years. Stratified as treatment-naive vs treatment-experienced; BCLC stage, tumor burden, performance status, and Child-Pugh class all captured at patient level.
EBRT delivered per each contributing series; the pooling filter was prespecified technical standards for HCC. Ablative dose was independently associated with reduced risk of death, but specific dose/fractionation schedules and the ablative-dose threshold are not reported in the source abstract.
Median OS 6.8 years for BCLC-0 and 4.6 years for BCLC-A; among treatment-naive pts not reached for BCLC-0 and 5.4 years for BCLC-A. On multivariable modeling, advanced BCLC stage, higher tumor burden, worse performance status, and Child-Pugh B/C raised mortality risk; ablative dose and more recent treatment year lowered it.
| Cohort | BCLC-0 | BCLC-A |
|---|---|---|
| All pts | 6.8 yrs (95% CI 5.7-8.7) | 4.6 yrs (95% CI 4.1-5.1) |
| Treatment-naive | NR (95% CI 8.6-NR) | 5.4 yrs (95% CI 4.5-6.7) |
The authors position these OS figures as comparable with resection, thermal ablation, and other ablative locoregional therapies. That comparison is across literatures, not within a trial, so the usual selection differences (lesion location, vascular proximity, comorbidity burden) between an EBRT-referred and a resection-eligible population remain unadjusted.
No comparator arm: the resection/ablation equivalence claim is a cross-study inference. IPD came only from authors who responded, and the technical-standard filter selects for expert centers, both biasing toward better outcomes. Year-of-treatment effect confounds technique era with staging and systemic-therapy improvements.
The practical argument here is algorithmic placement: BCLC has historically routed early HCC to resection, ablation, or transplant with EBRT absent, and this is the largest patient-level dataset assembled to contest that omission. The treatment-naive BCLC-0 result matters most, since it isolates first-line EBRT from salvage-after-ablation-failure use.
Large multinational prospective-collected IPD across many sites with stage-stratified analyses, but non-randomised and no head-to-head comparator; supports EBRT's guideline-listed role rather than establishing it.
In BCLC-0 or A HCC where ablation or resection is unattractive on lesion location or comorbidity, this supports offering ablative-dose EBRT as a first-line locoregional option rather than a salvage one; it does not speak to BCLC-B/C or Child-Pugh B-C pts, where OS was worse.
- Randomised EBRT vs thermal ablation in early HCC recruiting Stereotactic Radiosurgery Versus Radiofrequency Ablation for Primary Liver Cancer Phase 2n=130 · primary completion 2025-01 · randomised SBRT vs RFA, inoperable primary liver caactive Stereotactic Body Radiotherapy Versus Radiofrequency Ablation for Unresectable, Small (≤ 3 cm) HCC Phase NAn=178 · primary completion 2026-12 · randomised SBRT vs RFA in unresectable ≤3 cm HCCn=218 · primary completion 2032-04 · SABR vs percutaneous ablation, BCLC 0/A, 2y FFLP
- Ablative dose threshold defining the OS benefit
- Generalizability beyond expert EBRT centers
📚 Sources · 📄 1 paper
Abstract
EXTEND Trial
ForOligometastatic solid tumors, 1-5 mets, on standard systemic therapy
HR 0.54
95% CI 0.41-0.72, p<0.001 (per-protocol, all baskets)
TL;DRMDT+SOC improved PFS across all baskets, HR 0.54 (0.41-0.72), p<0.001; RT delivered 98% of MDT.
The RT-relevant read is that this is essentially an SBRT trial (98% of MDT was radiotherapy) layered on top of continued systemic therapy, so the PFS gain is attributable to local ablation, not a systemic switch. The prostate-excluded HR 0.60 (0.40-0.89) is what matters for referrals outside prostate. Dose and fractionation are not in the source abstract, which gates transfer to practice.
Also covered May 17
9 details 5 trials watching
Multicenter randomized phase II basket trial, accrual 2018 to 2023. Six baskets (breast, pancreas, kidney, two prostate, "Other") each with basket-specific stratification and powering. Median follow-up 53 months.
Patients with 1-5 metastases from solid tumors, randomized to MDT+SOC vs SOC systemic therapy alone. Screened 521, randomized 350, 334 analyzed per protocol (MDT+SOC n=166; SOC n=168).
Radiotherapy was the MDT for 98% of metastases (370/379), so this reads as an ablative RT trial in all but name. Dose, fractionation, and technique are not reported in the source abstract.
Primary: PFS, pre-specified in the per-protocol set within each basket, across all baskets, and across all baskets excluding prostate. Exploratory: ctDNA and immune profiling.
Overall PFS HR 0.54 (0.41-0.72), p<0.001; excluding prostate baskets HR 0.60 (0.40-0.89). Basket-level superiority in pancreas, prostate, and "Other"; breast and kidney inconclusive. Per-basket effect sizes not reported in source.
