Combined
ARS Appropriate Use Criteria for Locoregionally Recurrent Rectal Cancer
TL;DRGuideline update, 116 studies: margin-negative (R0) resection determines survival; preop systemic ± RT/reirradiation enables downsizing, no major practice change.
Reirradiation and preop (chemo)RT are framed as R0-enabling downsizing tools in the previously-irradiated pelvis, not definitive therapy: the guideline holds that margin-negative resection, not RT dose or intensity, is the survival and local-control lever. Moves the reirradiate-to-downstage-before-salvage-surgery decision.
8 details 5 trials watching
- 🔍 Systematic review with RAND/UCLA modified Delphi consensus; PICOTS + PRISMA; 116 references, Jan 2013-Jul 2025
- 🔍 Evidence base skews retrospective (116 refs total)
- 10 well-designed (phase 2 randomized / phase 3)
- 29 moderately designed (matched cohort / phase 2)
- 76 retrospective (design limitations)
- 1 meta-analysis
- 💊 Preop systemic therapy, RT, or both facilitate tumor downsizing → improve likelihood of R0 resection
- 🔍 Five PICO questions: surgery, preop/periop therapy, nonoperative management, RT/reirradiation, systemic therapy
- 🔍 High-res pelvic MRI preferred to map resectability (sidewall, sacral, nerve involvement)
- 🔍 FDG-PET/CT separates postoperative fibrosis from active recurrent tumor
- 📊 Margin-negative (R0) resection is the ultimate determinant of survival and local control
- ⚠️ Updates 2012 ACR AUC; does not suggest major practice change, reaffirms combined-modality therapy
- Optimal reirradiation dose and technique for previously-irradiated LRRC recruiting Pencil Beam Proton Therapy for Pelvic Recurrences in Rectal Cancer Patients Previously Treated With Radiotherapy Phase 2n=65 · primary completion 2025-10 · proton reirradiation for previously-RT rectal recurn=31 · primary completion 2025-12 · carbon-ion reirradiation, unresectable LRRC
- Role of ctDNA in detecting and monitoring LRRC n=800 · primary completion 2026-06 · ctDNA methylation for postop CRC recurrence monitoringrecruiting RESPONSE: Colorectal Cancer Survivors' Follow-up Care - Now Digital and Need-based Phase NAn=400 · primary completion 2028-03 · ctDNA recurrence surveillance in CRC follow-up
- Role of immunotherapy in LRRC management n=31 · primary completion 2026-11 · SBRT + PD-1 in unresectable LRRC
📚 Sources · 📄 1 paper
Abstract
INDIBLADE
ForStage II/III MIBC, cT2-4aN0-2, bladder-preservation candidates
TL;DR2yr bladder-intact EFS 78% (67-90%) with induction ipi+nivo before chemoRT; 2yr OS 96% in cT2-4aN0-2 MIBC.
Cohort spans cT2-4a and clinically node-positive (N1-2), pushing bladder preservation into nodal disease that usually routes to cystectomy. The novel lever is induction ipi+nivo before chemoradiation, not the RT itself; 78% 2yr bladder-intact EFS tests whether induction dual-IO belongs in a trimodality pathway. RT dose and fractionation absent from source, so transferability stays unconfirmed.
7 details 4 trials watching
Single-arm bladder-preservation trial: induction dual checkpoint blockade followed by chemoradiation. N and site count not reported in source. Outcomes reported at 2 years.
Stage II/III MIBC, cT2-4aN0-2. Notably includes clinically node-positive (N1-2) disease, a group usually routed to radical cystectomy.
Induction ipilimumab + nivolumab (dual IO) before chemoradiation. Doses, cycles, and radiosensitizing chemotherapy not stated in source.
Chemoradiation is the definitive local component, but RT dose, fractionation, and target volume are not specified in source, gating whether the result transfers to a given practice.
Headline readout is 2yr bladder-intact event-free survival; overall survival reported alongside.
Single-arm, no comparator vs chemoRT alone or cystectomy; short 2yr follow-up; bladder-intact EFS is a composite surrogate; N and RT details absent from source.
Single-arm, no comparator vs chemoRT alone or cystectomy; 2yr follow-up; bladder-intact EFS a composite surrogate. Hypothesis-generating induction-IO-plus-CRT signal, not yet mature.
In cT2-4aN0-2 MIBC weighing bladder preservation against radical cystectomy, this signals induction ipi+nivo plus chemoradiation is feasible even with node-positive disease, but single-arm 2yr data do not yet displace cystectomy or chemoRT alone off-protocol.
- Does induction ipi+nivo improve bladder-intact EFS vs chemoRT alone? n=50 · primary completion 2024-07 · MMC/cape chemoRT + nivo±ipi, nivo-mono comparator armn=50 · primary completion 2025-09 · induction ipi+nivo → chemoRT, cT2-4aN0-2 bladder-sparing
- Durability of bladder preservation beyond 2 years n=30 · primary completion 2027-06 · long-term bladder-preservation outcomes post-NAT TMT
- Does bladder preservation extend to node-positive (N1-2) MIBC? n=11 · primary completion 2026-02 · chemoRT ± durvalumab, node-positive bladder cancer
📚 Sources · 🐦 1 tweet
‼️ INDIBLADE: stage II/III (cT2-4aN0-2) MIBC -> induction ipilimumab plus nivolumab -> CRT
— NonsparseOncologist (@5_utr) June 17, 2026
2-year bladder-intact event-free survival is 78% (0.67−0.9) 🤩
2-year overall survival was 96% (0.91−1)
Lots of bladders can be potentially spared!https://t.co/LzTe72GYHD
KEYNOTE-689 vs NIVOPOSTOP
TL;DRRound-up of two positive phase 3 IO trials in resectable LA-HNSCC: perioperative pembro and post-op nivo added to adjuvant CRT.
KEYNOTE-689NIVOPOSTOP
Neither trial changes the RT prescription: both keep standard adjuvant cisplatin-CRT. What moves for the radonc reader is IO placement around that RT course, neoadjuvant pembro before surgery (KEYNOTE-689) versus nivo added to postop CRT (NIVOPOSTOP, 3-yr DFS ~63% vs 53%). The role is integrating IO into unchanged local therapy, not re-planning it.
- KEYNOTE-689 = first positive perioperative IO trial in resectable HNSCC in >2 decades (per source)
5 details 2 trials watching
- 🔍 Both retain standard adjuvant cisplatin-based (chemo)RT; IO is added, RT dose/fractionation/target volume unchanged
- 💊 KEYNOTE-689: 2 cycles neoadjuvant pembro → surgery → risk-adapted adjuvant RT/CRT + pembro → maintenance pembro
- 📊 KEYNOTE-689 vs NIVOPOSTOP at a glance
Feature KEYNOTE-689 NIVOPOSTOP Drug Pembrolizumab Nivolumab IO timing Perioperative (neoadj + adj) Postoperative only Population Resectable stage III-IVA High-risk resected (ENE/margin+) Control arm Surgery → adj RT + cisplatin Postop cisplatin CRT Primary EP EFS DFS Result Positive EFS (no value in source) 3-yr DFS ~63% vs 53% - 📊 NIVOPOSTOP high-risk criteria for postop CRT + nivo
- Positive margins
- Extranodal extension (ENE)
- ≥4 involved nodes
- Extensive perineural invasion
- ⚠️ Educational round-up, not primary data; KEYNOTE-689 EFS magnitude not reported in source; NIVOPOSTOP is ASCO 2025 abstract-level
In resectable stage III-IVA LA-HNSCC these inform two settings: perioperative pembro for newly-diagnosed resectable disease (KEYNOTE-689), and nivo on postop cisplatin-CRT for high-risk resected pts with extranodal extension or positive margins (NIVOPOSTOP); the RT backbone is unchanged in both.
