Radiation
ESTRO Prostate SBRT Consensus Recommendations
TL;DR15-expert ESTRO Delphi consensus on optimising primary prostate SBRT: patient selection, contouring, dose/fractionation, follow-up, and delivery technique.
HYPO-RT-PCPACE-B
For a department standardising primary prostate SBRT, this is the implementation reference: an ESTRO Delphi panel settles the controversy points (patient selection, contouring, dose, fractionation, follow-up, delivery technique). Planning is anchored to the PACE-B protocol (Fig 1, isodose 8 to 46 Gy).
Sets the RT technical playbook for primary prostate SBRT: patient selection, contouring, dose, fractionation, follow-up, and minimal vs optimal delivery technique, resolved by a 15-expert Delphi. Figure 1 anchors planning to the PACE-B protocol (isodose 8 to 46 Gy), useful for benchmarking or standing up a program.
4 details 5 trials watching
ESTRO clinical practice consensus, 15-expert panel, Delphi process answering a 10-item questionnaire on areas of controversy. Covers selection, contouring, dose, fractionation, follow-up, and minimal-vs-optimal delivery technique for primary prostate SBRT.
- Optimal dose and fractionation for prostate SBRT active Prostate Radiotherapy Comparing Moderate and Extreme Hypo-fractionation (PRIME Trial) Phase NAn=526 · primary completion 2024-09 · extreme vs moderate hypofx, non-inferiorityrecruiting Two-fraction Versus Five-fraction Stereotactic Radiotherapy for Localized Prostate Cancer Phase NAn=562 · primary completion 2027-12 · 2-fraction vs 5-fraction SBRT, localized
- Role of focal ablative microboost n=124 · primary completion 2022-06 · SBRT focal ablative microboost, hypo-FLAME 2.0recruiting Image-guided Focal Dose Escalation- Primary pc Treated With Primary External Beam Hypofract.Stereotactic rt Phase NAn=374 · primary completion 2025-08 · randomized focal dose escalation vs no boostactive Standard Moderately Hypofractionated RT vs. Ultra-hypofractionated Focal Lesion Ablative Microboost in Prostate Cancer Phase NAn=484 · primary completion 2032-01 · randomized standard RT vs focal microboost
📚 Sources · 📄 1 paper
NRG Oncology/RTOG 0848
ForResected pancreatic head adenocarcinoma, progression-free after adjuvant chemo
HR 0.96
90% CI 0.79-1.18, 1-sided P=.38; primary EP not met
TL;DROS primary EP not met (HR 0.96, 90% CI 0.79-1.18) adding adjuvant CXRT to gemcitabine; node-negative subgroup OS benefit on interaction (P=.0063).
The RT read is the node-negative interaction: CXRT improved OS (P=.0063) and DFS (P=.014) in node-negative pts, though the subgroup HR/median isn't in the source text. Unlike ESPAC-1's older 5-FU CXRT, modern CXRT showed no OS harm. Moves selective adjuvant CXRT for node-negative resected head tumors, pending FOLFIRINOX-era confirmation.
This reopens selective adjuvant CXRT in node-negative resected head tumors (OS interaction P=.0063), where modern technique avoided the OS harm ESPAC-1 saw. Cost is doubled grade 3 toxicity (38% vs 19%); dose and target volume aren't in the source, and node-positive pts got no benefit.
Adjuvant gemcitabine-based chemo alone stays the reference: adding CXRT didn't improve OS (HR 0.96) or DFS (HR 0.82, P=.089) overall and raised grade 3 toxicity to 38% vs 19%. The node-negative interaction (P=.0063) would need retesting against FOLFIRINOX before altering adjuvant sequencing.
8 details 3 trials watching
Multicenter phase IIR/III, two-step RCT. Step 1: gemcitabine vs gemcitabine + erlotinib. Step 2 (reported here): random assignment to a sixth chemo cycle ± CXRT after 5 progression-free cycles. N=354 (180 CXRT, 174 chemo).
Curative-intent resected pancreatic head adenocarcinoma, progression-free on adjuvant chemo. Median age 63, 55% male, 56% PS 1.
Fluoropyrimidine-sensitized CXRT added to the sixth cycle. Dose, fractionation, and target volume not stated in the source excerpt.
Primary: overall survival. Secondary: DFS. Powered for HR 0.76 (316 events, 80% power, 1-sided α=.05).
