Caveats dominate
ProtecT (secondary analysis: cribriform morphology)
ForPSA-screened clinically localized prostate cancer, GG1-2 predominant
TL;DRCribriform-negative pts (87%): radical Rx gave no significant 15yr metastasis reduction vs active monitoring; cribriform-negative GG2 matched GG1 risk.
Reported via UroToday →
Selection, not technique, is the RT read: cribriform-negative GG2 matched GG1 on 15yr metastasis risk and gained no significant benefit from radical treatment, so definitive RT is deferrable there. Cribriform-positive (~13%) is where local treatment changed metastasis outcomes, moving the surveillance-vs-treat decision at biopsy.
Selection, not technique: cribriform-negative GG2 matched GG1 on 15yr metastasis risk and got no significant benefit from radical treatment, so definitive RT is deferrable there. Cribriform-positive (~13%) marks the group where local treatment changed metastasis outcomes, sharpening who to irradiate versus monitor at biopsy.
First trial-level backing for EAU's advice against active surveillance in any cribriform disease, which previously rested on no prospective data. Cribriform-negative GG2 behaved like GG1, supporting continued surveillance; cribriform-positive (~13%) flags pts for radical prostatectomy or RT despite a localized presentation.
8 details
Secondary analysis of the ProtecT RCT. Cribriform status was not a randomization characteristic; biopsy slides from 712 of 1,643 randomized pts were centrally reviewed, with centralization still ongoing.
PSA-detected clinically localized prostate cancer. ~13% cribriform-positive on biopsy, 87% cribriform-negative. Gleason re-graded to 2019 ISUP from the original 2005 criteria, which did not change the result.
The radical-treatment options were surgery or EBRT with 3-6mo neoadjuvant ADT. The RT+ADT arm carried a higher cribriform prevalence, attributed to chance since cribriform was not randomized.
Primary outcome was metastases at 15yr median follow-up, analyzed by both intention-to-treat and per-protocol (accounting for crossover between assigned and received treatment).
In cribriform-negative pts (87%), early radical Rx gave no significant 15yr metastasis reduction vs active monitoring, in ITT and per-protocol. Cribriform-negative GG2 matched GG1 metastasis risk on multivariable Cox.
The cribriform-positive group carrying the clinical message is small (~13% of the 712 reviewed), and its metastasis effect size is not reported in source. The 20yr ProtecT follow-up (census just reached) is not yet available.
Post-hoc analysis of a non-randomized histologic feature; only 712 of 1,643 randomized pts had slides reviewed. Cribriform-positive effect size not reported in source.
In cribriform-negative GG2 localized prostate cancer, this supports active surveillance as reasonable (same 15yr metastasis risk as GG1); it does not extend to cribriform-positive disease, which the data marks as higher-risk.
- Magnitude of radical-treatment benefit in cribriform-positive pts
- Should cribriform status formally gate active surveillance eligibility
- Does 20yr ProtecT follow-up confirm the cribriform signal
📚 Sources · 📄 1 paper
Abstract
SUPREMO
ForPost-mastectomy breast cancer, pN0 or 1-3 positive nodes
TL;DR10yr chest-wall recurrence 1.1% vs 2.5% (HR 0.45), no DFS/OS gain, but trial prohibited RNI so tests incomplete PMRT.
Even with SUPREMO's truncated field (chest-wall RT alone, supraclav in just 12%), the supplement shows local recurrence still fell 4.8% to 3.3% (HR 0.51) in node-positive pts. A partial RT field still helping argues FOR nodal irradiation, not omission, in 1-3 node+ disease, so the null OS/DFS shouldn't justify omitting PMRT.
Also covered Jul 7
8 details 4 trials watching
ASO editorial (Naoum, Taghian) critically evaluating SUPREMO. SUPREMO randomized post-mastectomy pts to chest-wall irradiation vs observation; RNI was prohibited, so it tested chest-wall RT alone, not chest-wall plus nodal PMRT.
Only 25% truly node-negative; the majority had N1 (1-3 positive nodes). 65% hormone-receptor-positive, 10% triple-negative. Post-neoadjuvant pts are out of scope.
Chest-wall irradiation alone. Supraclavicular coverage reached only 12% of the PMRT arm (n=97), internal mammary RT under 2% both arms, and regional nodal irradiation was otherwise prohibited.
No DFS or OS benefit from chest-wall irradiation; the only positive signal is reduced local recurrence (see table).
| Endpoint | CW-RT | No RT | Effect |
|---|---|---|---|
| 10yr chest-wall recurrence | 1.1% | 2.5% | HR 0.45 |
| LRR (supplement) | 3.3% | 4.8% | HR 0.51 (0.27-0.96) |
Danish and British Columbia trials, plus MA-20 and EORTC 22922, showed regional nodal RT improves LRR, DFS, and breast-cancer mortality in 1-3 node+ disease, even after ALND. SUPREMO's chest-wall-only field never tested this.
Node-negative dilution (25%) may mask node-positive benefit; incomplete nodal field; TNBC (10%) underpowered with a paradoxical forest-plot direction; only 10-year follow-up for a 65% HR-positive cohort prone to late recurrence.
The editorial's read: SUPREMO's null headline should not license omitting PMRT in node-positive pts, because it never tested chest-wall plus nodal RT. Even its truncated field improved node-positive local recurrence, consistent with the Danish, British Columbia, and EBCTCG data.
SUPREMO tested chest-wall RT alone, prohibited RNI, and diluted with 25% node-negative pts, so its null DFS/OS can't establish PMRT omission for node-positive disease.
In 1-3 node-positive post-mastectomy pts, this critique cautions against reading SUPREMO as clearance to omit nodal RT; it does not extend to truly node-negative pts, where SUPREMO and EBCTCG show no PMRT benefit.
- Full nodal RT vs chest-wall-only PMRT in 1-3 node-positive disease active Standard or Comprehensive Radiation Therapy in Treating Patients With Early-Stage Breast Cancer Previously Treated With Chemotherapy and Surgery Phase NAn=1636 · primary completion 2023-09 · comprehensive nodal vs standard RT, phase 3active Postmastecomy Internal Mammary Nodal Irradiation for High-risk Breast Cancer Patients Phase 3n=2400 · primary completion 2025-11 · randomised IMN nodal RT vs none, DFS endpointrecruiting The T-REX Trial: Tailored Regional External Beam Radiotherapy in Clinically Node-negative Breast Cancer Patients With 1-2 Sentinel Node Macrometastases. Phase NAn=1350 · primary completion 2028-12 · randomised omission of regional RT, 1-2 macrometsrecruiting RecurIndex Guided Avoidance of Regional Nodal Irradiation for Node Positive Breast Cancer Phase NAn=540 · primary completion 2029-08 · RNI vs avoidance in N1, RecurIndex-guided
- PMRT value in triple-negative post-mastectomy disease
📚 Sources · 📄 1 paper
FIRESTORM
ForHigh-risk meningioma: WHO grade 2 STR or recurrent, postop RT
TL;DR5-yr PFS 65.8% vs 38.8% favoring dose-escalated RT (BED ≥79.2 Gy), HR 0.40; OS not improved.