Detectable ctDNA at enrollment tracked with shorter PFS and survival; 3-month ctDNA clearance tracked with improved survival, raising the option of a ctDNA-refined oligometastatic definition. Systemic immune activation after MDT was most pronounced in the baskets that showed PFS superiority, offered as a candidate mechanism.
Per-protocol, not ITT, primary analysis with 16 of 350 randomized patients excluded. Phase II with six baskets tested, so histology-specific claims are hypothesis-generating; no OS result reported in source.
Randomized phase II, primary PFS endpoint hit with 53mo f/u, but per-protocol analysis and basket design; histology signals explicitly framed as hypothesis-generating for phase III.
In pts with 1-5 metastases from pancreas or prostate primaries already on standard systemic therapy, this supports adding ablative MDT rather than systemic therapy alone; the breast and kidney baskets were inconclusive and do not carry the same read.
- Does MDT-driven PFS gain translate to overall survival recruiting Veterans Affairs Seamless Phase II/III Randomized Trial of STAndard Systemic theRapy With or Without PET-directed Local Therapy for Oligometastatic pRosTate Cancer Phase 2/3n=464 · primary completion 2026-09 · phase 2/3 SST +/- PET-directed local therapy, CRPC-FSn=873 · primary completion 2027-04 · phase 3 MDT +/- ADT/ARTA, n=873, PMFS endpointn=1200 · primary completion 2030-12 · n=1200 prospective LAT cohort, any-histology OMD
- Can ctDNA refine which oligometastatic pts benefit from MDT n=60 · primary completion 2027-12 · SABR cohort with ctDNA dynamics as biomarkerrecruiting Phase II Non-Randomized Study Evaluating POSLUMA-PSMA PET Response After Oligo- Metastatic/Progressive-directed Treatment With Radiotherapy (PROMPT-R) Phase 2n=50 · primary completion 2028-05 · ctDNA change after ablative RT vs PSMA-PET response
- Why were breast and kidney baskets inconclusive
📚 Sources · 📄 1 paper
Abstract
NRG/RTOG 1005 NCT01349322
ForHigh-risk early breast cancer post-lumpectomy, receiving WBI plus cavity boost
HR 1.31
90% CI 0.84-2.04, P=.037; NI margin 2.12
TL;DR7-yr IBR 2.6% vs 2.2%, HR 1.31 (90% CI 0.84-2.04): concurrent boost noninferior to sequential, cutting WBI+boost to 15 fractions.
The transferable parameter is the boost itself: 8 Gy in 15F at 0.53 Gy per day, a lower cavity total than 12 Gy/6F sequential, with 7-yr IBR 2.6% vs 2.2%. Blinded photo cosmesis at 3y numerically favored concurrent (72.0% vs 64.2%, p=0.11). This moves boost technique, not whether to boost.
9 details 4 trials watching
Randomized, unblinded, phase 3 noninferiority trial across 278 sites in North America and 6 other countries. 2,354 randomized May 2011 to June 2014, 2,255 eligible for analysis. Median follow-up 7.3 years.
Higher risk of IBR after lumpectomy and axillary surgery. Median age 55 (IQR 47-64), 35.6% under 50; 96.8% invasive, 52.7% grade 3, 29.6% ER-negative, 16.3% node-positive, 16.7% LVI, 16.7% close (<2 mm) or focally positive margins. 61.8% received chemotherapy.
Concurrent arm: WBI 40 Gy/15F with concurrent boost 8 Gy/15F at 0.53 Gy per day. Sequential arm: WBI 50 Gy/25F (52.4%) or 42.7 Gy/16F (47.6%), then 12 Gy/6F (84.9%) or 14 Gy/7F. 3DCRT in 59%, photons in 73.8%; QART scored 92.8% of contours and 91.9% of dose plans per protocol or acceptable variation.
Primary: IBR as first recurrence, noninferiority defined as an HR upper 90% CI limit below 2.12. Secondary: DFS, OS, adverse events, and cosmesis (BCTOS, physician Global Cosmesis Score, blinded central digital photo review).
56 IBR events, 24 sequential and 32 concurrent. Noninferiority held on cause-specific hazards, Fine-Gray (HR 1.31, 90% CI 0.84-2.03), and against each sequential WBI fractionation separately; the triggered superiority test was not significant. 7-yr regional nodal recurrence 1.2% (95% CI 0.8-1.7) with no difference by arm, and no differences in DFS, DDFS, or OS.
| Endpoint | Sequential (n=1,118) | Concurrent (n=1,137) |
|---|---|---|
| 5-yr IBR | 2.1% | 1.9% |
| 7-yr IBR | 2.2% (90% CI 1.5-3.0) | 2.6% (90% CI 1.9-3.5) |
| IBR HR (90% CI) | reference | 1.31 (0.84-2.04), P=.037 |
Toxicity above grade 2 was uncommon, with no significant difference in grade 3-4 events (p=0.81); radiation dermatitis, fatigue, and breast pain were most prevalent. 3-yr excellent/good cosmesis by physician rating 85.9% vs 82.4% (p=0.34) and by central photo review 64.2% vs 72.0% (p=0.11).