- Optimal IO sequencing: perioperative vs purely postoperative recruiting Sintilimab Plus Chemotherapy as Neoadjuvant and Adjuvant Treatment for Locally Advanced Oral Squamous Cell Carcinoma Phase 3n=104 · primary completion 2030-12 · phase 3 perioperative chemo-IO in resected oral SCC
- Which PD-L1/CPS threshold selects benefit
- Can adjuvant CRT be de-escalated when IO is added n=20 · primary completion 2026-09 · de-escalated RT after induction chemo+pembro, LAHNSCC
📚 Sources · 🐦 1 tweet
🧠 High-yield: KEYNOTE-689 vs NIVOPOSTOP
— Dr Rupam Manna MD (@DrRupamOncology) June 15, 2026
These two trials are redefining standards for resectable LA-HNSCC.
1/ KEYNOTE-689 (NEJM 2025)
Perioperative pembro → significant EFS benefit
First positive perioperative IO trial in >2 decades
2/ NIVOPOSTOP (ASCO 2025)
Post-op nivo +… pic.twitter.com/1mRQr9jmVX
RADIOSA NCT03940235
ForMetachronous oligorecurrent HSPC, ≤3 lesions, post-radical local tx
TL;DRmcPFS 32.2 vs 15.1mo, HR 0.43 (0.26-0.72), p=0.001 adding 6mo ADT to metastasis-directed SBRT in oligorecurrent HSPC.
Surfaced from a review's discussed trials
Both arms get ablative SBRT (30 Gy/3fx, BED >100 Gy) to all sites, so the trial isolates the 6-mo ADT add-on, not SBRT's own contribution (no observation arm). The decision it moves: whether to layer short ADT onto metastasis-directed SBRT. SBRT alone still gave 15.1-mo cPFS in selected pts.
Also covered May 17
8 details 2 trials watching
Single-centre, randomised, open-label phase 2 (European Institute of Oncology, Milan). N=105 randomised 1:1 (52 SBRT alone, 53 SBRT+ADT); modified ITT, 51/arm analysed. Median follow-up 31 mo.
Metachronous oligorecurrent hormone-sensitive prostate cancer after radical local treatment; ≤3 lesions (pelvic/extra-regional nodal or bone) on PSMA-PET or MRI; ECOG 0-1; median age 70. Stratified by PSMA-DT (≤3 vs >3 mo), site (node vs bone), imaging.
SBRT 30 Gy in 3 fractions every other day (EQD2 98.6 Gy at α/β 1.5, BED >100 Gy), or equivalent by site. All oligometastatic sites treated in both arms.
The SBRT+ADT arm added 6 months of LHRH-analogue ADT starting within 1 week before SBRT.
Primary: clinical progression-free survival. OS and time-to-CRPC were not the primary read.
Adding short ADT roughly doubled median cPFS; effect sizes in the results table.
Near-absent RT toxicity: 1 G1 GI, 1 G3 GU (left ureter stenosis, SBRT+ADT), no late effects. ADT added 22 G1 AEs, all resolved. No treatment-related deaths.
First RCT of adding short ADT to MDT in metachronous oligorecurrent HSPC. STOMP/ORIOLE established MDT vs observation; RADIOSA instead isolates the ADT add-on onto an SBRT backbone.
Single-centre, open-label, N=105. Primary endpoint is clinical PFS, a surrogate; ADT's own progression-delaying effect confounds the SBRT+ADT arm. Optimal ADT duration untested.
Single-centre open-label phase 2, N=105; 1° EP is clinical PFS (surrogate), not OS. Consistent with STOMP/ORIOLE MDT signals; not definitive enough to change practice.
In metachronous oligorecurrent hormone-sensitive prostate cancer with ≤3 lesions on PSMA-PET, this supports adding 6 mo ADT to metastasis-directed SBRT for longer cPFS; it does not address synchronous or polymetastatic disease, and SBRT alone remains reasonable in carefully selected pts.
- Optimal duration of ADT added to SBRT active Androgen Deprivation Therapy for Oligo-recurrent Prostate Cancer in Addition to radioTherapy Phase 3n=280 · primary completion 2027-10 · phase 3 ADT added to MDRT vs MDRT alonen=532 · primary completion 2031-02 · tests timing of ADT+ARPI added to SBRT in mHSPC
- Biomarkers predicting benefit from SBRT alone
- Whether cPFS gain translates to OS or delayed CRPC
📚 Sources · 📄 1 paper
Abstract
Concurrent Systemic Therapy + Radiation Timing (Speers)
TL;DRTraffic-light framework for what runs concurrent with breast/CW + RNI RT vs hold: continue endocrine + trastuzumab/pertuzumab, caution T-DXd/CDK4/6i, hold cytotoxics/PARPi.
HERANCCTG N9831APHINITYKATHERINEATEMPTDESTINY-Breast05COMBARTKEYNOTE-522
The actionable RT read: in the DESTINY-Breast05 arm, T-DXd ILD was 10.7% sequential vs 9.6% concurrent, so timing around RT did not change ILD, and concurrency is reasonable with lung-dose limits. The 'do not ignore' signal is T-DM1 plus CNS SRS radionecrosis; hold CDK4/6i for large fields.

+1 more figure

7 details 3 trials watching
ASCO 2026 educational review / Educational Book chapter (Wong, Speers, Schaverien, Table 5). Sorts systemic agents into a continue / caution / hold framework for concurrency with breast/chest-wall + RNI RT. Evidence base is mostly retrospective, post-hoc, or small prospective series.
Context is adjuvant breast/CW + regional nodal irradiation. Plan features that raise the concurrency stakes: large lung volumes, IMN coverage, bolus, reconstruction, and CNS SRS (T-DM1 radionecrosis, T-DXd ILD).
Endocrine therapy and trastuzumab/pertuzumab are safe concurrent; T-DXd and CDK4/6i are plan-dependent; cytotoxics, veliparib, and capecitabine sequence. Default outside protocol is PK-based washout, then RT, then resume.
| Agent class | With RT | Notes / evidence |
|---|---|---|
| Endocrine therapy | Continue | minimal radiosensitization |
| Trastuzumab ± pertuzumab | Continue | concurrent standard (HERA, NCCTG N9831, APHINITY) |
| T-DM1 | Continue | per KATHERINE / ATEMPT; watch dermatitis, pneumonitis, CNS SRS necrosis |
| T-DXd | Caution | ILD dominant; sequence/hold for high lung-dose or active pulmonary disease |
| Pembrolizumab | Continue, monitor | KEYNOTE-522 concurrent tolerated; pneumonitis vigilance |
| CDK4/6i (palbo/ribo/abema) | Hold large fields | mostly retrospective; concurrent only in protocol |
| Olaparib | Sequence | complete RT 2-12 wks before; RadioPARP suggests concurrent safety |
| Veliparib / talazoparib | Avoid concurrent | veliparib severe acute/late tox (TBCRC 024) |
| Capecitabine | Hold / sequence | adjuvant paradigm sequential (CREATE-X) |
| Cytotoxics (anthracycline/taxane/platinum) | Hold | sequence, do not give concurrently |
| Metric | Value |
|---|---|
| ILD, T-DXd 5.4 mg/kg (PI) | ~12%; fatal ~0.9% |
| DESTINY-Breast05 ILD | 9.6% T-DXd vs 1.6% T-DM1 |
| RT timing (T-DXd arm) | 10.7% seq vs 9.6% concurrent, no effect |
| COMBART concurrent RT/SRT | 40 pts; acute tox 20% |
For a HER2+ patient on adjuvant trastuzumab/pertuzumab or T-DM1 needing chest-wall + nodal RT, this supports running HER2 therapy through RT with pneumonitis and CNS-SRS vigilance; it does not extend to concurrent cytotoxics, veliparib, or CDK4/6i in large fields.