The trade-off is the actionable read: escalating to BED ≥79.2 Gy (≈66 Gy/33 fx) roughly doubled 5-yr PFS (65.8% vs 38.8%) but tripled any-grade radionecrosis (33.9% vs 13.2%), with severe RN unchanged (5.1% vs 3.2%) and no OS gain. Benefit was largest after subtotal resection.
9 details 3 trials watching
Individual patient-level meta-analysis pooling 7 institutions, N=248 (59 DE-RT, 189 SD-RT). Retrospective, non-randomized; compared by Kaplan-Meier, Cox multivariable, and IPTW propensity analysis.
High-risk meningioma: 75.8% WHO grade 2, 41.5% recurrent (grade 3 the remainder), 75.2% subtotal resection.
DE-RT defined as biologically effective dose ≥79.2 Gy (equivalent 66 Gy/33 fx); SD-RT comparator conventionally fractionated 59.4 Gy/33 fx or 60 Gy/30 fx. Mixed photon/carbon vs photon-alone DE-RT showed no PFS difference (81.3% vs 92.0% at 3y, P=.34).
Primary: progression-free survival, DE-RT vs SD-RT. Also overall survival and CNS radionecrosis.
OS not improved despite the PFS gain: 5-yr OS 83.8% vs 68.4% (P=.056 UVA), non-significant on MVA (HR 0.66, P=.27) and IPTW (HR 0.77, P=.42).
| Endpoint | DE-RT | SD-RT |
|---|---|---|
| 3-yr PFS | 86.4% | 55.6% |
| 5-yr PFS | 65.8% | 38.8% |
| Adjusted HR (MVA) | 0.40 (0.24-0.69), P=.001 | ref |
| IPTW HR | 0.45 (0.24-0.83), P=.01 | ref |
| Radionecrosis | DE-RT | SD-RT |
|---|---|---|
| Any grade | 33.9% (20/59) | 13.2% (25/189) |
| Grade 3+ | 5.1% | 3.2% |
Any-grade radionecrosis higher with DE-RT (33.9% vs 13.2%, P=.001) but grade 3+ similar (5.1% vs 3.2%); most RN was low-grade.
Standard-dose postoperative meningioma RT (RTOG-0539 high-risk 60 Gy, EORTC-22042 60 Gy) sits at/below this cohort's SD-RT arm; the dose-response signal here motivates the ongoing randomized escalation question.
Retrospective non-randomized pooling: DE-RT allocation confounded, IPTW mitigates but cannot fully adjust. PFS gain without OS benefit; prior-RT and grade imbalance across arms.
Retrospective non-randomized IPD pooling; DE-RT allocation confounded despite IPTW. PFS-only gain, no OS benefit. Signal supports escalation but needs randomized confirmation.
In high-risk meningioma (WHO grade 2, subtotally resected or recurrent) receiving postoperative RT, this supports a higher dose (BED ≥79.2 Gy) for local control; it does not extend to gross-totally-resected grade 1 disease or establish an OS benefit.
- Randomized confirmation of dose-escalated RT for high-risk meningioma active A Trial of Increased Dose Intensity Modulated Proton Therapy (IMPT) for High-Grade Meningiomas Phase NAn=21 · primary completion 2027-08 · increased-dose IMPT for high-grade meningioman=90 · primary completion 2028-12 · proton dose-escalation, 5y RFS in grade II/III
- Whether the PFS gain translates to an OS benefit
- Optimal escalation technique and dose (photon vs particle) recruiting Long-term Cognitive and Functional Impact of Proton-therapy or Modern Fractionated Radiotherapy in Cavernous Sinus Meningioma: An Open-label Randomized 1:1 Phase III Study Phase NAn=160 · primary completion 2032-02 · randomized proton vs photon RT, phase 3
📚 Sources · 📄 1 paper
Abstract
DeLLphi-304
ForRelapsed SCLC with brain mets, >70% prior CNS-directed therapy
TL;DRIntracranial: time-to-CNS-progression HR 0.54 ITT; in brain-mets pts CNS PFS 6.5 vs 4.2mo (HR 0.40), CNS CR 15% vs 5% for tarlatamab.
The RT read is intracranial control without new radiation: brain-mets CNS PFS 6.5 vs 4.2mo (HR 0.40) and CNS CR 15% vs 5%. But >70% had prior CNS-directed therapy, so this is salvage intracranial activity, not a defer-brain-RT signal in RT-naive disease. Informs sequencing systemic ahead of repeat cranial RT.