IMPORT HIGH tested a simultaneous integrated boost in 15 fractions against a sequential boost in the same setting; its effect sizes are not in this source. This is the larger North American test of the same question, enriched for grade 3 and node-positive disease.
Unblinded. The noninferiority margin (HR 2.12) was set under a protocol redesign against an assumed 1.59% 5-yr IBR, and the point estimate favored sequential (HR 1.31) on 56 total events. Cosmesis response rates fell to 50.5% (physician) and 47.1% (central photo) by 3 years.
Randomized phase 3, prespecified noninferiority met at 7.3-yr median follow-up; wide NI margin (HR 2.12) and a point estimate favoring sequential keep it below practice-changing.
In high-risk early breast cancer after lumpectomy (grade 3, ER-negative, node-positive, or close margins) this supports a 15-fraction concurrent boost in place of a sequential boost; it does not address boost omission, partial breast irradiation, or post-mastectomy RT.
- Durability of the concurrent boost beyond 7 years recruiting 5 fr Ultrahypofractionated WBI and SIB for Breast Cancer With Unfavorable Characteristics Phase NAn=458 · primary completion 2029-06 · randomised 5fr WBI+SIB vs 15fr WBI+SIB noninferiority
- Whether a concurrent boost transfers to regional nodal irradiation active Hypofractionated Loco-regional Adjuvant Radiation Therapy of Breast Cancer Combined With a Simultaneous Integrated Boost Phase NAn=2963 · primary completion 2021-07 · loco-regional hypofx with SIB, late morbidity 1° EPrecruiting Ultra-Hypofractionated vs Moderate Hypofractionated Radiotherapy for Regional Lymph Nodes in High Risk Breast Cancer Phase NAn=1950 · primary completion 2034-03 · randomised ultrahypofx vs moderate hypofx RNI, n=1950
- Boost omission versus concurrent boost in high-risk pts n=400 · primary completion 2025-11 · WBI +/- tumor bed boost in HER2+, 7y IBTR endpoint
📚 Sources · 📄 1 paper
Abstract
PIVOTALboost
ForHigh-risk localised prostate, 20-fraction IMRT candidates
TL;DRLate 2yr G2+ bowel 8.2% / 8.7% / 6.5% and bladder 19.5% / 24.1% / 16.5% across prostate, +boost, +pelvic nodes arms.
The late bladder G2+ signal sits with the boost, not the nodes: 24.1% in P+B vs 19.5% prostate-only and 16.5% in PPN+B, so adding elective nodal volume did not track with worse 2yr bladder or bowel toxicity. That makes the 20-fraction focal boost plus pelvic node volume a tolerable technique choice while the biochemical/clinical failure endpoint matures.

| Arm (n) | Bowel G2+ (95% CI) | Bladder G2+ (95% CI) |
|---|---|---|
| Prostate (n=281) | 8.2% (5.7-11.7) | 19.5% (15.5-24.4) |
| Prostate+Boost (n=345) | 8.7% (6.3-12.1) | 24.1% (20.2-28.7) |
| Prostate+Nodes+Boost (n=347) | 6.5% (4.5-9.5) | 16.5% (13.1-20.6) |
+2 more figures
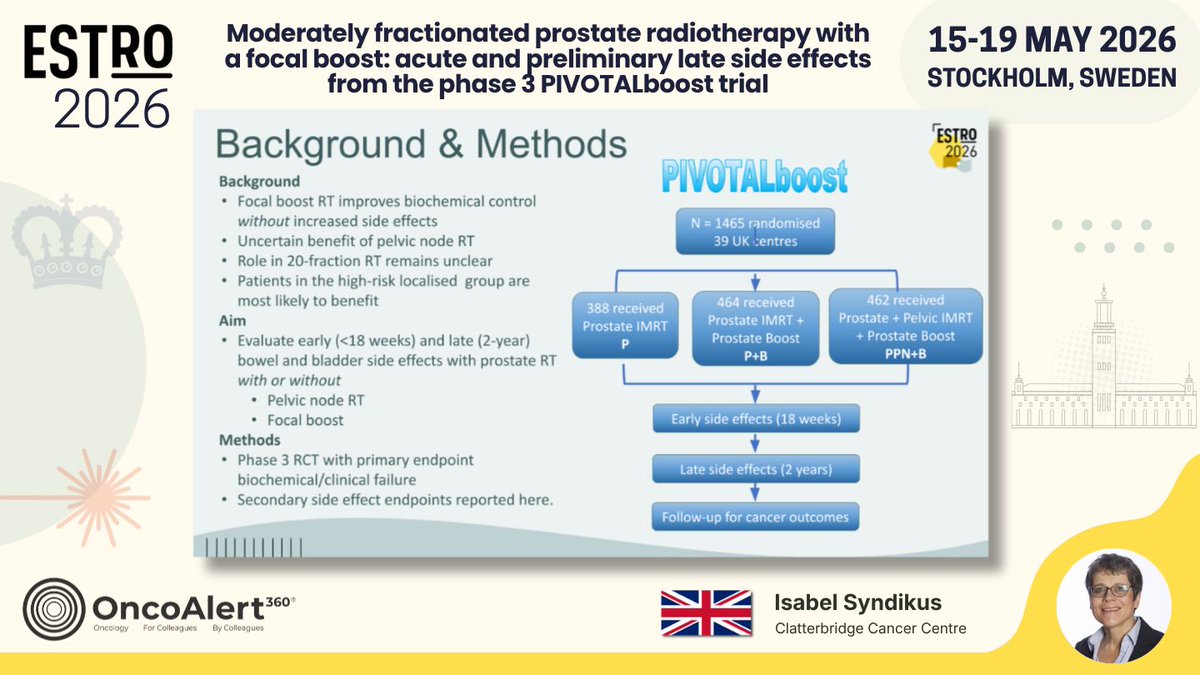
| Arm | Received |
|---|---|
| Prostate IMRT | 388 |
| Prostate IMRT + Boost (P+B) | 464 |
| Prostate + Pelvic IMRT + Boost (PPN+B) | 462 |

8 details 5 trials watching
Phase 3 RCT, N=1465 randomised across 39 UK centres. Primary endpoint: biochemical/clinical failure; the side-effect endpoints presented here are secondary.