- Concurrent CDK4/6 inhibitor safety with regional nodal RT recruiting Safety Assessment of Concurrent Radiotherapy and Novel Systemic Therapy for Breast Cancer Phase NAn=148 · primary completion 2026-01 · concurrent nodal RT + CDK4/6i tolerabilityn=15 · primary completion 2026-09 · preop RT + abemaciclib phase 1b safety
- Optimal T-DXd sequencing around thoracic RT to limit ILD
- Concurrent olaparib with RT in early-stage breast active Radiation Therapy With or Without Olaparib in Treating Patients With Inflammatory Breast Cancer Phase 2n=300 · primary completion 2027-06 · phase 2 RT ± olaparib in non-met breast
📚 Sources · 🐦 1 tweet
#ASCO26
— Yakup Ergün (@dr_yakupergun) June 1, 2026
Which treatments should continue with RT, and which should be held?
From the Great presentation by Dr. Corey W. Speers pic.twitter.com/9B7e0HePDZ
mRCAT-III NCT06507371
ForpMMR/MSS LARC, cT3-4N0/+, tumor ≤10cm from verge, no lateral node
61.0% vs 28.6%
P<0.0001, ITT, blinded central review
TL;DRpCR 61.0% vs 28.6% (P<0.0001) with node-sparing SCRT + tislelizumab + CAPOX vs conventional SCRT + CAPOX in pMMR LARC.
The RT read is a confound, not a green light for nodal omission: the experimental arm changed two things at once, tumor-bed-only targeting AND added tislelizumab, so node-sparing's own contribution to the pCR doubling (61.0% vs 28.6%) can't be isolated. Node-sparing plausibly drove the lower severe-GI toxicity, but this doesn't yet license dropping elective nodal RT.

| Endpoint | Experimental | Control | P |
|---|---|---|---|
| pCR (ITT) | 61.0% (47/77) | 28.6% (22/77) | <0.0001 |
| MPR (TRG0+1) | 77.9% (60/77) | 50.6% (39/77) | <0.0001 |
+1 more figure

6 details 5 trials watching
Open-label, multicenter phase 3 RCT across 17 China hospitals; randomized 1:1, 77 pts per arm, stratified by clinical N stage (cN0 vs cN+). Primary pCR read by blinded independent central review.
pMMR/MSS rectal adenocarcinoma, cT3-4N0/+M0, tumor lower edge ≤10cm from the anal verge, ECOG 0-1, age 18-75, no positive lateral pelvic node.
Both arms CAPOX (oxaliplatin 130mg/m² d1, capecitabine 1000mg/m² d1-14). Experimental adds tislelizumab 200mg d1; control is chemo + RT only.
Both arms short-course 5Gy×5. Experimental is node-sparing (tumor bed only, spares tumor-draining nodes); control is conventional elective-nodal coverage. This target-volume contrast is the RT question.
Primary: pCR (ITT). Secondary: MPR, TRG, organ-preservation rate, EFS, OS, AEs.
Primary pCR and secondary MPR both favored the experimental arm (see figure); EFS, OS, organ-preservation not reported in source.
Experimental arm reported fewer severe GI AEs (author takeaway), plausibly from the smaller node-sparing volume; numeric AE rates not in source.
Control pCR 28.6% matches short-course RT + consolidation chemo benchmarks (RAPIDO ~28%). The novelty is a PD-1 benefit in an MSS population usually IO-refractory, with nodal-RT omission as the immunologic rationale.
Open-label; pCR is a surrogate with EFS/OS immature; the experimental arm confounds node-sparing target volume with added tislelizumab, so the RT-attributable effect can't be isolated; N=154, single country.
Divergent MSS-rectal result from a randomized P3 with blinded-review primary; kept off practice-changing because pCR is a surrogate (EFS/OS immature) and node-sparing is confounded with added tislelizumab.
In pMMR/MSS LARC (cT3-4, tumor ≤10cm from verge), this is a trial-stage signal that neoadjuvant PD-1 may help an IO-resistant group; it does not extend to dMMR disease and does not yet displace conventional elective-nodal short-course RT off-protocol.
- Node-sparing RT's independent contribution vs added tislelizumab
- Whether pCR gain translates to EFS, OS, organ preservation n=30 · primary completion 2025-01 · 1° endpoint organ-retention, MSS/pMMR SCRT+IOrecruiting Node-sparing Radiotherapy Combined With Total Neoadjuvant CAPOX and Sintilimab for MSS Middle and Low Rectal Cancer Phase 2n=37 · primary completion 2027-09 · node-sparing SCRT+PD-1, W&W organ preservation
- PD-1 benefit reproducibility in MSS/pMMR rectal cancer recruiting A Series of Neoadjuvant Chemoradiotherapy Combined With Immunotherapy for Locally Advanced Rectal Cancer Phase 2/3n=375 · primary completion 2026-12 · RCT chemoRT ± tislelizumab, pMMR/MSS LARCrecruiting Neoadjuvant Chemoradiotherapy Plus Tislelizumab With or Without Probio-M9 in pMMR/MSS Locally Advanced Rectal Cancer Phase 2n=50 · primary completion 2027-05 · pMMR/MSS chemoRT+tislelizumab vs CRT-only armnot yet Neoadjuvant Chemoradiotherapy Followed by Chemotherapy With or Without Tislelizumab for Resectable Ultra-low Rectal Cancer: The RELIEVE-02 Study Phase 3n=154 · primary completion 2027-12 · phase 3 chemoRT ± tislelizumab, pMMR/MSS
📚 Sources · 🐦 1 tweet
One of most interesting rectal ca studies at #ASCO26
— Dr. Nina Niu Sanford (@NiuSanford) June 2, 2026
P3 RCT in pMMR LARC: Node-sparing short-course RT + CAPOX + tislelizumab doubled pCR v conventional SCRT + CAPOX (61 v 29%)
Hypothesis = sparing elective node RT preserves antitumor immunity & improves PD1 response @OncoAlert pic.twitter.com/6xvA6ne0mg
CAN-2409 NCT01436968
ForIntermediate or high-risk localised prostate cancer, EBRT candidates
TL;DRDFS HR 0.70 (0.52-0.94, p=0.016) adding intraprostatic CAN-2409 to EBRT in intermediate/high-risk localised prostate; OS and PCSM immature.
The RT read is local control: 2yr biopsy positivity fell 36.4% to 19.6% (p=0.0015), comparable to adding ADT (RTOG 9408) but on standard 78Gy without a brachy or SIB boost. Whether it adds over modern dose-intensification plus ADT is the open integration question, since ADT was optional and no boost was used.