| Arm | Median CNS PFS | HR (95% CI) |
|---|---|---|
| Tarlatamab (n=254) | NE (13.7-NE) | 0.54 (0.39-0.75) |
| Chemotherapy (n=255) | 7.2 mo (5.6-NE) | n/a |
+2 more figures

| Arm | Median CNS PFS | HR (95% CI) |
|---|---|---|
| Tarlatamab (n=67) | 6.5 mo (4.3-13.7) | 0.40 (0.24-0.66) |
| Chemotherapy (n=56) | 4.2 mo (2.9-5.5) | n/a |
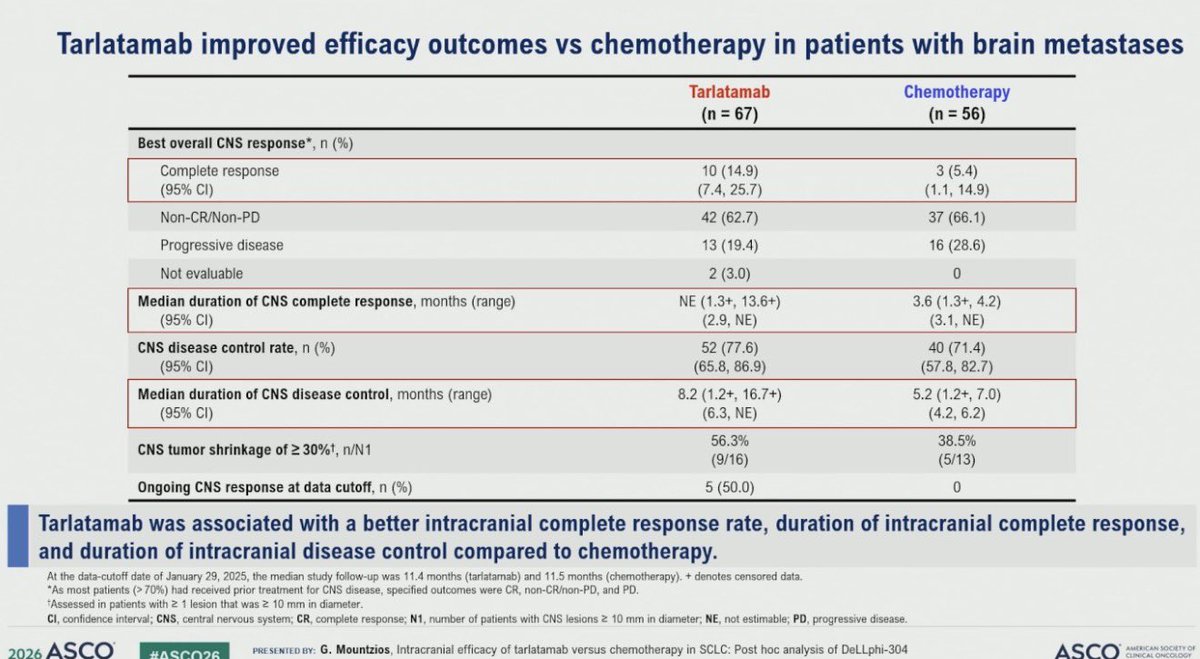
| CNS endpoint | Tarlatamab (n=67) | Chemotherapy (n=56) |
|---|---|---|
| Complete response | 10 (14.9%) | 3 (5.4%) |
| Disease control rate | 52 (77.6%) | 40 (71.4%) |
| Median duration CNS disease control | 8.2 mo | 5.2 mo |
5 details 2 trials watching
Post hoc intracranial analysis of DeLLphi-304, a phase 3 RCT of tarlatamab vs chemotherapy in relapsed SCLC. CNS endpoints were not prespecified primary. Data cutoff Jan 29 2025; median follow-up 11.4 mo (tarlatamab), 11.5 mo (chemo).
Relapsed SCLC. ITT CNS cohort n=254 tarlatamab vs 255 chemo; brain-mets subgroup n=67 vs 56. >70% of brain-mets pts had prior CNS-directed therapy.
Time to CNS progression or death (ITT, RECIST per investigator); brain-mets CNS PFS by mRANO-BM (BICR); best CNS response, CNS disease control rate, and response durations.
ITT time to CNS progression HR 0.54 (0.39-0.75), median NE vs 7.2 mo. Brain-mets CNS PFS and response detail in figures.
First DLL3xCD3 bispecific intracranial signal in SCLC; CNS control historically relied on WBRT/SRS and prophylactic cranial irradiation, not a systemic agent.
Post hoc, unstratified brain-mets HRs, small subgroup N. >70% prior CNS therapy confounds de novo intracranial activity. No new safety data in source.
Post hoc CNS analysis; brain-mets HRs unstratified with small N (67 vs 56), and >70% had prior CNS-directed therapy, confounding de novo intracranial activity.
For relapsed SCLC with previously-treated brain mets, this supports systemic intracranial control as an option before committing to repeat cranial RT; it does not inform RT-naive or symptomatic brain mets, where upfront local therapy still applies.
- Durability of intracranial response beyond current follow-up
- Activity in RT-naive or untreated brain metastases n=35 · primary completion 2029-02 · candidate match
- Sequencing tarlatamab vs cranial radiotherapy in SCLC brain mets n=39 · primary completion 2027-12 · candidate match
📚 Sources · 🐦 1 tweet
Dr. @g_mountzios #ASCO26 presents CNS outcomes with 2L tarlatamab in DeLLphi-304. Improved time to CNS progression overall (HR 0.54). In pts with brain nets, tarlatamab vs chemo CNS CR rate 15% vs 5% with DCR 78% vs 71% and time to CBS progression 6.5m vs 4.2m, HR 0.40 pic.twitter.com/5i8jL1zlKW
— Stephen V Liu, MD (@StephenVLiu) June 1, 2026
PROTEUS
TL;DRMost distant mets PSMA PET-detected (53.0% APA vs 60.7% control); preview NEJM data, MFS benefit's clinical meaning contested.
6 details 1 trial watching
Randomized, apalutamide + ADT vs ADT alone. Results just posted (NEJM online); full ASCO26 presentation pending, so this is a preview read.
Most distant metastases were PSMA PET-detected: 53.0% in the apalutamide group vs 60.7% in the control group. Primary MFS effect size not reported in source.
MFS events were predominantly PET-detected, raising lead-time / detection-bias concerns about the endpoint. The 50-vs-60 BCR/100 figures circulating are an illustrative hypothetical, not PROTEUS primary data.
Curator frames it as 'homerun vs largest negative' pending full data. A companion thought experiment argues PSMA PET vs conventional detection differences could account for much of the apparent metastasis delta.
Preview NEJM data; primary effect size not in source. Most MFS events PSMA PET-detected (53.0% vs 60.7%), raising lead-time/detection bias that undermines the MFS read.
- Does the MFS benefit hold on OS or conventional-imaging endpoints? n=1503 · primary completion 2026-06 · apalutamide MFS by conventional imaging (BICR)
- How much of the MFS delta reflects PSMA PET lead-time bias?
📚 Sources · 🐦 3 tweets
#ASCO26
— Daniel E Spratt (@DrSpratticus) May 31, 2026
The PROTEUS trial results are now online...buckle up as we wait to see the full presentation. This is going to be a trial that is likely highly controversial until the full results are published.
Some may call this a homerun, others may call this the largest negative…
Thought experiment:
— Sean McBride (@seanmmcbride) May 31, 2026
Let's take a very simple hypothetical trial involving 100 patients in the APA arm and 100 patients in the ADT alone arm. Pulling from PROTEUS EFS data, assume that, by 5 years, 60 patients in the ADT arm have had a BCR compared to 50 in the ADT+APA arm.… pic.twitter.com/WJaiDlJnQs
#ASCO26
— Daniel E Spratt (@DrSpratticus) May 31, 2026
Talk about real-time updates. NEJM paper now online and my predictions and inferences appear true.