Localised prostate cancer; the trial rationale states high-risk localised pts are most likely to benefit from pelvic node RT. Full eligibility criteria not reported in source.
20-fraction moderately hypofractionated IMRT. Arms as received: prostate alone (388), prostate + focal prostate boost (464), prostate + pelvic nodes + boost (462). Boost dose and nodal dose not reported in source.
Reported here: early bowel and bladder side effects (<18 weeks) and late (2-year, 6-24 month) G2+ events. Cancer-outcome follow-up is ongoing.
Nodal RT increased early bowel side effects, which resolved by 18 weeks post-RT. At 2 years G2+ bowel and bladder rates were similar across arms, with the numerically highest late bladder rate in the boost-without-nodes arm.
Late analysis covers only the 973 (74%) with ≥2yr follow-up, and no between-arm p-values are reported in source. The efficacy primary endpoint is unreported, so the toxicity read cannot yet be set against a benefit.
Randomised phase 3, prespecified secondary toxicity endpoint, 2yr follow-up. Efficacy 1° EP not yet reported, so it supports safety only, not a practice change.
In high-risk localised prostate pts being planned for 20-fraction IMRT, this supports the safety of adding a focal intraprostatic boost and elective pelvic nodal coverage; it does not yet speak to whether either improves biochemical or clinical control.
- Does focal boost or pelvic nodal RT improve biochemical/clinical failure recruiting A Trial of 5 Fraction Prostate SBRT Versus 5 Fraction Prostate and Pelvic Nodal SBRT Phase 3n=1128 · primary completion 2028-06 · phase 3 prostate-only vs prostate + pelvic nodal SBRTn=250 · primary completion 2031-05 · PSMA-N0M0 high risk, PORT vs whole pelvis RTrecruiting Addition of Focal Boost to Primary Radiotherapy for Prostate Cancer in 12 or 20 Fractions Phase NAn=1016 · primary completion 2040-10 · tests if intraprostatic boost improves cure rates
- Do late toxicity differences emerge beyond 2 years n=700 · primary completion 2021-12 · longitudinal GI/GU toxicity after whole-pelvis IMRTn=68 · primary completion 2025-10 · 5y accumulated GI/GU toxicity, integrated index boost
- Boost and nodal dose/fractionation details for reproducibility
📚 Sources · 🐦 1 tweet
Day THREE of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 17, 2026
Moderately fractionated prostate radiotherapy with a focal boost: acute and preliminary late side effects from the phase 3 PIVOTALboost trial Presented by Isabel Syndikus 🇬🇧 #RadOnc ☢️
In the PIVOTALboost trial, we treated 1314… pic.twitter.com/cGuR1j2Qos
APBI-IMRT Florence NCT02104895
ForPost-BCS early breast cancer, pT <25mm, margins ≥5mm, age >40
7.7% vs 4.2% at 15yr
HR 1.57 (95% CI 0.82-3.04), p=0.17
TL;DR15yr IBTR 7.7% APBI vs 4.2% WBI, HR 1.57 (0.82-3.04) p=0.17; excess is new primaries, not true local relapse.
The 15yr excess sits in new ipsilateral primaries (5.9% vs 2.7%, p=0.09), not true local relapse (2.1% vs 1.6%). That splits the decision: 30Gy in 5# to the tumour bed holds the bed, but leaves untreated breast tissue at risk, which is a surveillance and endocrine-adherence question rather than an argument for whole-breast coverage.