Primary OS not met (HR 0.96). The one positive signal was the treatment-by-nodal-status interaction (OS P=.0063, DFS P=.014) favoring CXRT in node-negative pts; subgroup effect size not in source.
| Endpoint | Chemo + CXRT | Chemo alone |
|---|---|---|
| Median OS | 2.3 yr (2.0-2.6) | 2.6 yr (2.1-3.1) |
| 5-yr OS | 27.9% (22.2-33.6) | 23.1% (17.7-28.6) |
| OS HR (90% CI) | 0.96 (0.79-1.18), P=.38 | ref |
No increase in grade 4/5 toxicity. Grade 3 toxicity higher with CXRT: 38% vs 19% (P<.001).
ESPAC-1's older 5-FU-based CXRT suggested inferior outcomes; here modern CXRT shows no OS harm but no all-comer benefit. Backbone predates FOLFIRINOX-type adjuvant chemo, named in the source as current SOC.
Node-negative benefit rests on a subgroup interaction, not the prespecified primary. Trial underwent multiple mid-course modifications (LAP07, accrual, slow event rate), and no local-control or pattern-of-failure endpoint is reported despite RT's locoregional rationale.
Clean negative primary OS (HR 0.96) reinforces no routine adjuvant CXRT; node-negative benefit is a subgroup interaction needing confirmation; gemcitabine backbone predates FOLFIRINOX.
In resected node-negative pancreatic head adenocarcinoma completing adjuvant gemcitabine, this offers a subgroup signal favoring fluoropyrimidine-sensitized CXRT (OS interaction P=.0063); it does not extend to node-positive pts, where CXRT showed no OS or DFS benefit.
- Does node-negative CXRT benefit hold with mFOLFIRINOX backbone? n=770 · primary completion 2028-06 · phase 3 adjuvant CXRT vs chemo, resected high-risk
- Neoadjuvant vs adjuvant CXRT sequencing in node-negative resected pancreas recruiting Preoperative Stereotactic Body Radiation Therapy in Patients With Resectable Pancreatic Cancer Phase 2n=25 · primary completion 2026-09 · preop SBRT then resection in resectable pancreas
- Local-regional control and pattern of failure with modern CXRT n=30 · primary completion 2028-10 · freedom from local failure at 12mo, SBRT
📚 Sources · 📄 1 paper
Abstract
TROG 08.03 RAVES QOL Substudy
ForPost-RP prostate cancer with adverse pathology or PSA >0.2 ng/ml
TL;DRAt 5yr, 16% vs 2% severe urinary leakage aRT vs no RT (p=0.01); sRT timing had no QOL effect.
The mechanism of sRT's benefit is sparing, not delay: time from RP to RT showed no association with any QOL domain at 3-5 yr (all coefficients ns), and irradiated sRT pts looked like aRT pts. The gain sits entirely with the men who never need RT, so late salvage confers no functional dividend over early salvage.
9 details 4 trials watching
Planned secondary analysis of the TROG 08.03 RAVES randomised trial comparing adjuvant RT with salvage RT delivered at PSA >0.2 ng/ml after radical prostatectomy. Patient-reported QOL collected prospectively across multiple Australian and New Zealand sites.
EORTC QLQ-C30 and QLQ-PR25. The unit of analysis is a minimal clinically important change (MCIC), a decline of >0.5 SD from baseline, in bowel symptoms, urinary symptoms, sexual activity, and sexual functioning.
The aRT arm (n=166) reported more bowel-symptom MCIC at 1-5 yr than sRT pts who never required RT. Against pts in the sRT group who did receive RT, no consistent differences in urinary, bowel, or sexual domains emerged.
| Timepoint | Adjuvant RT | No RT | p |
|---|---|---|---|
| 4 yr | 15/124 (12%) | 1/59 (1.7%) | 0.02 |
| 5 yr | 18/111 (16%) | 1/50 (2%) | 0.01 |
| Domain / timepoint | aRT | sRT | p |
|---|---|---|---|
| Sexual activity MCIC, 3 yr | 32% | 58% | 0.004 |
| Sexual activity MCIC, 4 yr | 43% | 65% | 0.038 |
| Urinary symptom MCIC, 2 yr | 23% | 38% | 0.036 |
| Severe urinary leakage, 5 yr | 16% | 13% | 0.7 |
Dose, fractionation, and target volume are not reported in the source text. Median follow-up from RT was 2.6 yr in the salvage group who received RT (IQR 1.2-5.2), and aRT pts started RT younger (63.9 vs 66.8 yr, p=0.01).