| Endpoint | CAN-2409 | Placebo | HR / p |
|---|---|---|---|
| DFS median | NR | 86.1 mo | HR 0.7 (0.52-0.94), p=0.0155 |
| 2yr biopsy pCR | 80.4% | 63.6% | n/a |
| 2yr local recurrence | 19.6% | 36.4% | p=0.0015 |
+1 more figure

| Trial | Intensifier | Local endpoint: control → intensified |
|---|---|---|
| RTOG 9408 | +4mo ADT | 2yr biopsy+ 40% → 20% |
| ASCENDE-RT | LDR brachy boost | 10y local failure 7.1% → 1.5% |
| FLAME | SIB 95Gy | Crude local failure 7.7% → 2.7% |
| CAN-2409 | +CAN-2409 | 2yr biopsy+ 36.4% → 19.6% |
8 details
Phase 3, double-blind, placebo-controlled RCT, 2:1 randomisation, N=745 across 51 US and Puerto Rico centres. Median follow-up 50.3 mo.
Intermediate or high-risk localised prostate cancer, ECOG 0-2, planned for EBRT. Stratified by risk category and ADT use. 79% White, 16% Black.
EBRT 78 Gy/2 Gy, or hypofractionated 60 Gy/3 Gy or 70 Gy/2.5 Gy. ADT optional. No dose-escalation or brachytherapy boost mandated.
Three intraprostatic aglatimagene injections (5×10^11 viral particles) plus valacyclovir prodrug, versus placebo plus valacyclovir.
Primary: disease-free survival (recurrence or death, ITT). Secondary/exploratory: OS, PCSM, 2-year post-RT biopsy pathologic response.
Primary met: DFS favoured aglatimagene; OS and PCSM immature, not significantly different. Arm-by-endpoint values in the results figure.
| Event (G3+) | Aglatimagene | Placebo |
|---|---|---|
| Any TEAE | 8% (40/479) | 7% (17/232) |
| Acute kidney injury | 2% (9/479) | 2% (4/232) |
| Serious AEs | 6% (28/479) | 7% (17/232) |
Grade 3+ TEAEs 8% vs 7%; most common acute kidney injury (2% both arms). Serious AEs 6% vs 7%. No treatment-related deaths.
Discussant benchmarked the biopsy-positivity gain against ADT (RTOG 9408), brachytherapy boost (ASCENDE-RT), and SIB (FLAME) as established local-control intensifiers.
DFS is a composite surrogate; OS and PCSM immature. ADT optional, no boost mandated, confounding added value over modern intensification. Accrual (2012-2021) predates PSMA staging.
Positive phase 3 primary (DFS) but on a surrogate/composite; OS and PCSM immature (1 event/arm). Additive benefit over modern dose-intensification plus ADT unproven.
In intermediate or high-risk localised prostate cancer planned for definitive EBRT, this informs whether an added intraprostatic biologic could improve local control; it does not extend to post-prostatectomy, salvage, or metastatic settings.
- Does the local-control gain add over modern dose-escalation and ADT?
- Do DFS and pCR gains translate to overall or cancer-specific survival?
- Optimal ADT and RT-intensification pairing with intraprostatic CAN-2409
📚 Sources · 🐦 1 tweet · 📄 1 paper
🗣️Prostate Oral Abstract #ASCO25
— Michael Serzan, MD (@MikeSerzanMD) June 3, 2025
👉Dr @angela_jia_ discusses "Better Treatments, Better Selection: Improving Patient Outcomes in Localized Prostate Cancer"
🔑 KEY TAKE AWAYS
- #CAN2409 improves DFS and 2yr PathCR however PCSM and OS remain immature.
❓How to integrate with… pic.twitter.com/WamsneYBI1
Abstract
MIRACLE-2
For1L unresectable MSS rectal cancer, synchronous liver/lung mets
TL;DR68% ORR, mOS 23.2mo, 18% NED with RT-primed chemo + tislelizumab in MSS unresectable met rectal ca.
The RT-relevant read is technique: HFRT to the primary plus HFRT/SBRT to mets, delivered first to prime immunity, but no dose or fractionation in source, so it doesn't transfer to practice yet. 18% (9/50) converted to NED via resection or watch-and-wait. Near-universal lymphopenia (95.9% all-grade, 36.7% G3/4) undercuts a strategy premised on RT-driven T-cell activation.

| Metric | n (%) | 95% CI |
|---|---|---|
| CR | 1 (2.0%) | |
| PR | 33 (66.0%) | |
| SD | 10 (20.0%) | |
| PD | 6 (12.0%) | |
| ORR | 34 (68.0%) | 53.6-80.0% |
| DCR | 44 (88.0%) | 76.0-95.2% |
| ETS | 38 (76.0%) | 62.4-86.8% |
9 details 2 trials watching
Prospective single-arm phase I, N=50, Fudan University Shanghai Cancer Center. Data cutoff Dec 31 2025; median follow-up 19.9 mo (95% CI 16.4-23.4).
MSS rectal cancer, primary ≤10cm from anal verge, synchronous unresectable mets. 76% male, median age 57; 52% liver, 8% lung, 40% both; RAS/BRAF-mut 56%.
RT delivered first as an immune primer: HFRT to the primary, HFRT or SBRT to metastases. Dose, fractionation, and target volumes not reported in source.
Post-RT, biomarker-gated: FOLFOX-bevacizumab-tislelizumab (RAS/BRAF-mut) or FOLFIRI-cetuximab-tislelizumab (WT); tislelizumab 200mg Q2W. Resection/metastasectomy if converted, watch-and-wait if primary cCR.
Primary: ETS rate (≥20% target shrinkage at 8wk). Secondary: DCR, DOR, OS, PFS, safety.
ETS 76.0%, ORR 68.0%, DCR 88.0%; 18% (9/50) reached NED. Median OS 23.2mo, PFS 9.3mo, DOR 8.0mo (endpoints in table).
| Endpoint | Median | 95% CI | 1-yr rate |
|---|---|---|---|
| OS | 23.2 mo | 15.1-31.3 | 93.3% |
| PFS | 9.3 mo | 7.1-11.5 | 33.4% |
| DOR (n=34) | 8.0 mo | 5.2-10.8 | 20% |
Single-arm phase I, N=50, no comparator to isolate RT's contribution. Surrogate primary (ETS at 8wk), short median DOR (8mo), and near-universal lymphopenia (95.9%).
Single-arm phase I, N=50; surrogate primary (ETS at 8wk); no comparator to isolate RT's contribution to the immune-priming effect.
- RT's added benefit over chemo plus PD1 alone in MSS mCRC
- Optimal RT dose and fractionation for immune priming in MSS mCRC recruiting Regorafenib Alone or in Combination With Hypofractionated/Low-dose Radiotherapy Plus Toripalimab for Metastatic Colorectal Cancer Phase 2n=108 · primary completion 2025-04 · randomized hypofrac+LDRT + toripalimab, MSS mCRCrecruiting Standard Systemic Therapy Combined With High/Low-dose Radiotherapy Plus Toripalimab for Metastatic Colorectal Cancer Phase 2n=96 · primary completion 2026-12 · high + low-dose RT + toripalimab in MSS mCRC
- Predictive biomarker for MSS response to trimodal therapy
📚 Sources · 🐦 1 tweet
MIRACLE-2: RT to primary/mets -> chemo + tislelizumab in MSS unresectable met rectal ca (N=50): 68% ORR & median OS 23 mo.
— Dr. Nina Niu Sanford (@NiuSanford) May 31, 2026
Early, single-arm data, but ~1 in 5 pts reached NED.