| Endpoint (15-year) | APBI N (%) | WBI N (%) | P-value |
|---|---|---|---|
| Ipsilateral breast tumour recurrence | 20 (7.7) | 11 (4.2) | 0.14 |
| Local relapse | 5 (2.1) | 4 (1.6) | 0.75 |
| New ipsilateral breast cancer | 15 (5.9) | 7 (2.7) | 0.09 |
| Locoregional tumour recurrence | 20 (7.2) | 13 (5.0) | 0.28 |
| Contralateral breast tumour | 10 (3.8) | 13 (5.0) | 0.67 |
| Distant metastasis | 7 (2.7) | 12 (4.6) | 0.35 |
| Deaths | 56 (21.5) | 51 (19.6) | 0.66 |
+2 more figures


10 details 1 trial watching
Phase III equivalence trial, n=520, 1:1 randomisation, accrued 2005-2013, single institution. Powered on a 5-year estimated IBTR of 3% with a 5% equivalence margin and 80% power. Survival outcomes analysed ITT; toxicity and cosmesis per protocol after 14 withdrawals.
Post breast-conserving surgery, pT <25 mm, final surgical margins ≥5 mm, age >40 years. Nodal status and receptor subtype not specified in the source slides.
APBI arm: 30 Gy in 5 fractions IMRT to the partial breast. WBI arm: 50 Gy in 25 fractions plus a 10 Gy in 5 fraction tumour-bed boost. The comparator is a conventionally fractionated whole-breast course, not a modern hypofractionated 26 Gy/5 or 40 Gy/15 schedule.
IBTR HR 1.57 (95% CI 0.82-3.04), p=0.17 at 15 years. The gap widens across timepoints (5yr 2.3% vs 1.2%, 10yr 4.2% vs 2.7%, 15yr 7.7% vs 4.2%) but never reaches significance.
The only 5-fraction PBI dataset reporting to 15 years. IMPORT LOW and NSABP B-39 support PBI at shorter follow-up with different fractionation, so this trial carries the durability question for the ultrahypofractionated schedule specifically.
Powered for 5-year equivalence, so the 15-year read is descriptive rather than a met endpoint. Single institution. The local relapse vs new primary split that carries the interpretation is investigator-adjudicated, not molecularly confirmed.
Randomised phase III, prespecified 5yr equivalence endpoint, 15yr mature f/u, no significant divergence on any oncologic endpoint. Reinforces PBI as a listed option.
In the post-BCS pt over 40 with a pT <25mm tumour and ≥5mm margins, this supports 5-fraction PBI as a durable option out to 15 years; it does not extend to node-positive disease, close margins, or younger pts, and the untreated-breast new-primary rate is the tradeoff to counsel.
- Does the new-primary excess keep widening past 15 years
- Do modern hypofractionated WBI schedules change the comparison recruiting Ultra-hypofractionated for Whole Breast Irradiation (WBI) Compared to Partial Breast Irradiation (PBI) Phase 2n=100 · primary completion 2026-05 · randomised 26 Gy/5 fx WBI vs same-dose PBI
📚 Sources · 🐦 1 tweet
📌 Fifteen-year outcomes of the randomised APBI-IMRT Florence phase Ill trial of partial versus whole-breast irradiation in early breast cancer ✨
— Elisabetta Bonzano MD, PhD (@to_be_elizabeth) May 17, 2026
Excellent presentation led by @CarlottaB 👏🏻#ESTRO26 @Icro_Meattini @ESTRO_RT @OncoAlert #OncoAlertAF pic.twitter.com/1j4bIA2nyC
IMPORT HIGH
ForInvasive early breast pT1-3 pN0-pN3a M0 post-BCS requiring tumour bed boost
3.5% vs 3.7% vs 5.5% at 10yr
95% CI 2.4-5.0 / 2.6-5.3 / 4.1-7.3
TL;DR10yr IBTR 3.5% vs 3.7% vs 5.5% across 40+16Gy, 48Gy SIB, 53Gy SIB; further escalation adds nothing.
The transferable parameter is 48Gy/15F in 3 weeks with the boost built in, no separate 8-fraction phase, holding IBTR at 3.7% at 10yr with moderate/marked distortion under 18%. The 53Gy arm settles the escalation question: 5.5% IBTR, worse not better, so the decision this moves is boost delivery (SIB vs sequential), not boost dose.

| Arm | 10-yr IBTR (95% CI) | Absolute OS diff vs 40Gy/15F |
|---|---|---|
| 40Gy/15F + 16Gy/8F | 3.5% (2.4, 5.0) | reference |
| 48Gy/15F (3.2Gy/F) | 3.7% (2.6, 5.3) | -0.5 (-3.0, 2.8) |
| 53Gy/15F (3.5Gy/F) | 5.5% (4.1, 7.3) | 1.5 (-1.4, 5.1) |
+2 more figures

| Arm | N | 5-yr IBTR (95% CI) |
|---|---|---|
| 40Gy/15F + 16Gy/8F | 871 | 1.9% (1.2, 3.1) |
| 48Gy/15F (3.2Gy/F) | 874 | 2.0% (1.2, 3.2) |
| 53Gy/15F (3.5Gy/F) | 872 | 3.2% (2.2, 4.7) |

9 details 4 trials watching
Phase 3 randomised 1:1:1, N=2617 across 76 UK hospitals, accrued 2009-2015. Annual clinical follow-up to 10 years; PROs and photographs collected only to 5 years.