Self-reported QOL in an unblinded trial, so expectancy cuts toward the arm that knows it was irradiated. Denominators thin sharply by 5 yr (23 sRT pts post-RT; 8 in the no-RT sexual-functioning group), and the scattered significant timepoints in the aRT-vs-sRT comparison are fragile at that N.
Reframes the early-salvage rationale: the QOL dividend is sparing roughly the share of men who never trigger RT, not delaying exposure. That matters because delay was the intuitive mechanism, and the regression data do not support it.
Prespecified secondary QOL analysis of a randomised trial; supports the already-guideline-endorsed early-salvage strategy. Small late-timepoint denominators and unblinded self-report temper it.
In post-RP men with adverse pathology deciding adjuvant versus PSA-triggered salvage, this supports counselling that the QOL advantage comes from avoiding RT altogether rather than from postponing it; it does not inform men who already have a rising PSA and will be irradiated either way.
- Does hypofractionated post-prostatectomy RT alter the late incontinence signal? recruiting Hypofractionated Post-prostatectomy Radiotherapy (HYPORT)for Localized Prostate Cancer Phase NAn=428 · primary completion 2026-02 · hypofx vs conventional post-RP RT, safety endpointn=538 · primary completion 2029-09 · phase 3 hypofx vs conventional salvage bed RT
- Does PSMA-guided salvage timing change functional outcomes? recruiting PSMA-PET Guided De-escalation of Salvage Radiation Treatment in Recurrent Prostate Cancer Phase 2n=54 · primary completion 2029-09 · PSMA-guided de-escalated SRT; 1° EP acute G≥2 toxn=380 · primary completion 2032-12 · eSRT at PSA 0.2 vs dSRT 0.4-0.5; safety endpoint
📚 Sources · 📄 1 paper
TREASURE NCT04462276
ForES-SCLC, ≥stable disease after chemo-IO induction; unselected
6.7 vs 13.4 mo
HR 1.55 (95% CI 0.90-2.69), P=.34; TRT arm worse, ns
TL;DRmOS 6.7 vs 13.4mo (HR 1.55, ns) adding consolidative TRT to atezo maintenance; halted early for SAEs 61% vs 18%.
The harm, not the null OS, is the RT read: SAEs 61% vs 18%, fatal AEs 19% vs 3%, driven by post-TRT lymphocyte depletion and low baseline DLCO in the fatal cases. 30Gy/10fx consolidative TRT on atezo maintenance is net harmful in unselected ES-SCLC; any future use needs lung-function gating.
6 details 1 trial watching
Phase 2 open-label RCT (AIO-TRK-0320), 1:1, 20 sites in Germany/Austria. Planned 104 pts; halted early by the SMC after 68 randomized (34/arm) for excess fatal SAEs in the TRT arm. Recruited 2020-2022, last follow-up Sept 2024, post-hoc survival update April 2026.
ES-SCLC with at least stable disease after induction carboplatin-etoposide-atezolizumab. Baseline well balanced between arms and between pts with vs without SAEs. Unselected for lung function.
Consolidative TRT 30 Gy in 10 fractions added to atezolizumab maintenance (arm A) vs atezolizumab maintenance alone (arm B).
Primary: overall survival. Secondary included PFS and safety.
Primary OS not met: the TRT arm was numerically worse with no PFS difference and sharply higher serious and fatal toxicity (see table).
| Endpoint | +TRT (arm A) | Atezo alone (arm B) | Effect |
|---|---|---|---|
| mOS | 6.7 mo (5.1-9.0) | 13.4 mo (10.7-17.5) | HR 1.55 (0.90-2.69), P=.34 |
| mPFS | 2.4 mo (1.3-3.9) | 2.6 mo (1.2-3.9) | HR 0.92 (0.54-1.55), P=.85 |
| SAEs | 61.3% | 18.2% | P<.001 |
| Fatal AEs | 19.4% | 3.0% | P=.04 |
SAEs dominated by infection and respiratory disorders, linked to radiation-induced lymphocyte depletion; fatal-AE pts in arm A had lower baseline DLCO. No other risk factors identified.
CREST (pre-immunotherapy) showed a modest OS benefit from thoracic RT after chemo; TREASURE tested that strategy on an IMpower133-style IO-maintenance backbone and found harm, not benefit.
Open-label; small N (68) and early termination leave OS underpowered with a wide CI. Phase 2; efficacy conclusions provisional, though the safety signal is robust.
Randomised harm signal (SAEs 61% vs 18%, fatal 19% vs 3%) argues against adding consolidative TRT to IO maintenance, contesting emerging RT enthusiasm; OS worse but underpowered by early stop.