Suggests RT + systemic + PD1 blockade could overcome immune resistance in MSS mCRC. #ASCO26 @OncoAlert pic.twitter.com/sjnUW8x7f3
OCEANUS
ForAdvanced/refractory NSCLC on immunoradiotherapy, median age 64, 74% male
TL;DRSequential iRT beat concurrent for real-world OS in newly-dx advanced NSCLC: median 20.3 vs 16.0 mo, HR 0.68 (0.47-0.99), P=.045.
Sequential iRT (ICI and RT not overlapping) beat concurrent for real-world OS in newly-dx advanced NSCLC, HR 0.68 (0.47-0.99), P=.045, favoring temporal separation of RT from ICI. RT dose, fractionation, and target volume aren't in the source, so the signal can't yet transfer to a specific plan. The refractory RT+ICI-maintenance read was NS (P=.20).
7 details 1 trial watching
Territory-wide real-world cohort (OCEANUS, Hong Kong CDARS, >90% population coverage); NSCLC diagnosed 2010-2021 who received iRT. Overlap-weighting propensity score primary, IPTW sensitivity; landmark-based OS with weighted Kaplan-Meier and Cox (restricted mean survival time where PH violated).
335 of 3522 ICI-treated pts received RT: 155 newly-dx advanced, 180 refractory. Median age 64 (34-90), 73.7% male. Refractory analysis required survival ≥90 days (landmark).
RT dose, fractionation, modality, and target volume not reported in source. The variable studied is timing of RT relative to ICI (sequential vs concurrent), not technique.
Both comparisons favored the sequential / ICI-maintenance arm (magnitudes in table). Chemotherapy was associated with longer OS in newly-dx pts only; not significant in refractory disease.
| Setting / comparison | Experimental OS | Control OS | HR / P value |
|---|---|---|---|
| Newly-dx advanced, sequential vs concurrent iRT | 20.3 mo (95% CI 13.3-NR) | 16.0 mo (95% CI 8.3-30.0) | HR 0.68 (0.47-0.99), P=.045 |
| Refractory, RT + ICI maintenance vs RT alone | 11.2 mo (95% CI 7.9-20.6) | 6.7 mo (95% CI 4.4-17.4) | P=.20 (ns) |
Randomized data on iRT sequencing in advanced NSCLC are limited (stated by authors). RT-before-ICI direction is consistent with the PACIFIC consolidation paradigm, but PACIFIC treated curative-intent unresectable stage III with concurrent chemoRT, a different population.
Observational: sequential vs concurrent not randomized, residual confounding by indication despite weighting. Small subgroups (155 newly-dx). Refractory comparison non-significant (P=.20).
Observational real-world cohort; sequential-vs-concurrent not randomized, confounding by indication despite propensity weighting. Small subgroups (155 newly-dx). Authors label it hypothesis-generating.
In newly-diagnosed advanced NSCLC starting immunoradiotherapy, this real-world signal supports separating RT from ICI in time rather than delivering them concurrently; it does not extend to refractory disease, where the RT-plus-ICI-maintenance benefit was not significant.
- Optimal RT-ICI sequencing (sequential vs concurrent) in advanced NSCLC active PD-1 Inhibitor and Chemotherapy With Concurrent Irradiation at Varied Tumour Sites in Advanced Non-small Cell Lung Cancer Phase 3n=327 · primary completion 2026-12 · phase 3 concurrent RT+PD-1 in stage IIIB/IV NSCLC
- Value of ICI maintenance after RT in refractory NSCLC
📚 Sources · 📄 1 paper
Abstract
RAD-IO
ForT2-T4a N0M0 muscle-invasive urothelial bladder cancer
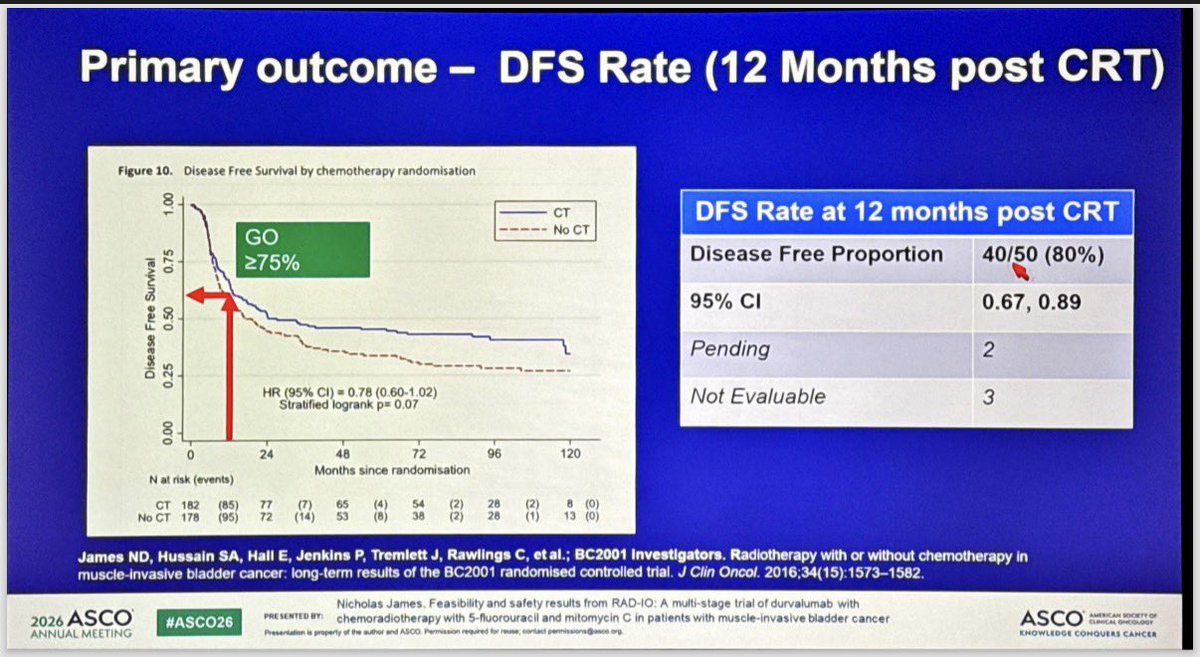
TL;DR12-mo DFS 40/50 (80%, 95% CI 0.67-0.89) cleared the pre-set ≥75% GO bar for durvalumab added to 5FU/MMC chemoRT in MIBC.
RT is standard and transferable: 55Gy/20fx to bladder, plus 46Gy/20fx elective nodal coverage in the node-positive expansion, extending durvalumab-chemoRT preservation to N+ disease. 12-mo DFS 80% (40/50, 95% CI 0.67-0.89) cleared the pre-set ≥75% GO bar vs BC2001. Moves whether to layer IO onto a hypofractionated preservation backbone.
+1 more figure

8 details 4 trials watching
Single-arm, multi-stage feasibility and safety trial testing durvalumab added to 5FU/MMC chemoradiation for bladder preservation. Benchmarked against BC2001 historical CRT data, not a randomised comparator.
T2-T4a N0M0 urothelial muscle-invasive bladder cancer, stratified by prior neoadjuvant chemotherapy (yes vs no). A stage-1 expansion added the first 6 node-positive pts.
Durvalumab 1500 mg given neoadjuvant, synchronous, and adjuvant to 12 months post-chemoRT. Concurrent 5-FU 500 mg/m²/24h ×5 days and mitomycin C 12 mg/m².
55 Gy in 20 fractions to bladder (hypofractionated). Node-positive expansion added 46 Gy/20 fx elective nodal RT.
Primary: 12-month disease-free survival post-chemoRT, read against a GO/NO-GO framework (GO ≥75%, contextual 60-75%, NO-GO <60%).