Majority of MFS events were by PET not conventional imaging. "Most distant metastases were identified by PSMA PET (53.0% of those in the apalutamide group and 60.7% in the… https://t.co/Yz4myY0flq
OCEANUS
ForAdvanced/refractory NSCLC on immunoradiotherapy, median age 64, 74% male
TL;DRSequential iRT beat concurrent for real-world OS in newly-dx advanced NSCLC: median 20.3 vs 16.0 mo, HR 0.68 (0.47-0.99), P=.045.
Sequential iRT (ICI and RT not overlapping) beat concurrent for real-world OS in newly-dx advanced NSCLC, HR 0.68 (0.47-0.99), P=.045, favoring temporal separation of RT from ICI. RT dose, fractionation, and target volume aren't in the source, so the signal can't yet transfer to a specific plan. The refractory RT+ICI-maintenance read was NS (P=.20).
7 details 1 trial watching
Territory-wide real-world cohort (OCEANUS, Hong Kong CDARS, >90% population coverage); NSCLC diagnosed 2010-2021 who received iRT. Overlap-weighting propensity score primary, IPTW sensitivity; landmark-based OS with weighted Kaplan-Meier and Cox (restricted mean survival time where PH violated).
335 of 3522 ICI-treated pts received RT: 155 newly-dx advanced, 180 refractory. Median age 64 (34-90), 73.7% male. Refractory analysis required survival ≥90 days (landmark).
RT dose, fractionation, modality, and target volume not reported in source. The variable studied is timing of RT relative to ICI (sequential vs concurrent), not technique.
Both comparisons favored the sequential / ICI-maintenance arm (magnitudes in table). Chemotherapy was associated with longer OS in newly-dx pts only; not significant in refractory disease.
| Setting / comparison | Experimental OS | Control OS | HR / P value |
|---|---|---|---|
| Newly-dx advanced, sequential vs concurrent iRT | 20.3 mo (95% CI 13.3-NR) | 16.0 mo (95% CI 8.3-30.0) | HR 0.68 (0.47-0.99), P=.045 |
| Refractory, RT + ICI maintenance vs RT alone | 11.2 mo (95% CI 7.9-20.6) | 6.7 mo (95% CI 4.4-17.4) | P=.20 (ns) |
Randomized data on iRT sequencing in advanced NSCLC are limited (stated by authors). RT-before-ICI direction is consistent with the PACIFIC consolidation paradigm, but PACIFIC treated curative-intent unresectable stage III with concurrent chemoRT, a different population.
Observational: sequential vs concurrent not randomized, residual confounding by indication despite weighting. Small subgroups (155 newly-dx). Refractory comparison non-significant (P=.20).
Observational real-world cohort; sequential-vs-concurrent not randomized, confounding by indication despite propensity weighting. Small subgroups (155 newly-dx). Authors label it hypothesis-generating.
In newly-diagnosed advanced NSCLC starting immunoradiotherapy, this real-world signal supports separating RT from ICI in time rather than delivering them concurrently; it does not extend to refractory disease, where the RT-plus-ICI-maintenance benefit was not significant.
- Optimal RT-ICI sequencing (sequential vs concurrent) in advanced NSCLC active PD-1 Inhibitor and Chemotherapy With Concurrent Irradiation at Varied Tumour Sites in Advanced Non-small Cell Lung Cancer Phase 3n=327 · primary completion 2026-12 · phase 3 concurrent RT+PD-1 in stage IIIB/IV NSCLC
- Value of ICI maintenance after RT in refractory NSCLC
📚 Sources · 📄 1 paper
Abstract
ENZAMET + Decipher (Part 2)
FormHSPC on ADT + enzalutamide, Decipher genomic classifier available
TL;DRDecipher >0.85 predicts docetaxel OS benefit on an ADT+enza backbone (HR 0.75 vs 1.94, interaction p=0.04); ≤0.85 can skip docetaxel.
In mHSPC starting ADT + enzalutamide, a Decipher score >0.85 is where the docetaxel OS benefit concentrates while ≤0.85 sees little added benefit; the read informs docetaxel selection, not any radiotherapy decision.

| Treatment arm | Decipher >0.85 vs ≤0.85 OS HR | p |
|---|---|---|
| ADT + ENZA | 3.02 (1.50-5.76) | — |
| ADT + ENZA + Doce | 1.08 (0.60-1.71) | 0.73 |
+1 more figure

| Decipher stratum | Unweighted HR (doce vs none) | IPTW-weighted HR |
|---|---|---|
| ≤0.85 | 2.78 (1.49-5.21) | 1.94 (0.95-3.96) |
| >0.85 | 1.13 (0.71-1.79) | 0.75 (0.43-1.33) |
7 details
Preplanned biomarker analysis of the phase 3 ENZAMET RCT. Decipher genomic classifier (DPMC, cutpoint >0.85) applied to the ADT + enzalutamide backbone cohort, N=320.
Metastatic hormone-sensitive prostate cancer on an ADT + enzalutamide backbone with an available Decipher score. A low-volume subset was analysed separately.
ADT + enzalutamide ± early docetaxel. Docetaxel was given at investigator discretion (a stratification factor), so the docetaxel comparison is not randomised.
Two-part signal: Decipher >0.85 is prognostic for worse OS on ADT+enza, and by IPTW interaction (p=0.04) predicts OS benefit from added docetaxel; ≤0.85 derives little benefit. Effect sizes in the figures.
Consistent with docetaxel OS benefit in CHARTED and STAMPEDE for high-volume/high-risk mHSPC; positions Decipher as a molecular refinement of that selection. Presented as Level 1B evidence.
Docetaxel not randomised (IPTW-weighted, residual imbalance after scoring); the high-Decipher benefit's CI crosses 1 and rests on a subgroup interaction. Hypothesis-generating, not yet practice-defining.
Post-hoc biomarker-by-docetaxel interaction; docetaxel not randomised (IPTW-weighted, residual imbalance acknowledged). High-Decipher benefit CI crosses 1, rests on interaction p=0.04, strengthened only after weighting.
- Prospective validation of Decipher-guided docetaxel selection in mHSPC
- Whether DPMC ≤0.85 pts can safely omit docetaxel
- Decipher predictive value across other intensification agents (ARSI, PARP)
📚 Sources · 🐦 1 tweet
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 ENZAMET + Decipher | Part 2
Can genomics guide docetaxel intensification in mHSPC?