Women ≥18 years after breast conserving surgery for invasive early breast cancer, pT1-3, pN0-pN3a, M0, all requiring tumour bed boost RT. Described by the investigators as a higher-than-average risk group.
Control was 40Gy/15F whole breast plus sequential 16Gy/8F boost. Both experimental arms used a simultaneous integrated boost in 15 fractions over 3 weeks, 48Gy (3.2Gy/F) or 53Gy (3.5Gy/F) to the tumour bed, with a modest dose reduction to whole breast distant from the tumour.
Primary: ipsilateral breast tumour relapse (IBTR), reported here at 10 years. Secondary reporting covers overall survival and clinician-assessed late normal tissue effects.
Moderate/marked AEs at 10 years were low across all randomised groups: breast distortion/shrinkage <18%, induration <10%, telangiectasia <2%, breast oedema <2%. No arm-specific late toxicity split is given in the source.
At 5 years (Coles, Lancet 2023) IBTR was 1.9% / 2.0% / 3.2%, and 48Gy was declared non-inferior in absolute terms. The 10-year data preserve that ordering, and both 40+16Gy and 48Gy stay below the 5% control estimate assumed in the original sample size calculation.
Source reports absolute rates only, no between-arm HRs or non-inferiority p-values at 10 years. PRO and photographic cosmesis stopped at 5 years, so 10-year toxicity is clinician-scored. Conference presentation, not yet a full peer-reviewed 10-year report.
The practical yield is logistic as much as oncologic: SIB collapses boost into the same 15 fractions, cutting visits without paying an IBTR or late-toxicity penalty. Further escalation to 53Gy does not help, which closes the dose-escalation arm of this question in a boost-indicated population.
Randomised 3-arm phase 3, prespecified 10-yr follow-up of a published primary; reaffirms 48Gy/15F SIB rather than changing it. No new comparator.
In pT1-3 pN0-pN3a post-BCS pts you would otherwise book for 40Gy/15F plus a sequential 16Gy boost, this supports a 15-fraction 48Gy SIB as an equivalent-control option; it does not speak to boost omission in low-risk pts, who were not the population studied.
- Does SIB benefit extend to post-mastectomy or nodal RT settings?
- Which boost-indicated subgroups could safely omit boost entirely? n=295 · primary completion 2029-11 · RT omission in low-risk DCIS, age >=50
- Five-fraction SIB as the next de-escalation step? recruiting Ultra-hypofractioNated Adjuvant Radiotherapy ± sImultaneous Integrated Boost for Low-risk Breast Cancer Patients Phase 2n=65 · primary completion 2025-10 · phase 2 ultrahypofx WBI +/- SIB, feasibilityn=50 · primary completion 2029-02 · ultra-short WBI with SIB, cosmesis + PROM endpointsrecruiting 5 fr Ultrahypofractionated WBI and SIB for Breast Cancer With Unfavorable Characteristics Phase NAn=458 · primary completion 2029-06 · randomised 26/30Gy 5fr SIB vs 40.05/48Gy 15fr SIB
📚 Sources · 🐦 1 tweet
Day THREE of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 17, 2026
Ten-year results of the IMPORT HIGH trial (ISRCTN47437448): Dose escalated simultaneous integrated boost radiotherapy in early breast cancer Presented by Charlotte Coles 🇬🇧 #RadOnc ☢️
Ten-year IMPORT HIGH trial data show that a… pic.twitter.com/7RqVy2SrQm
HypoG-01
ForBreast cancer receiving adjuvant RT + tumour-bed boost per HypoG-01 eligibility
TL;DR118 first events at 4.8y median f/u; LRR infrequent and mostly in-volume, patterns comparable between 40Gy/15fx and 50Gy/25fx.
The contouring read matters more than the fractionation read here: 20/30 recurrence sites fell in-volume and 19/30 nodal recurrences sat in L1-L2, so ESTRO CTV definitions covered where disease actually came back. That supports keeping current axillary level coverage rather than expanding target volumes when moving to 40 Gy/15 fx.

| Event type | n |
|---|---|
| Isolated LRR | 19 |
| Concomitant LRR | 1 |
| Isolated distant recurrence | 61 |
| Second malignancy | 37 |
| Total first events | 118 |
+1 more figure

9 details
Pre-planned secondary analysis (ITT) of the HypoG-01 phase III randomised trial. N=1,260, median follow-up 4.8 years.
Randomisation was 40 Gy/15 fractions over 3 weeks vs 50 Gy/25 fractions over 5 weeks, each with a tumour-bed boost. Target volumes followed ESTRO contouring guidelines.