In unselected ES-SCLC with at least stable disease after chemo-IO induction, this evidence argues against routinely adding consolidative thoracic RT to atezolizumab maintenance; it does not address the good-lung-function subset the authors flag as possibly selectable.
- Which lung-function-selected ES-SCLC pts might tolerate consolidative TRT on IO maintenance not yet Adebrelimab Combined with Chemotherapy and Thoracic Radiotherapy for First-line Treatment of ES-SCLC Phase 3n=524 · primary completion 2029-06 · phase 3 consolidative TRT on adebrelimab IO maintenance
- Whether lower-dose or delayed TRT lessens lymphocyte depletion and infection risk
📚 Sources · 📄 1 paper
Abstract
HYDRA
ForLocalised prostate cancer, definitive EBRT, moderately hypofractionated
TL;DRNo PFS difference vs conventional RT for either MHFRT type, but dose-escalated MHFRT alone raised late G2+ GI + bowel-QoL decrement; isodose 60/20 clean.
The split that matters: dose-escalated MHFRT raised late G2+ GI (OR 1.48, p=0.0035) and patient-reported bowel decrement (OR 1.68, p=0.023), while isodose 60/20 stayed clean on every toxicity and QoL axis at equal PFS. Escalating buys no efficacy, so default to isodose MHFRT.
8 details 5 trials watching
IPD meta-analysis of 7 phase 3 RCTs (MARCAP consortium) of CFRT vs MHFRT. Primary efficacy endpoint PFS; co-primary toxicity late G2+ GU and G2+ GI; co-primary PRO urinary/bowel QoL decrement. Two prespecified strata: isodose vs dose-escalated MHFRT.
Localised prostate cancer. CFRT arm required modern dose (≥70 Gy in 2 Gy equivalents); trials lacking published IPD efficacy or late-toxicity data excluded. 3454 pts across 3 isodose trials, 2426 pts across 4 dose-escalated trials.
Isodose MHFRT exemplified by 60 Gy in 20 fractions; dose-escalated MHFRT schedules pooled (specific fractionations not given in source). Median follow-up 5.4 y (isodose) and 7.1 y (dose-escalated).
Efficacy equivalent to CFRT for both strata. The only toxicity separations were in the dose-escalated arm, late G2+ GI and bowel QoL, not isodose (see table).
Reinforces isodose 60/20 (CHHiP-type) as the standard MHFRT regimen and argues against dose-escalating hypofractionated schedules, which buy no efficacy but cost bowel toxicity.
Physician-scored late toxicity carries grading subjectivity, though PRO data corroborate the bowel signal. Dose-escalated stratum pools heterogeneous fractionation; longer follow-up needed to confirm late-toxicity divergence.
IPD meta-analysis of 7 phase 3 RCTs consolidating isodose 60/20 as standard MHFRT; reinforces current practice, no efficacy gained by dose-escalating.
In localised prostate cancer choosing moderate hypofractionation, this supports isodose 60 Gy/20 fx over dose-escalated hypofractionated schedules; it does not speak to SBRT/ultrahypofractionation or node-positive disease.
- Late-toxicity divergence with follow-up beyond 7 years
- Whether ultrahypofractionation (SBRT) shares the dose-escalation toxicity penalty n=54 · primary completion 2027-02 · 2-fx MR-linac dose de-escalation vs bowel/GU toxicityn=42 · primary completion 2028-01 · 40Gy/5fx SABR, GI/GU vs historical rates
- Optimal dose-escalated schedule if used in higher-risk disease active Comparative Study of Radiotherapy Treatments to Treat High Risk Prostate Cancer Patients Phase 3n=307 · primary completion 2026-12 · HDR boost vs hypofx dose-escalation, high-riskrecruiting Hypofractionated Radiotherapy With a Focal Microboost for High-Risk and Locally Advanced Prostate Cancer Phase 2n=46 · primary completion 2029-01 · hypofx focal microboost, high/very-high riskrecruiting Tumor-directed Radiation Therapy for Patients With the Highest Risk Category of Localized Prostate Cancer Phase NAn=76 · primary completion 2031-09 · ultra-hypofx boost + nodal RT, very high-risk
📚 Sources · 📄 1 paper
Abstract
ASTRO 2024: SBRT for Unfavorable Intermediate-Risk Prostate Cancer
TL;DRModern 5-fraction SBRT (1-2% bothersome toxicity vs 10-30% for 2D-era 45fx) is now NCCN-endorsed for UIR prostate; focal-boost de-escalation is next.