Outstanding presentation by @ChrisSweeney1.@OncoAlert@ASCO
After Part 1, the key question was:
➡️ Can a genomic classifier identify which patients with… pic.twitter.com/nJYMxuXelV
SPIN Score (Celiac Plexus SRS) NCT03323489
ForPancreatic cancer, intractable retroperitoneal pain, celiac SRS candidates
TL;DR89% pain response at SPIN 2 vs 32% at SPIN 0 for celiac SRS; post-hoc selection score, n=90.
Response is threshold-gated on baseline pain (>6 → 65.8%, rising to 85.7% at >8), and the strongest predictor was neurotoxic-chemo exposure (multivariate OR 5.1). The RT decision this moves is timing: refer for celiac SRS before neurotoxic agents. SRS dose/fractionation not reported in source (parent Lancet Oncol trial).
9 details
Post-hoc predictor analysis of the pivotal single-arm phase 2 celiac plexus SRS trial (NCT03323489, Lancet Oncol 2024). 90 evaluable pts; univariate/multivariate logistic regression with 500-iteration bootstrap internal validation.
Pancreatic-cancer pts with intractable retroperitoneal (celiac) cancer pain treated on the phase 2 SRS trial. Age and BMI were the prior-reported predictors; median baseline values not in source.
Celiac plexus radiosurgery, target D12-L2. Dose and fractionation not reported in source (specified in the parent Lancet Oncol trial), so transferability of the technique can't be judged here.
Pain response = ≥2-point reduction in average BPI-SF pain from baseline to 3 weeks. Score performance judged by optimism-corrected AUC.
Two independent predictors (severe baseline pain, no prior neurotoxic chemo) build a 0-2 score with a monotonic response gradient (see tables). Discrimination modest, AUC 0.714 corrected.
| SPIN score | Pain response | n |
|---|---|---|
| 0 | 32% | 31 |
| 1 | 53% | 40 |
| 2 | 89% | 19 |
| Predictor | Univariate OR | Multivariate OR |
|---|---|---|
| Neurotoxic chemo exposure | 5.33 (2.13-13.4), p<0.001 | 5.1, p=0.009 |
| Baseline pain intensity | 1.73, p=0.003 | 1.8, p=0.003 |
| Age | 1.06, p=0.014 | dropped (collinearity) |
| Therapy line | 0.65, p=0.04 | dropped (collinearity) |
Celiac plexus SRS is a novel non-invasive palliative option recently added to NCCN guidelines. This analysis converts the parent trial's flat response into an actionable selection score and argues for earlier use, before neurotoxic chemotherapy.
Post-hoc, single-arm data; predictors are associative. Internal bootstrap validation only (optimism-corrected AUC 0.714), external validation required. Subjective 3-week pain endpoint; score not prospectively tested.
Post-hoc predictor modeling of a single-arm phase 2; internal bootstrap validation only, external validation pending. Associations, not a prospectively validated selection tool.
In pancreatic-cancer pts with severe retroperitoneal pain and no prior neurotoxic chemo (SPIN 2), this supports earlier celiac plexus SRS, where 89% (n=19) achieved pain response; it does not extend to SPIN-0 pts, whose response was 32% (n=31).
- External validation of the SPIN score in an independent cohort
- Whether earlier SRS before neurotoxic chemo improves outcomes prospectively
- Durability of pain response beyond 3 weeks
📚 Sources · 🐦 1 tweet
Celiac SRS = convenient, effective tx for intractable pain, but who benefits most?
— Dr. Nina Niu Sanford (@NiuSanford) May 30, 2026
Post-hoc Ph2 analysis identified 2 response predictors (SPIN score): severe baseline pain & no prior neurotoxic chemo.
Supports earlier use before potential chemo neuropathy. #ASCO26 @OncoAlert pic.twitter.com/3qFYU6N1iD
SWOG S1007
ForHR+/HER2− breast, 1-3 nodes, Oncotype RS ≤25
TL;DR5y LRR 0.55% without RNI vs 0.85% with; IDFS unchanged by RNI (HR 1.03 premenopausal, 0.85 postmenopausal) in RS ≤25 N1 breast.
The RT read: RNI omission after breast conservation carries low locoregional risk, 5y LRR 0.55% without RNI vs 0.85% with, in RS ≤25 N1 disease. Chemo omission alone is not an RNI indication, so this supports withholding RNI in biologically favorable N1, pending randomized confirmation.
6 details 3 trials watching
Secondary analysis of SWOG S1007 (RxPONDER), a phase 3 RCT of chemo omission by 21-gene recurrence score. RNI receipt was prospectively recorded, not randomized. Median follow-up 6.1y; survival landmarked at 1y.
HR+/HER2−, Oncotype RS ≤25, 1-3 positive nodes. 4871 had RT forms; 81% received RT, and 59% of those with target data received RNI (targeting ≥ supraclavicular region).
RNI defined as targeting at least the supraclavicular region. The 59/41 split in RNI use reflects genuine practice equipoise in favorable N1 disease.
LRR was low across every locoregional approach; only mastectomy without RT reached 1.7%. IDFS did not differ by RNI in either menopausal group (see tables).
| Locoregional therapy | 5y cumulative LRR |
|---|---|
| BCS + RT + RNI | 0.85% |
| BCS + RT, no RNI | 0.55% |
| Mastectomy + PMRT | 0.11% |
| Mastectomy, no RT | 1.7% |
| Menopausal status | IDFS HR | 95% CI | p |
|---|---|---|---|
| Premenopausal | 1.03 | 0.74-1.43 | 0.87 |
| Postmenopausal | 0.85 | 0.68-1.07 | 0.16 |
Consistent with MA.20 / EORTC 22922, where RNI's benefit was concentrated in higher-risk node-positive disease. TAILOR RT (MA.39) is randomizing RNI in exactly this RS-low N1 population.
RNI comparison is non-randomized: confounding by indication (higher-risk pts selected for RNI) can mask a true RNI effect. Landmarking at 1y and diverse-setting RT reporting add noise.
RNI vs no-RNI comparison is non-randomized within RxPONDER; confounding by indication limits the null IDFS and low-LRR read. Randomized RNI trial (TAILOR RT) pending.
In HR+/HER2− breast with 1-3 positive nodes and Oncotype RS ≤25, this supports omitting regional nodal irradiation given low LRR; it does not extend to higher recurrence-score or >3 node disease.