First oncological event: locoregional recurrence (LRR), distant recurrence (DR), or second malignancy. LRR classified against the CTV as in-volume, marginal (outside CTV, ≥50% prescribed dose), or out-of-volume (<50%), with planned dose at the recurrence site re-estimated on the initial RT-plan CT.
118 first events. LRR was the lowest-frequency event type; distant recurrence (n=61) and second malignancy (n=37) dominated. 20/30 recurrence sites were in-volume (67%) and 19/30 nodal sites were mainly levels I and II.
Arm-level event counts are not reported in the source, so the "no obvious difference" claim between arms cannot be checked. With roughly 20 LRR events total, the analysis is descriptive and underpowered to exclude a modest fractionation effect on failure pattern.
The actionable signal is target-volume adequacy rather than fractionation: recurrences clustered inside the treated volume and in axillary levels I-II, which argues the ESTRO CTV is catching the right anatomy rather than that coverage needs widening. Out-of-volume failures would have been the argument for larger fields; they were the minority.
Pre-planned secondary analysis of a randomised phase III; supports moderate hypofractionation and ESTRO contouring. Event count (19 iLRR) too small for a powered arm comparison.
In breast pts eligible for adjuvant RT with a tumour-bed boost, this supports 40 Gy/15 fx with standard ESTRO-guided CTVs without widening nodal volumes; it does not address ultra-hypofractionation or pts whose recurrence risk sits outside the trial's eligibility.
- Do failure patterns hold with ultra-hypofractionation (5-fraction) schedules?
- Does boost technique alter in-volume vs marginal recurrence distribution?
📚 Sources · 🐦 1 tweet
Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 16, 2026
Patterns of locoregional and distant recurrence and dosimetric analysis in the HypoG-01 phase III trial Presented by Louis Munschi 🇫🇷 #RadOnc ☢️
In the HypoG-01 phase III trial (1260 patients, median follow-up 4.8 years), 118… pic.twitter.com/ogARInu0fB
DBCG HYPO
ForNode-negative early breast cancer or DCIS after breast-conserving surgery
24.7% vs 19.5% at 10 yr
HR 0.76 (95% CI 0.62-0.92), p=0.005 favouring 40 Gy/15 fx
TL;DR10-yr grade 2-3 breast induration 19.5% with 40Gy/15fx vs 24.7% with 50Gy/25fx, HR 0.76, p=0.005; no recurrence or survival cost.
The induration difference is not just non-inferiority, it favours 40 Gy/15 fx (24.7% vs 19.5%, HR 0.76, p=0.005), so the shorter course is the lower-fibrosis option, not merely the more convenient one. Applies to node-negative and DCIS whole-breast fields; boost and nodal coverage are not addressed in source.

| Endpoint | 50 Gy/25 fx | 40 Gy/15 fx | Effect size |
|---|---|---|---|
| 10-yr grade 2-3 induration | 24.7% | 19.5% | HR 0.76 (95% CI 0.62-0.92), p=0.005 |
| 10-yr overall survival | 92.1% | 93.0% | HR 0.81 (95% CI 0.63-1.04), p=0.10 |
+1 more figure

9 details 5 trials watching
Phase III randomised non-inferiority trial, 1:1, run across Denmark, Norway and Germany with accrual 2009-2014. Median follow-up 12.8 years; these are the prespecified 10-year analyses.
1,882 women with node-negative breast cancer or DCIS. Allocation was 949 to 50 Gy and 933 to 40 Gy after exclusions; 936 and 917 women respectively carried forward in the flow diagram.
Whole-breast RT only: 50 Gy in 25 fractions vs 40 Gy in 15 fractions. No boost, nodal target volume, or technique detail (IMRT vs 3D, prone vs supine) is reported in the source.
Primary: grade ≥2 breast induration at 3 years, scored at two consecutive visits or at final follow-up. Morbidity assessed at years 0, 1, 2, 3, 4, 5 and 10; recurrence and survival were prespecified 10-year secondary analyses.
Induration is the toxicity endpoint here and it favours the hypofractionated arm. No other late-effect domain (cardiac, pneumonitis, cosmesis scoring, second malignancy) is reported in the source.
Consistent with START-B and the UK long-term hypofractionation experience, but adds prospectively scored induration out to 10 years in a trial that also enrolled DCIS.
Locoregional recurrence, distant failure and breast cancer mortality are reported only as not significantly different, with no event counts, HRs, or non-inferiority margin in the source. Induration scoring is clinician-assessed and not blinded to fractionation.
Prespecified 10-yr analysis of a randomised phase III with 12.8-yr median f/u; reinforces moderate hypofractionation already standard worldwide.
In node-negative invasive breast cancer or DCIS after lumpectomy, this supports 40 Gy/15 fx over 50 Gy/25 fx on long-term induration as well as convenience; it does not speak to node-positive pts needing regional nodal irradiation.