Reported via UroToday →
RTOG 9408HYPO-RT-PCPACE BFLAME 2.0FORT
The actionable RT read is urethral dose: PACE-B did not require urethra contouring, so ≥48 Gy hotspots (~121 Gy EQD2) likely drove the higher G2+ GU (5.4% vs 3.7%). Routine urethra delineation plus a V44 constraint, not avoiding SBRT, is what lowers toxicity.
9 details 5 trials watching
ASTRO 2024 EDU 16 educational session (Dr. Spratt); narrative review of SBRT for UIR prostate, not a new trial. Synthesizes RTOG 9408, HYPO-RT-PC, PACE-B and focal-boost series.
Modern SBRT is 5 fx over 1-2 weeks (vs 2D-era 45 fx/9 wk). Reviewed schedules: HYPO-RT-PC 42.7 Gy/7 fx, PACE-B 40 Gy CTV / 36.25 Gy PTV in 5 fx, focal-boost 36.25 Gy/5 fx + DIL 45-50 Gy.
Pooled late G3+ GU 2.0% (1.4-2.8), GI 1.1% (0.6-2.0). Higher dose improves biochemical control (P=.018) but worsens late G3+ GU (P=.014).
PACE-B 5-yr: no EFS difference SBRT vs conventional; G2+ GU 5.4% vs 3.7% (p=0.28). NCCN lists SBRT for nearly all risk groups including UIR.
Spratt argues SBRT toxicity reflects missing dose constraints, not the modality: un-contoured urethra in PACE-B allowed ≥48 Gy hotspots. Field is moving toward whole-gland de-escalation with a focal DIL boost.
| RTOG 9408 secondary | Distant mets HR (95% CI) | PCSM HR (95% CI) |
|---|---|---|
| UIR vs FIR | 2.36 (1.44-3.89), P=.001 | 1.84 (1.29-2.62), P=.001 |
| ADT benefit in UIR | 0.48 (0.28-0.83), P=.008 | 0.40 (0.26-0.60), P<.001 |
In unfavorable intermediate-risk localized prostate, this supports 5-fraction SBRT as an NCCN-listed definitive option with urethra contouring; whole-gland de-escalation plus focal DIL boost remains investigational, not standard practice.
- Does focal-boost with whole-gland de-escalation improve the therapeutic ratio? recruiting Image-guided Focal Dose Escalation- Primary pc Treated With Primary External Beam Hypofract.Stereotactic rt Phase NAn=374 · primary completion 2025-08 · randomized focal dose-escalation vs standard RTn=68 · primary completion 2025-10 · MRI integrated index-tumor boost, 5y toxicityn=23 · primary completion 2026-12 · PSMA-guided focal microboost, spare resolved areas
- Optimal urethral dose constraint to reduce G2+ GU after prostate SBRT recruiting Daily Adaptive Radiation Therapy Using an Individualized Approach for Prostate Cancer Phase NAn=132 · primary completion 2026-07 · urethra-sparing adaptive SBRT, EPIC urinary endpointn=42 · primary completion 2028-01 · central urethra-sparing SABR, GU toxicity endpoint
📚 Sources · 📄 1 paper
Abstract
SUPREMO
ForPost-mastectomy breast cancer, pN0 or 1-3 positive nodes
TL;DR10yr chest-wall recurrence 1.1% vs 2.5% (HR 0.45), no DFS/OS gain, but trial prohibited RNI so tests incomplete PMRT.
Even with SUPREMO's truncated field (chest-wall RT alone, supraclav in just 12%), the supplement shows local recurrence still fell 4.8% to 3.3% (HR 0.51) in node-positive pts. A partial RT field still helping argues FOR nodal irradiation, not omission, in 1-3 node+ disease, so the null OS/DFS shouldn't justify omitting PMRT.
Also covered Jul 7
8 details 4 trials watching
ASO editorial (Naoum, Taghian) critically evaluating SUPREMO. SUPREMO randomized post-mastectomy pts to chest-wall irradiation vs observation; RNI was prohibited, so it tested chest-wall RT alone, not chest-wall plus nodal PMRT.
Only 25% truly node-negative; the majority had N1 (1-3 positive nodes). 65% hormone-receptor-positive, 10% triple-negative. Post-neoadjuvant pts are out of scope.
Chest-wall irradiation alone. Supraclavicular coverage reached only 12% of the PMRT arm (n=97), internal mammary RT under 2% both arms, and regional nodal irradiation was otherwise prohibited.