- Randomized confirmation of RNI omission in favorable-risk N1 disease recruiting Evaluating Omitting of Internal Mammary Irradiation Among Early Stage Intermediate Risk (N1) Breast Cancer Phase NAn=214 · primary completion 2025-10 · genomic model omits IMN irradiation in N1recruiting The T-REX Trial: Tailored Regional External Beam Radiotherapy in Clinically Node-negative Breast Cancer Patients With 1-2 Sentinel Node Macrometastases. Phase NAn=1350 · primary completion 2028-12 · RCT omitting regional RT, 1-2 macromets, ER+/HER2-recruiting RecurIndex Guided Avoidance of Regional Nodal Irradiation for Node Positive Breast Cancer Phase NAn=540 · primary completion 2029-08 · RecurIndex-guided RNI avoidance in N1 low-risk
- Durability of low LRR beyond 6 years without RNI
📚 Sources · 📄 1 paper
Abstract
Proton vs Photon PMRT Capsular Contracture
ForPostmastectomy implant-based reconstruction (TE/I or DTI) receiving PMRT
TL;DRProton PMRT trended toward higher capsular contracture vs IMRT photon (univariate HR 2.3; MVA HR 1.76 ns); proton+DTI worst, 50% 2yr CC.
The interaction is the read: DTI reconstruction, not modality, dominates CC risk (HR 3.0), and proton+DTI stacks to 50% 2yr CC vs 12% for photon+TE/I. When proton is chosen for cardiac/pulmonary sparing, reconstruction choice (favor TE/I over DTI) is the modifiable lever.
8 details 2 trials watching
Retrospective, IRB-approved, 2 centers within one institution, Jan 2017 to Dec 2023. N=175 (89 proton, 86 photon). CC estimated by Kaplan-Meier; Cox proportional hazards for HRs, logistic regression to verify. Median follow-up 42 mo (proton), 47 mo (photon).
Breast cancer pts with subpectoral 2-stage tissue expander/implant (TE/I) or direct-to-implant (DTI) reconstruction receiving PMRT. Median age 49 (24-78); 63% Hispanic. All TE/I pts had the expander irradiated. Groups imbalanced on laterality (P<.001) and reconstruction type (P<.001).
PBS proton vs IMRT photon PMRT. Dose and fractionation not reported in source. In TE/I, the tissue expander itself was the irradiated target.
Proton vs photon CC: univariate HR 2.3 (1.26-4.30, P=.007), attenuating to HR 1.76 (0.93-3.32, P=.083, ns) on multivariable. DTI vs TE/I: HR 3.0 (1.7-5.5, P<.001), the dominant driver. Per-group 2yr CC rates in the table.
| Modality + reconstruction | n | 2-yr CC rate |
|---|---|---|
| Proton + DTI | 36 | 50% |
| Photon + DTI | 15 | 35% |
| Proton + TE/I | 53 | 23% |
| Photon + TE/I | 71 | 12% |
Prior proton PMRT evidence centered on improved cardiac and pulmonary dosimetry; head-to-head capsular-contracture data proton vs photon were scarce. This is the largest proton reconstruction cohort reported to date.
Retrospective, single-institution, N=175, with groups imbalanced on reconstruction type and laterality. The proton effect lost significance after adjustment (P=.083), so residual confounding (reconstruction type driving both proton selection and CC) cannot be excluded.
The modifiable variable is reconstruction, not beam: DTI carries roughly 3x the CC hazard, and proton stacked on DTI reaches 50% 2yr CC. Where proton is chosen for heart or lung sparing, staged TE/I may blunt the CC penalty; a prospective comparison is needed to confirm.
Retrospective single-institution cohort; groups imbalanced on reconstruction type and laterality; proton effect lost significance on multivariable (HR 1.76, P=.083). Signal, not confirmation.
In a postmastectomy pt weighing DTI vs staged TE/I reconstruction who will receive proton PMRT, the CC signal is concentrated in DTI (proton+DTI 50% vs proton+TE/I 23% 2yr); it does not resolve proton vs photon overall, which was ns on multivariable.
- Prospective proton vs photon PMRT capsular contracture comparison
- Whether staged TE/I reconstruction mitigates proton capsular contracture risk n=300 · primary completion 2023-08 · 2-stage expander/implant, capsular contracture EPrecruiting Breast Reconstruction and Radiotherapyn=750 · primary completion 2027-08 · recon timing + type vs RT complication risk
- Mechanism: proton dose distribution vs selection bias driving contracture
📚 Sources · 📄 2 papers
Abstract
NRG/RTOG 9804 + E5194 Combined Analysis
ForGood-risk DCIS (low/int grade, ≤2.5cm, ≥3mm margins), lumpectomy without RT
TL;DR15-yr IBR 11.4% vs 19.0% with vs without tamoxifen in RT-omitted good-risk DCIS; MVA HR 0.54, invasive-IBR HR 0.43.
Tamoxifen's benefit here concentrates on invasive IBR (HR 0.43, p=0.0042), not DCIS-IBR (p=0.089), offsetting the recurrences that carry survival weight. But 15-yr IBR stays 11.4% even with tamoxifen, and no arm tests RT, so this informs the omit-RT-plus-endocrine path, not RT vs tamoxifen.
7 details 4 trials watching
Ancillary exploratory analysis pooling the non-RT arm of NRG/RTOG 9804 with the good-risk cohort of ECOG-ACRIN E5194. N=878 (317 + 561), median follow-up 14.85 yr.
Good-risk DCIS: low or intermediate grade, ≤2.5 cm, margins ≥3 mm, lumpectomy without RT. Median age 59. Tamoxifen users skewed toward negative re-excision and pathologic size ≤5 mm.
Tamoxifen optional and non-randomized, used by 43.1% overall (65.6% in 9804, 30.3% in E5194).
No RT in either cohort by design; this characterizes the RT-omitted good-risk population, not an RT comparison.
IBR overall, invasive IBR, DCIS-IBR, contralateral breast event, OS. Fine-Gray competing-risk models, univariate plus multivariable.
NSABP B-24 randomized tamoxifen after lumpectomy plus RT and cut breast events; this extends the tamoxifen signal to the RT-omitted good-risk setting, though non-randomized.