- Does the induration advantage hold with a tumour bed boost? active Hypofractionation With Simultaneous Integrated Boost vs. Standard Fractionation in Early Breast Cancer Phase NAn=2324 · primary completion 2019-01 · hypofx + SIB vs standard fractionation, n=2324n=132 · primary completion 2026-03 · 40 Gy/15 fx + SIB boost, 4y fibrosis 1° endpoint
- How does 40 Gy/15 fx compare with 26 Gy/5 fx at 10 years? n=2100 · primary completion 2029-03 · 1 wk vs 3 wk adjuvant RT, non-inferiority, n=2100recruiting 5 fr Ultrahypofractionated WBI and SIB for Breast Cancer With Unfavorable Characteristics Phase NAn=458 · primary completion 2029-06 · randomised 26 Gy/5 fx vs 40.05 Gy/15 fx, both SIBrecruiting Ultra-Hypofractionated vs Moderate Hypofractionated Radiotherapy for Regional Lymph Nodes in High Risk Breast Cancer Phase NAn=1950 · primary completion 2034-03 · 26 Gy/5 fx vs 40 Gy/15 fx nodal RT, f/u to 2034
📚 Sources · 🐦 1 tweet
Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 17, 2026
10-year Follow-Up of the DBCG HYPO Trial: Breast Induration, Recurrence and Survival After Hypofractionated Whole Breast Irradiation Presented by Hanna Forsberg 🇩🇰 @BOffersen #RadOnc ☢️ #BreastCancer
The DBCG HYPO trial reports… pic.twitter.com/4qf9R3HZwT
OligoCare
ForOligometastatic solid tumors treated with SABR; prostate/NSCLC/CRC/breast…
TL;DRReal-world SABR local in-field progression 5.0% at 1yr, 11.4% at 3yrs across 2447 pts / 3533 lesions; CRC worst.
The histology split is the actionable read: CRC 3yr in-field failure 19.6% vs prostate 8.1%, despite CRC receiving the highest median dose per fraction. That argues for dose escalation or a combination strategy in CRC mets specifically, and it puts minimum PTV dose (not prescription dose) on the plan-review checklist.

| Primary | n | 1 year | 3 years |
|---|---|---|---|
| Colorectal | 518 | 9.3% | 19.6% |
| Breast | 378 | 4.1% | 11.3% |
| NSCLC | 530 | 6.0% | 9.8% |
| Prostate | 1021 | 2.7% | 8.1% |
+2 more figures


10 details
EORTC OligoCare prospective real-world registry of SABR for oligometastatic disease, 57 institutions, accrual July 2019 to July 2025. Interim analysis; median follow-up 31 months (minimum 6).
2447 eligible pts with 3533 lesions. Median age 69 (28-94), 69% male. Primary tumors: prostate 1021 (42%), NSCLC 530 (22%), colorectal 518 (21%), breast 378 (15%).
SABR to metastatic sites; lesion locations were lung 807 (23%), non-vertebral bone 869 (25%), non-regional lymph node 558 (16%), spine 515, liver 306 (9%), brain 231 (7%), other 247 (7%). Minimum PTV dose correlated with outcome and is named the most critical technical factor; prescription dose and fractionation not reported in source.
Local in-field progression reported as cumulative incidence. No primary endpoint stated in the source; no survival or systemic-progression endpoints given here.
Local in-field progression 5.0% at 1 year and 11.4% (99% CI 10.0-12.9%) at 3 years, i.e. 88.6% local control at 3 years, 237 events among 2447 pts.
Colorectal primaries failed most (19.6% at 3 years) despite the highest median dose per fraction, which the authors read as relative radioresistance rather than underdosing and a case for dose escalation or combination approaches. De novo oligometastatic disease outperformed repeat OMD, attributed to higher delivered dose.
Registry design with no comparator arm and heterogeneous dose/fractionation across 57 centres; indication and selection bias are unaddressed in source. Safety and toxicity outcomes are not reported in the source content.
Large prospective multi-site registry with explicit histology-stratified analyses, but non-randomised and no comparator; supports rather than tests current oligomet SABR practice.
In a CRC oligomet being planned for SABR, this registry supports treating minimum PTV dose as the coverage constraint to scrutinize and sets a realistic ~1 in 5 three-year in-field failure expectation; it does not extend to unirradiated or non-oligometastatic disease.
- Optimal dose escalation strategy for colorectal oligometastases
- Minimum PTV dose threshold for durable local control
- Whether repeat OMD failure reflects dose or biology
📚 Sources · 🐦 1 tweet
📣 #ESTRO26 - @UmbertoRicardo e2irradiate @EORTC prospective OLIGOCARE registry of SABR for oligomets. ~2500 patients, ~3500 mets.
— Shankar Siva (@_ShankarSiva) May 17, 2026
➡️ local failure 5% at 1 year and 11% at 3 years
➡️ Colorectal cancer has higher risk of progression
➡️ minimum PTV dose correlated with outcome… pic.twitter.com/cx4zERqHhK