No DFS or OS benefit from chest-wall irradiation; the only positive signal is reduced local recurrence (see table).
| Endpoint | CW-RT | No RT | Effect |
|---|---|---|---|
| 10yr chest-wall recurrence | 1.1% | 2.5% | HR 0.45 |
| LRR (supplement) | 3.3% | 4.8% | HR 0.51 (0.27-0.96) |
Danish and British Columbia trials, plus MA-20 and EORTC 22922, showed regional nodal RT improves LRR, DFS, and breast-cancer mortality in 1-3 node+ disease, even after ALND. SUPREMO's chest-wall-only field never tested this.
Node-negative dilution (25%) may mask node-positive benefit; incomplete nodal field; TNBC (10%) underpowered with a paradoxical forest-plot direction; only 10-year follow-up for a 65% HR-positive cohort prone to late recurrence.
The editorial's read: SUPREMO's null headline should not license omitting PMRT in node-positive pts, because it never tested chest-wall plus nodal RT. Even its truncated field improved node-positive local recurrence, consistent with the Danish, British Columbia, and EBCTCG data.
SUPREMO tested chest-wall RT alone, prohibited RNI, and diluted with 25% node-negative pts, so its null DFS/OS can't establish PMRT omission for node-positive disease.
In 1-3 node-positive post-mastectomy pts, this critique cautions against reading SUPREMO as clearance to omit nodal RT; it does not extend to truly node-negative pts, where SUPREMO and EBCTCG show no PMRT benefit.
- Full nodal RT vs chest-wall-only PMRT in 1-3 node-positive disease active Standard or Comprehensive Radiation Therapy in Treating Patients With Early-Stage Breast Cancer Previously Treated With Chemotherapy and Surgery Phase NAn=1636 · primary completion 2023-09 · comprehensive nodal vs standard RT, phase 3active Postmastecomy Internal Mammary Nodal Irradiation for High-risk Breast Cancer Patients Phase 3n=2400 · primary completion 2025-11 · randomised IMN nodal RT vs none, DFS endpointrecruiting The T-REX Trial: Tailored Regional External Beam Radiotherapy in Clinically Node-negative Breast Cancer Patients With 1-2 Sentinel Node Macrometastases. Phase NAn=1350 · primary completion 2028-12 · randomised omission of regional RT, 1-2 macrometsrecruiting RecurIndex Guided Avoidance of Regional Nodal Irradiation for Node Positive Breast Cancer Phase NAn=540 · primary completion 2029-08 · RNI vs avoidance in N1, RecurIndex-guided
- PMRT value in triple-negative post-mastectomy disease
📚 Sources · 📄 1 paper
ESTRO Oral Cavity CTV Delineation Guidelines
TL;DRNew consensus recipe for post-op CTV: recreate pre-op GTV-P +10mm composited with surgical defect/flap +5mm; standardizes OCSCC delineation at EQD2 60 Gy.
DAHANCA
The recipe is asymmetric: 10mm around the recreated pre-op GTV-P but only 5mm around the surgical defect/flap, composited. Recreating the GTV-P pre-op (not relying on the defect alone) is the load-bearing step; one buccal case would have missed the infratemporal fossa otherwise. Standardizes OCSCC post-op contouring at EQD2 60 Gy.
7 details
Consensus clinical guideline from an ESTRO multidisciplinary expert panel; proposals drafted, then validated by a second tier of international HNSCC experts across many countries for worldwide applicability. Not a trial, no outcome data.
Post-operative oral cavity SCC (OCSCC) requiring PORT. Fills a gap: no prior systematic consensus for post-op primary + nodal CTV in mucosal HNSCC, a source of wide institutional variation.
CTV-P post-op = (GTV-P pre-op + 10mm) composited with (surgical defect/flap + 5mm), edited for air/bone/teeth/fascial planes. Surrogate GTV-P/N recreated on the planning scan via MRI/CT registration or anatomical landmarks. Nodal CTV-N1 = GTV-N + involved level, CTV-N2 covers prophylactic at-risk levels, with uni- vs bilateral neck guidance. Example dose EQD2 60 Gy (2 Gy/fx).
Extends the 2018 primary-setting CTV guidelines (5mm + 5mm geometric expansion) into the post-op setting. DAHANCA data showed geometric margins give more conformal CTVs than anatomical ones, and a protocol switch correlated with lower late dysphagia in an unplanned post-hoc analysis.