Tamoxifen not randomized; users differed on prognostic factors (re-excision, size), so residual confounding is likely. Exploratory combined dataset, not a prespecified endpoint.
| Endpoint | HR (95% CI) | p |
|---|---|---|
| Any IBR | 0.54 (0.35-0.83) | 0.0045 |
| Invasive IBR | 0.43 (0.24-0.77) | 0.0042 |
| Group | 15-yr IBR (95% CI) |
|---|---|
| Tamoxifen | 11.4% (7.9-15.5) |
| No tamoxifen | 19.0% (15.3-22.9) |
Non-randomized optional tamoxifen compared within a post-hoc combined dataset; users differed on prognostic factors. Consistent with randomized NSABP B-24 signal but confounded here.
For good-risk DCIS where RT is already being omitted, this supports endocrine therapy to reduce invasive IBR; it does not test whether tamoxifen substitutes for RT.
- Whether endocrine therapy can substitute for RT in good-risk DCIS not yet Assessment of Biosignature Classification of DCIS for RadioTherapy Benefit Post Lumpectomy (ABCD RT) Phase 3n=5270 · primary completion 2039-07 · phase 3 RT omission in biosignature-low DCIS
- Aromatase inhibitor vs tamoxifen in RT-omitted good-risk DCIS recruiting DCIS: RECAST Trial Ductal Carcinoma In Situ: Re-Evaluating Conditions for Active Surveillance Suitability as Treatment Phase 2n=400 · primary completion 2028-11 · DCIS trial with tamoxifen vs AI arms
- Which good-risk DCIS pts can omit both RT and endocrine therapy active Comparing an Operation to Monitoring, With or Without Endocrine Therapy (COMET) Trial For Low Risk DCIS Phase NAn=997 · primary completion 2024-06 · active monitoring vs surgery, low-risk DCISn=2500 · primary completion 2034-02 · active surveillance vs standard, low-risk DCIS
📚 Sources · 📄 1 paper
Abstract
OPERA Trial (5-year)
ForRectal cancer, post-neoadjuvant therapy
TL;DR76% achieved a good clinical response at W14 (DRE+rectoscopy); nCR matched cCR for 5yr organ preservation (77% vs 81%), enabling early W&W selection.
nCR carries the same 5yr organ-preservation prognosis as cCR (77% vs 81%) and reflects RT-related mucosal change, not residual tumor, so an nCR at reassessment shouldn't route a patient to salvage TME. Early W14 clinical exam (DRE+rectoscopy) matched MRI TRG1-2 in 98%, letting W&W selection move up from W24.
8 details 3 trials watching
Post-hoc analysis of the randomised OPERA trial, N=141 evaluable. Tests an earlier response timepoint (W14, ~1 mo after NAT end) against the protocol W24 triad, scoring clinical tumor response (CTRE) by DRE + rectoscopy as cCR / nCR / PR.
OPERA randomised the boost after neoadjuvant chemoradiotherapy (EBRT boost vs contact X-ray brachytherapy boost); these slides don't label which arm is which. The higher early good-response rate in one arm did not translate to a 5yr organ-preservation difference (see table).
Post-hoc, non-randomised comparison of response groups; W14 selection not prospectively validated against the protocol W24 assessment. Single-trial, modest N; 5yr OP differences underpowered (p=0.24).
Authors' RT-relevant read: nCR reflects radiation change, not residual tumor, and matches cCR for organ preservation (77% vs 81%), so an nCR should not trigger salvage TME. Early DRE + rectoscopy can move W&W selection up to W14 with MRI confirmation.
| Endpoint | Arm A | Arm B | p |
|---|---|---|---|
| W14 good response (cCR+nCR) | 65% | 88% | 0.004 |
| 5yr organ preservation | 75% | 83% | 0.24 |
Post-hoc analysis of an alternate (W14 vs protocol W24) timepoint; response-group comparison non-randomised and not prospectively validated for W&W selection.
In a rectal-cancer pt with a near-complete clinical response after chemoradiotherapy, this supports continued watch-and-wait over radical TME; the 24% with only a partial response stay surgical candidates and aren't covered.
- Prospective validation of W14 vs W24 response assessment for W&W selection active Short RT Versus RCT,Followed by Chemo.and Organ Preservation for Interm and High-risk Rectal Cancer Patients Phase 3n=702 · primary completion 2023-09 · candidate match
- Optimal RT boost technique to maximise early complete clinical response active Short RT Versus RCT,Followed by Chemo.and Organ Preservation for Interm and High-risk Rectal Cancer Patients Phase 3n=702 · primary completion 2023-09 · candidate match
- Long-term regrowth risk in nCR pts managed by watch-and-wait recruiting Organ Preservation First Strategy and Intentional Watch and Wait for MRI Defined Low-risk Rectal Cancer Phase NAn=96 · primary completion 2025-09 · candidate match
📚 Sources · 🐦 1 tweet
Day FOUR of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 18, 2026
Five-year Results of the OPERA Trial: When and How to Assess Tumor Response to Guide Rectal Preservation Presented by Syrine Ben Dhia 🇫🇷 #RadOnc ☢️
This post-hoc analysis of the OPERA trial evaluated early tumor response… pic.twitter.com/KUanFTxeFh
RADIOSA (MFS post-hoc)
ForOligorecurrent prostate cancer eligible for metastasis-directed SBRT
TL;DRPost-hoc MFS 16.6mo vs not reached, HR 0.39 favoring SBRT + 6mo ADT over SBRT alone in oligorecurrent prostate.
The additive read is the eugonadal MFS: benefit persisted after testosterone recovery (p<0.05), so the ADT effect is not just on-treatment suppression of imaging progression. That argues against reading RADIOSA's MFS split as a testosterone artifact, and moves the SBRT-alone vs SBRT + short-course ADT decision in oligorecurrence.
Also covered Jun 12

| Endpoint | Arm A (SBRT) | Arm B (SBRT + ADT) | Effect size |
|---|---|---|---|
| Metastatic progression | 32/51 (62.7%) | 19/51 (37.3%) | log-rank p=0.00079 |
| Median MFS | 16.6 mo (95% CI 12.83-NA) | not reached | HR 0.3894 (0.2201-0.6888), p=0.00119 |
+1 more figure

8 details 5 trials watching
Phase II randomized trial, 1:1, N=102, Arm A SBRT alone vs Arm B SBRT + 6-month ADT. Median follow-up (reverse KM) 49.23 months (95% CI 42.47-54.8). This report is a post-hoc analysis of MFS and eugonadal MFS.
Oligorecurrent prostate cancer. Detailed eligibility (number of lesions, imaging modality, prior local therapy, PSA thresholds) not reported in source.