12-mo DFS 40/50 (80%), 95% CI 0.67-0.89, clearing the ≥75% GO bar. 33/54 (61%) completed planned durvalumab; investigators reported very high bladder-preservation and DFS vs prior trial data.
AEs reported in line with component therapies (chemoRT plus durvalumab). 21/54 (39%) discontinued durvalumab early.
Benchmarked against BC2001 (James, JCO 2016), where adding 5FU/MMC to RT gave DFS HR 0.78 (0.60-1.02), p=0.07. RAD-IO's 80% 12-mo DFS is claimed higher than prior data, but the comparison is non-randomised.
Single-arm with a historical benchmark and no concurrent IO comparator; 12-mo DFS is an early surrogate; small N (~50 evaluable); node-positive experience limited to 6 pts.
Single-arm feasibility stage, no randomised IO comparator; benchmarked against historical BC2001. 12-mo DFS an early surrogate at small N; met pre-set GO bar for further evaluation only.
In T2-T4a N0M0 MIBC opting for bladder preservation, this supports durvalumab layered onto 5FU/MMC chemoRT as worth further evaluation; it does not yet establish that IO improves on chemoRT alone, and node-positive experience rests on only 6 expansion pts.
- Does durvalumab add over chemoRT alone in a randomised trial n=11 · primary completion 2026-02 · randomised chemoRT ± durvalumab in node+ MIBC
- Durability of bladder preservation and DFS beyond 12 months active Treating Muscle-invasive Bladder Cancer With A Non-surgical Method Consisting of Anti-PD-1 Therapy and Chemoradiation Phase 2n=71 · primary completion 2025-12 · IO+chemoRT bladder preservation, phase 2recruiting Enfortumab Vedotin in Combination With Pembrolizumab vs. Concurrent Chemoradiotherapy (cCRT) in People With Muscle Invasive Bladder Cancer (EV-309) Phase 3n=390 · primary completion 2030-03 · phase 3 EV+pembro vs cCRT bladder preservation
- Efficacy in node-positive MIBC beyond the 6-patient expansion n=11 · primary completion 2026-02 · durvalumab+chemoRT in node-positive bladder ca
📚 Sources · 🐦 3 tweets
RAD-IO: chemoradiation (5FU+MMC) + Durva in MIBC. #ASCO26 pic.twitter.com/yTyhkdjCox
— Álvaro Pinto (@dralvaropinto) May 30, 2026
#ASCO26 🔬 Abstract 4504 | RAD-IO
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
Durvalumab + chemoradiotherapy in muscle-invasive bladder cancer
Presented by Nicholas D. James, PhD, MBBS, FRCP@OncoAlert@ASCO
Bladder preservation in MIBC remains one of the most important curative-intent questions in GU oncology.
The key… pic.twitter.com/W6JqzTVsJ3
RAD-IO at #ASCO26: durvalumab added to chemoradiation in muscle-invasive bladder cancer cleared its efficacy bar in a bladder-preservation approach. Single-arm, benchmarked against prior CRT data.
— Katy Beckermann (@katy_beckermann) May 30, 2026
Durvalumab given before, during, and 12 months after chemoRT (55Gy/20Fr +… pic.twitter.com/UXxwoZzaMC
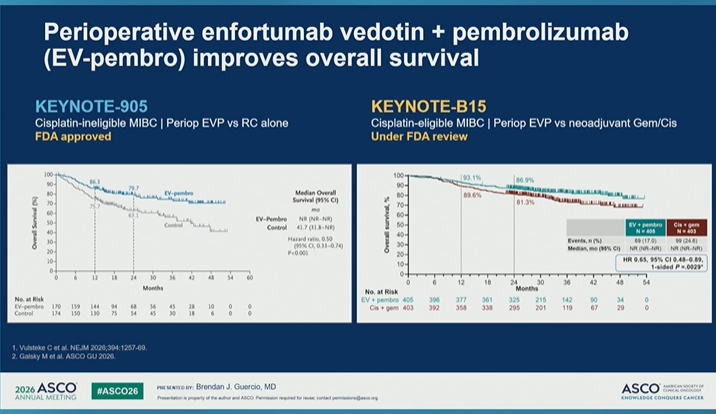
Management of MIBC After Pathologic Complete Response
TL;DRReview of perioperative MIBC management after pCR: sandwich IO regimens continue adjuvant regardless of response, cisplatin-chemo alone moves to surveillance.
SWOG 8710ABACUSCHECKMATE-274KEYNOTE-905VOLGANIAGARAVESPERKEYNOTE-B15
8 details 3 trials watching
- 🔍 pCR used as primary endpoint in signal-seeking phase 2 trials
- 🔍 pCR co-primary (not standalone) endpoint in phase 3 registrational trials
- 🔍 High-risk residual disease (≥ypT2 or N+) post-neoadjuvant chemo → adjuvant therapy (CHECKMATE-274)
- 💊 Post-pCR management by regimen
- Sandwich IO (NIAGARA, EVP): continue planned adjuvant regardless of pathologic response
- NIAGARA: resume durvalumab 8 mo post-cystectomy
- Cisplatin-based chemo alone: surveillance after pCR is standard
- 📊 pCR (pT0N0) post-neoadjuvant chemo = strong prognostic marker: SWOG 8710 85% 5-yr OS if pT0
- 📐 Meta-analysis: pooled RR 0.19 for RFS with pCR
- 📊 Perioperative regimens across trials
Trial Setting Comparison Result NIAGARA Cis-eligible Gem/Cis + periop durvalumab 24-mo OS 82.2% vs 75.2% VESPER Cis-eligible ddMVAC vs Gem/Cis 5-yr OS 66% vs 57% KEYNOTE-905 Cis-ineligible Periop EVP vs cystectomy alone OS HR 0.50 KEYNOTE-B15 Cis-eligible Periop EVP vs Gem/Cis OS improved (under FDA review)
- ⚠️ Not all pts in perioperative trials completed adjuvant therapy, often due to toxicity
- Relative contribution of pre- vs post-operative therapy components
- Can adjuvant therapy be de-escalated by pCR or biomarker n=761 · primary completion 2025-06 · adjuvant atezo gated by ctDNA+ post-cystectomyrecruiting Surveillance of the Genetic Signature in Circulating Tumor DNA for Guiding Adjuvant Chemotherapy in Urothelial Carcinoma Phase 2n=20 · primary completion 2025-09 · ctDNA-guided adjuvant gem/cis in urothelialn=992 · primary completion 2030-09 · ctDNA-guided adjuvant IO after cystectomy
📚 Sources · 🐦 1 tweet
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 Management in Bladder Cancer After Pathologic Complete Disease Response
Presented by Brendan J. Guercio, MD@OncoAlert@ASCO
In muscle-invasive bladder cancer, pCR after neoadjuvant therapy is one of the most powerful prognostic signals we… pic.twitter.com/sMd2In7X3p
Neo-CRAG
ForHigh-risk locally advanced gastric/EGJ (cT3N2-3 to cT4), fit for D2 resection
mDFS 52.7 vs 24.4 mo
HR 0.750 (95% CI 0.607-0.928), P=0.008
TL;DRAdding neoadjuvant chemoRT (45Gy/25fx) to periop XELOX improved mDFS 52.7 vs 24.4mo (HR 0.75) and mOS 67.5 vs 37.6mo in high-risk LAGC.