Expert consensus, not outcome-validated. The benefit is standardization (reduced inter-institutional variation, enabling RTQA and multi-institutional trials), not a demonstrated survival or toxicity endpoint.
In resected oral cavity SCC referred for PORT, this defines a standardized post-op CTV recipe; it does not extend to definitive (non-operative) RT or to other head/neck subsites (larynx, oropharynx, hypopharynx), which await their own guidelines.
- Whether standardized CTV margins reduce marginal recurrence vs current practice
- Extension to other head/neck subsites beyond oral cavity
📚 Sources · 📄 1 paper
10-yr SBRT for Prostate Cancer (Meier Nonrandomized Trial)
ForLow- and intermediate-risk localized prostate, no ADT, Gleason ≤7, PSA ≤20
TL;DR10-yr OS 84%, RFS 90% (94% LR, 86% IR); late G3 GU/GI ≤1.5%, no G4-5; 40Gy/5fx SBRT, no ADT, 21 centers
The unfavorable-IR subgroup is the read: 10-yr RFS 77% vs 92% favorable-IR, so SBRT monotherapy without ADT looks adequate for LR/favorable-IR but leaves unfavorable-IR pts short. 40Gy/5fx transfers directly to practice. Late GU G2+ 14% (vs GI 2.1%) is the toxicity to counsel.
9 details 4 trials watching
Investigator-initiated phase 2 nonrandomized single-arm trial, N=310 evaluable across 21 community, regional and academic centers, treated 2008-2010. Median follow-up 9 yr; 10-yr Kaplan-Meier estimates.
172 low-risk (T1b-T2a, Gleason 6, PSA ≤10) and 138 intermediate-risk (Gleason 7 with PSA ≤10, or Gleason 6 with PSA 10-20), central path review. Median age 68; prostate volume up to 100 cc; ADT not allowed.
40 Gy in 5 fractions (8 Gy×5) on a noncoplanar robotic platform with real-time motion management, dose escalated to ~100 Gy EQD2 (α/β=2).
10-yr OS 84% and overall RFS 90%; risk-group and favorable/unfavorable IR breakdown in the results table. Relapse defined as biochemical failure (nadir+2), clinical failure, or salvage/systemic therapy.
| Subgroup | 10-yr RFS |
|---|---|
| Overall | 90% |
| Low-risk | 94% |
| Intermediate-risk | 86% |
| Favorable IR | 92% |
| Unfavorable IR | 77% |
Late G3 GI/GU 1.4% LR, 1.5% IR; no grade 4-5. G2+ GI 2.1% vs GU 14%, the dominant late burden. Physician-reported CTCAE v3.
PACE-B showed SBRT noninferior to conventional EBRT at 5 yr; this extends single-arm SBRT durability to 10 yr, consistent with the cohort's prior 5-yr low-toxicity report.
Single-arm, no randomized comparator; toxicity is physician-reported (CTCAE v3), not patient-reported, so late GU burden may be understated; RFS folds salvage/systemic therapy into the relapse endpoint.
Single-arm nonrandomized phase 2; no comparator arm (PACE-B provides randomized evidence). Mature 10-yr data reassure but design caps the read below confirmatory.
In low- and favorable-intermediate-risk localized prostate (Gleason ≤7, no ADT indication), this supports ultrahypofractionated SBRT as durable at 10 yr; it does not extend to high-risk or node-positive disease, where ADT and nodal coverage remain in play.
- SBRT monotherapy sufficiency for unfavorable intermediate-risk without ADT n=310 · primary completion 2025-12 · randomized SRT +/- ADT, unfavorable intermediate risk
- 10-yr randomized SBRT vs conventional EBRT outcomes n=503 · primary completion 2028-08 · SBRT vs standard RT: local control + bDFSrecruiting PRO-BOOST-LC: Whole-Gland Boost Strategies Versus SBRT Monotherapy in PSMA-Staged Localized and Locally Advanced Prostate Cancer Phase 2/3n=1200 · primary completion 2033-12 · randomized SBRT monotherapy vs EBRT-backbone boostrecruiting Testing Shorter Duration Radiation Therapy Versus the Usual Radiation Therapy in Patients With High Risk Prostate Cancer Phase 3n=1209 · primary completion 2036-03 · phase 3 SBRT 5fx vs usual 20-45fx EBRT
📚 Sources · 📄 1 paper
American Radium Society AUC: Intraprostatic Recurrence After RT
TL;DRPSMA PET + mpMRI plus mandatory pre-salvage biopsy, then reirradiation (≤6 fx) over ADT alone, for radiorecurrent intraprostatic disease.