SBRT to the oligorecurrent sites in both arms. Dose, fractionation, and target volume are not reported in source, which limits transfer to a specific practice.
MFS defined as randomisation to any M1 metastatic recurrence on imaging. Eugonadal MFS measured from testosterone recovery to new metastasis or last follow-up. KM curves compared by log-rank; HRs from Cox models.
Effect sizes are in the figure caption table. All Arm B pts except two reached testosterone recovery within follow-up.
Post-hoc analysis; MFS was not the prespecified primary endpoint. No OS reported in source, so the surrogate carries the read. Toxicity and SBRT technique parameters absent from source.
The eugonadal analysis is the substantive contribution: separating the benefit from on-treatment castration addresses the standing objection that ADT simply delays imaging-detected progression. Whether that reflects durable synergy between ablation and transient androgen suppression, as the authors argue, is hypothesis-generating at N=102.
Post-hoc endpoint analysis of a phase II trial; MFS was not the prespecified primary. Design dominates the read despite the clean randomisation and mature follow-up.
In oligorecurrent prostate cancer being considered for metastasis-directed SBRT, this supports the discussion of adding 6-month ADT over SBRT alone; it does not address de novo metastatic or castration-resistant disease, and the SBRT dose and target volume are not stated in the source.
- Does the MFS advantage translate to overall survival active Prostate-cancer Treatment Using Stereotactic Radiotherapy for Oligometastases Ablation in Hormone-sensitive Patients Phase 3n=550 · primary completion 2026-06 · phase 3 SBRT to all mets in hormone-sensitive M1
- Optimal ADT duration alongside metastasis-directed SBRT n=873 · primary completion 2027-04 · randomises 1mo vs 6mo ADT + ARTA on top of MDTrecruiting Duration of Androgen Receptor Pathway Inhibitor and ADT With Metastasis Directed Therapy in Oligometastatic Cancer of the Prostate (DIRECT) Phase 2n=132 · primary completion 2031-02 · ADT/ARPI duration arm: 8-9mo abiraterone added to SBRT
- Whether PSMA-PET staging changes the size of the benefit recruiting Veterans Affairs Seamless Phase II/III Randomized Trial of STAndard Systemic theRapy With or Without PET-directed Local Therapy for Oligometastatic pRosTate Cancer Phase 2/3n=464 · primary completion 2026-09 · randomises PET-directed local therapy vs systemic alonerecruiting Metastasis Directed Stereotactic Body Radiotherapy for Oligo Metastatic Hormone Sensitive Prostate Cancer Phase NAn=118 · primary completion 2031-12 · MD-SBRT randomised in PSMA-PET-defined 1-3 mets
📚 Sources · 🐦 1 tweet
Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 16, 2026
Post-hoc analysis of metastasis-free survival (MFS) and Eugonadal MFS in the RADIOSA phase II randomized trial Presented by Giulia Marvaso 🇮🇹 #RadOnc ☢️ @giuliamarvaso84
Post-hoc analysis of RADIOSA shows SBRT plus short-term ADT… pic.twitter.com/1zpiChkUgA
Tumour bed boost after BCS + WBRT
ForPost-BCS invasive breast cancer treated with WBRT, Dutch cohort 2012-2016
TL;DR10-yr IBTR 1.2% no-boost vs 1.2% boost in 0-2 risk factors; boost omission viable in modern systemic era.
The boost arm carries HIGHER crude IBTR at every stratum (10-yr 3.3% vs 2.7% at ≥3 RF), which is confounding by indication, not harm, and it means these data cannot estimate boost efficacy at all. What they do support is a floor: with 0-2 risk factors, 10-yr IBTR is 1.2% either way, so the omission decision rests on that absolute rate.

| Risk factors | N no boost | N boost | 5-yr no boost | 5-yr boost | 10-yr no boost | 10-yr boost |
|---|---|---|---|---|---|---|
| 0-2 | 15,085 | 13,845 | 0.6% | 0.7% | 1.2% | 1.2% |
| ≥ 3 | 149 | 733 | 1.3% | 2.9% | 2.7% | 3.3% |
| Uncertain | 592 | 944 | 0.8% | 3.3% | 1.4% | 3.6% |
+2 more figures


9 details
Dutch population-based cohort (DBRT / Netherlands Cancer Registry linkage) of breast-conserving treatment, 2012-2016. Non-randomised: boost use reflects clinician risk assessment, not allocation.
Breast conserving treatment with or without an RT boost. Strata by number of risk factors: 0-2 (15,085 no boost / 13,845 boost), ≥3 (149 / 733), uncertain (592 / 944).
Whole-breast RT with or without tumour bed boost. No dose, fractionation, boost technique, or target-volume detail reported in source.
Primary: ipsilateral breast tumour recurrence (IBTR), histologically confirmed via a pathology-report text/code algorithm. Cumulative incidence reported at 5 and 10 years by risk-factor count.
Low IBTR across every subgroup. Only the ≥3 risk-factor boost group crossed an Assisi threshold at 10 years (3.3%, vs the <3% bar).
EORTC 22881-10882 anchored the ~50% relative IBTR reduction from boost. Absolute IBTR here is an order of magnitude below that trial's era, which is the authors' argument that a relative halving now buys little absolute benefit.
Confounding by indication is the dominant issue: higher-risk pts got the boost, so crude boost-arm rates run higher. The ≥3 RF no-boost cell is 149 pts. 10-yr estimates on a 2012-2016 cohort are projected, and IBTR ascertainment was algorithmic.
Registry cohort with non-random boost allocation; confounding by indication and a 149-pt no-boost ≥3 RF stratum undercut the omission claim.
In post-BCS pts with 0-2 of the listed risk factors receiving WBRT, this supports discussing boost omission on absolute-risk grounds; it does not inform pts with ≥3 risk factors, where the ≥3 RF no-boost stratum is only 149 pts.
- Which ≥3 risk-factor subgroups actually gain from a boost
- Does boost omission hold with longer observed follow-up
- Boost value in pts with residual disease after neoadjuvant therapy
📚 Sources · 🐦 1 tweet
Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 16, 2026
Is a boost to the tumour bed still indicated after breast-conserving surgery and whole-breast radiotherapy in the era of modern systemic therapy? Presented by Femke Froklage 🇳🇱 #RadOnc ☢️
We aimed to identify a subgroup of breast… pic.twitter.com/RqK5r9XPqW