The RT read is clean attribution: both arms share the XELOX backbone and the CRT arm got dose-reduced chemo during RT, yet locoregional recurrence halved (9.4% vs 18.3%) with more ypN0 and downstaging. On 45Gy/25fx, this revives neoadjuvant chemoRT for high-risk D2-resected gastric/EGJ, on a non-FLOT backbone.

| Endpoint | CRT | CT | HR (95% CI), P |
|---|---|---|---|
| Median DFS | 52.7 mo | 24.4 mo | 0.750 (0.607-0.928), P=0.008 |
| 3-yr DFS | 55.6% | 42.4% | — |
| Median OS | 67.5 mo | 37.6 mo | 0.781 (0.628-0.970), P=0.025 |
| 5-yr OS | 50.1% | 44.2% | — |
7 details 2 trials watching
Phase 3 open-label RCT, 1:1, N=620 (310/arm), 13 Chinese referral centers, enrolled 2013-2022. Primary: disease-free survival; secondary OS, pCR, R0, safety.
High-risk locally advanced gastric/EGJ adenocarcinoma: cT3N2-3M0, cT4aN+M0, or cT4bNanyM0; 36.3% EGJ (Siewert II/III). All planned standardized D2 gastrectomy.
Both arms: 3 cycles preoperative + 3 cycles adjuvant XELOX (oxaliplatin 130, capecitabine 1000 BID D1-14, Q3W) around D2 gastrectomy.
CRT arm only: concurrent 45 Gy/25 fx begun after chemo cycle 1, with dose-reduced XELOX (oxaliplatin 100, capecitabine 825) during RT. RT is the sole added variable between arms.
Primary DFS met and secondary OS positive, both favoring CRT; pathologic downstaging, ypN0, and locoregional control also improved (see figure and table).
Contrasts with CRITICS and TOPGEAR, where adding radiotherapy to a chemo backbone did not improve survival. A positive DFS/OS here reopens neoadjuvant chemoRT in high-risk, D2-resected LAGC.
Open-label; non-FLOT XELOX backbone limits transfer to current perioperative standard. Single-country (China) with high D2-resection quality; DFS (not OS) was the primary endpoint.
Randomised phase 3, primary DFS and OS both hit, but positive chemoRT diverges from negative CRITICS/TOPGEAR; non-FLOT XELOX backbone limits transfer to current SOC.
In high-risk cT3N2-3/cT4 gastric or EGJ adenocarcinoma planned for D2 gastrectomy on a XELOX backbone, these data support a DFS/OS and locoregional-control benefit from adding neoadjuvant chemoRT; the signal does not extend to FLOT-backbone or metastatic patients.
- Incremental benefit of RT on a FLOT chemo backbone n=776 · primary completion 2023-06 · candidate match
- Generalizability beyond high-quality-D2 Asian centers
- Whether EGJ and distal gastric benefit equally n=4 · primary completion 2024-03 · candidate match
📚 Sources · 🐦 1 tweet
Neo-CRAG: Ph3 RCT (n=620, gastric/GEJ) - adding neoadj chemoRT to peri-op XELOX improved OS (68 v 38 mo).
— Dr. Nina Niu Sanford (@NiuSanford) May 30, 2026
Limitation=non-FLOT, BUT still relevant IMO b/c:
1) DFS/OS benefit substantial.
2) Improvements in pCR, downstg, LRR supports plausible RT effect on OS. #ASCO26 @OncoAlert pic.twitter.com/eeM0Z8p20M
SWOG/NRG S1914 NCT04214262
ForEarly-stage inoperable/surgery-declined NSCLC (T1-3N0M0 ≤7cm), ≥1 risk factor
HR 1.15
95% CI 0.65-2.01, p=0.63; did not meet primary
TL;DROS HR 1.15 (0.65-2.01), p=0.63: adding atezolizumab to SBRT did not improve survival in early-stage inoperable NSCLC; futility-stopped, excess toxicity.
Local control got worse with IO, not better: local failures 13% vs 7% adding atezolizumab, alongside null OS/PFS and a former/never-smoker harm signal (OS HR 2.50). SBRT alone stays standard for inoperable early-stage NSCLC, closing the add-IO-to-SBRT question negatively.
6 details
Phase 3 open-label RCT, 1:1, SWOG/NRG; N=403 eligible (201 S / 202 AS). Stopped at first interim for futility on OS and PFS. Median follow-up 12 mo (0.03-49).
T1-3N0M0 NSCLC ≤7cm, medically inoperable or declined surgery, ≥1 recurrence risk factor (diameter ≥2cm, SUV ≥6.2, moderate/poor/undifferentiated). Median age 73, median tumor 2.3cm, 89% ECOG 0-1.
SBRT both arms (SoC backbone): 3-8 fractions, BED ≥100 Gy. Stratified by central vs peripheral, <4 vs ≥4cm, PS 0-1 vs 2.
Atezolizumab 1200mg IV Q3wk ×8 (neoadjuvant, concurrent, adjuvant); SBRT initiated at cycle 3.
Primary: overall survival. Secondary: PFS, failure patterns, toxicity, QoL. 1-sided stratified log-rank at 2.5%.
G≥3 AEs 12% AS (21 G3, 1 G4, 1 G5 respiratory-failure death) vs 2% S. Excess toxicity with no efficacy gain.
Prior randomized phase 2 (**PMID 37478883, I-SABR, nivolumab+SBRT) suggested benefit adding IO; S1914 with atezolizumab does not confirm** and shows harm signals.
Open-label; stopped early at interim (median f/u 12mo, only 49 deaths). Former/never-smoker harm is an exploratory subgroup; central review of local recurrence ongoing.
| Endpoint | S | AS | HR (95% CI), p |
|---|---|---|---|
| 2yr OS | 82% | 80% | 1.15 (0.65-2.01), p=0.63 |
| 2yr PFS | 71% | 60% | 1.35 (0.89-2.06), p=0.16 |
| Failure | S | AS |
|---|---|---|
| Local | 7% | 13% |
| Regional | 2% | 3% |
| Distant | 4% | 5% |
| Endpoint (never/former smokers) | HR (95% CI), p |
|---|---|
| OS | 2.50 (1.11-5.59), p=0.03 |
| PFS | 2.16 (1.15-4.04), p=0.01 |
Phase 3 stopped for futility; adding IO to SBRT gave no OS/PFS benefit and excess toxicity, reaffirming SBRT-alone SOC and not confirming the prior phase 2 signal.
In medically inoperable or surgery-declined early-stage (T1-3N0) NSCLC treated with definitive SBRT, this argues against adding atezolizumab, and does not extend to node-positive or locally advanced disease.
- Biomarker/PD-L1 subset that benefits from adding IO to SBRT
- Whether excess local failures with IO hold on central review
- Reconciling harm signal with prior phase 2 IO+SBRT benefit
📚 Sources · 📄 1 paper
Abstract
Multicenter TMT Bladder Preservation Analysis (n=369)
ForMuscle-invasive bladder, cT2-T4aN0M0, median age 76
TL;DRCLR 63.7% in 369 MIBC pts on definitive TMT; 5-FU-based CRT and better image guidance predicted higher complete local response.
The two modifiable levers here are RT delivery and chemo backbone, both in the radonc's hands: 5-FU-based CRT predicted higher CLR (OR 4.9) and weekly portal imaging lower CLR (OR 0.35, p<0.001), favoring daily volumetric IGRT. Technique, not just patient selection, moved local control.
8 details 4 trials watching
Multicenter retrospective cohort, Spain 2010-2022, N=369 treated with definitive TMT (maximal TURBT + concurrent chemoRT). Multivariable logistic regression for predictors of complete local response.
cT2-T4aN0M0 muscle-invasive bladder. Median age 76, 85.1% male. Node-positive and metastatic disease excluded by staging.
Image-guidance quality tracked with local control: weekly portal imaging predicted lower CLR (OR 0.35, p<0.001), favoring daily volumetric IGRT; VMAT showed a non-significant favorable trend. RT dose/fractionation not reported in source.
Concurrent chemoradiotherapy. 5-FU-based CRT predicted higher CLR (OR 4.9, 95% CI 1.1-22.1, p=0.038).
Primary: complete local response (CLR). Secondary: OS, CSS, recurrence patterns, salvage cystectomy.
CLR 63.7%. Disease progression 28.8% (local 10.1%, systemic 10.7%, combined 8.7%). Salvage cystectomy 9.7%.
Retrospective, non-randomised; CLR predictors exploratory and confounded by treatment era. No head-to-head vs radical cystectomy; RT technique detail and CLR-survival effect sizes absent from source.
Retrospective real-world European cohort; no randomised TMT-vs-cystectomy comparator. Reinforces guideline-recognized bladder preservation; predictor findings exploratory.
In cT2-T4aN0M0 MIBC pts already committed to bladder-preserving TMT, this favors daily volumetric IGRT and 5-FU-based chemoRT for local control; it does not inform the upstream TMT-versus-radical-cystectomy choice or node-positive/metastatic disease.
- Optimal concurrent chemoradiotherapy regimen for bladder preservation active Treating Muscle-invasive Bladder Cancer With A Non-surgical Method Consisting of Anti-PD-1 Therapy and Chemoradiation Phase 2n=71 · primary completion 2025-12 · adds toripalimab to concurrent chemoRTrecruiting Enfortumab Vedotin in Combination With Pembrolizumab vs. Concurrent Chemoradiotherapy (cCRT) in People With Muscle Invasive Bladder Cancer (EV-309) Phase 3n=390 · primary completion 2030-03 · phase 3 EV+pembro vs concurrent chemoRT
- Whether daily volumetric IGRT improves local control vs weekly imaging n=345 · primary completion 2021-12 · adaptive tumour-focused vs whole-bladder RTnot yet Evaluation of the Clinical Utility of Online Adaptive Radiotherapy in Bladder Cancer (BLADAPT-GETUG V11) Phase NAn=120 · primary completion 2029-01 · randomised online-adaptive vs standard RT in TMT
- Randomised TMT vs radical cystectomy comparison
📚 Sources · 🐦 1 tweet
📢 Presentamos en #ESTRO26 nuestro análisis multicéntrico sobre preservación vesical en cáncer vesical músculo-invasivo tratado con TMT.
— URONCOR (@URONCOR) May 19, 2026
🔎 En 369 pacientes, la respuesta completa clínica se asoció a menor recurrencia local y mejor supervivencia!@fcounago #NicoFeltes pic.twitter.com/aQjjkcHGP4
RADIOSA (MFS post-hoc)
ForOligorecurrent prostate cancer eligible for metastasis-directed SBRT
TL;DRPost-hoc MFS 16.6mo vs not reached, HR 0.39 favoring SBRT + 6mo ADT over SBRT alone in oligorecurrent prostate.
The additive read is the eugonadal MFS: benefit persisted after testosterone recovery (p<0.05), so the ADT effect is not just on-treatment suppression of imaging progression. That argues against reading RADIOSA's MFS split as a testosterone artifact, and moves the SBRT-alone vs SBRT + short-course ADT decision in oligorecurrence.
Also covered Jun 12

| Endpoint | Arm A (SBRT) | Arm B (SBRT + ADT) | Effect size |
|---|---|---|---|
| Metastatic progression | 32/51 (62.7%) | 19/51 (37.3%) | log-rank p=0.00079 |
| Median MFS | 16.6 mo (95% CI 12.83-NA) | not reached | HR 0.3894 (0.2201-0.6888), p=0.00119 |
+1 more figure

8 details 5 trials watching
Phase II randomized trial, 1:1, N=102, Arm A SBRT alone vs Arm B SBRT + 6-month ADT. Median follow-up (reverse KM) 49.23 months (95% CI 42.47-54.8). This report is a post-hoc analysis of MFS and eugonadal MFS.
Oligorecurrent prostate cancer. Detailed eligibility (number of lesions, imaging modality, prior local therapy, PSA thresholds) not reported in source.
SBRT to the oligorecurrent sites in both arms. Dose, fractionation, and target volume are not reported in source, which limits transfer to a specific practice.
MFS defined as randomisation to any M1 metastatic recurrence on imaging. Eugonadal MFS measured from testosterone recovery to new metastasis or last follow-up. KM curves compared by log-rank; HRs from Cox models.
Effect sizes are in the figure caption table. All Arm B pts except two reached testosterone recovery within follow-up.
Post-hoc analysis; MFS was not the prespecified primary endpoint. No OS reported in source, so the surrogate carries the read. Toxicity and SBRT technique parameters absent from source.
The eugonadal analysis is the substantive contribution: separating the benefit from on-treatment castration addresses the standing objection that ADT simply delays imaging-detected progression. Whether that reflects durable synergy between ablation and transient androgen suppression, as the authors argue, is hypothesis-generating at N=102.
Post-hoc endpoint analysis of a phase II trial; MFS was not the prespecified primary. Design dominates the read despite the clean randomisation and mature follow-up.
In oligorecurrent prostate cancer being considered for metastasis-directed SBRT, this supports the discussion of adding 6-month ADT over SBRT alone; it does not address de novo metastatic or castration-resistant disease, and the SBRT dose and target volume are not stated in the source.
- Does the MFS advantage translate to overall survival active Prostate-cancer Treatment Using Stereotactic Radiotherapy for Oligometastases Ablation in Hormone-sensitive Patients Phase 3n=550 · primary completion 2026-06 · phase 3 SBRT to all mets in hormone-sensitive M1
- Optimal ADT duration alongside metastasis-directed SBRT n=873 · primary completion 2027-04 · randomises 1mo vs 6mo ADT + ARTA on top of MDTrecruiting Duration of Androgen Receptor Pathway Inhibitor and ADT With Metastasis Directed Therapy in Oligometastatic Cancer of the Prostate (DIRECT) Phase 2n=132 · primary completion 2031-02 · ADT/ARPI duration arm: 8-9mo abiraterone added to SBRT
- Whether PSMA-PET staging changes the size of the benefit recruiting Veterans Affairs Seamless Phase II/III Randomized Trial of STAndard Systemic theRapy With or Without PET-directed Local Therapy for Oligometastatic pRosTate Cancer Phase 2/3n=464 · primary completion 2026-09 · randomises PET-directed local therapy vs systemic alonerecruiting Metastasis Directed Stereotactic Body Radiotherapy for Oligo Metastatic Hormone Sensitive Prostate Cancer Phase NAn=118 · primary completion 2031-12 · MD-SBRT randomised in PSMA-PET-defined 1-3 mets
📚 Sources · 🐦 1 tweet
Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 16, 2026
Post-hoc analysis of metastasis-free survival (MFS) and Eugonadal MFS in the RADIOSA phase II randomized trial Presented by Giulia Marvaso 🇮🇹 #RadOnc ☢️ @giuliamarvaso84
Post-hoc analysis of RADIOSA shows SBRT plus short-term ADT… pic.twitter.com/1zpiChkUgA