RTOG 9408FORECAST
The RT-actionable read is workup discipline: mandatory biopsy before salvage (radiographic recurrence is often just treatment effect) and PSMA PET + mpMRI to exclude nodal/distant disease first. Preferred salvage is reirradiation in ≤6 fx over ADT alone, with short-course classic ADT (not ARSIs) for radiosensitization.
8 details 5 trials watching
ARS Genitourinary Appropriate Use Criteria consensus. PubMed + Embase across four topics (staging, biopsy, salvage modality, hormone therapy); evidence tables by 3 authors, panel voting via modified Delphi with RAND disagreement methodology.
Workup: PSMA PET + mpMRI to exclude metastatic disease and map local extent; biopsy mandatory before salvage to avoid treating radiographic changes that are only treatment effect. Salvage reirradiation preferred over noncurative ADT alone, most regimens ≤6 fractions; focal salvage when focal recurrence is confirmed, though whole-gland toxicity called very tolerable.
Evidence limited to pts initially treated with conventionally fractionated EBRT and worked up before the PSMA PET era; no randomized salvage trials, so recommendations rest on retrospective series and expert consensus.
| Modality | Sensitivity (95% CI) | Specificity (95% CI) |
|---|---|---|
| mpMRI (n=155) | 94% (88-98%) | 18% (7-35%) |
| MRI-targeted biopsy (n=87) | 92% (83-97%) | 75% (45-92%) |
In a man with biopsy-confirmed isolated intraprostatic recurrence after definitive RT (mets excluded on PSMA PET/mpMRI), this supports curative-intent local salvage over ADT alone; it does not extend to nodal or distant failure.
- Optimal salvage reirradiation modality and dose/fractionation n=60 · primary completion 2024-11 · randomises salvage EBRT vs HDR brachytherapyrecruiting Stereotactic Re-irradiation of Local Recurrences of Prostate Cancer After Radiotherapy Phase 2n=55 · primary completion 2029-12 · phase 2 focal SBRT reirradiation, GU/GI toxicity
- Focal vs whole-gland salvage for intraprostatic radiorecurrence n=50 · primary completion 2025-03 · focal salvage HDR brachy after definitive RTn=30 · primary completion 2032-01 · partial-gland (focal) salvage HDR after EBRT/LDR
- Salvage outcomes in the PSMA PET era recruiting Trial Evaluating the Safety and Efficacy Of MR-Linac-Guided Radiotherapy as Salvage Treatment After External Beam Radiotherapy Recurrence (TUMORNATOR II) Phase NAn=28 · primary completion 2028-08 · PSMA/PET MR-Linac salvage SBRT, radiorecurrent
📚 Sources · 📄 1 paper
NRG-GU005
ForLocalized intermediate-risk prostate cancer, definitive RT candidates
HR 1.38
95% CI 0.91-2.09, p=0.13; DFS superiority not met (futility crossed)
TL;DRDFS superiority not met (HR 1.38, futility crossed); SBRT improved 2y bowel QoL (35% vs 44% MCID decline, p=0.034) vs MH-IMRT.
Reported via UroToday →
The urinary-irritation co-primary SBRT was powered for came back flat (35% vs 34%, p=0.68); the QoL edge is bowel and incontinence, not irritation. DFS superiority failed and 3y biochemical failure ran numerically higher on SBRT (8% vs 4%), so the case for 5-fx SBRT is convenience and lower GU/bowel toxicity, not better control.
8 details 3 trials watching
Phase 3, randomized, non-blinded, international; N=698 (SBRT 353 / MH-IMRT 345). Co-primary: disease-free survival (superiority) and EPIC-26 bowel + urinary-irritation QoL at 24 mo. Interim futility analyses prespecified.
Localized intermediate-risk prostate cancer, median age 68. Stratified by Gleason score, PSA, and rectal manipulation (SpaceOAR in ~55%).
SBRT 36.25 Gy/5 fx (7.25 Gy/fx, 2-3×/wk) vs MH-IMRT 70 Gy/28 fx or 60 Gy/20 fx. CTV = prostate ±1 cm proximal SV; SBRT PTV margin 5 mm radial / 3 mm AP. Fiducials, MRI fusion, daily IGRT mandated.
Co-primary DFS powered for a 38% relative improvement (target HR 0.62). Co-primary QoL: absolute reduction in MCID for EPIC bowel (≥4) and urinary irritation/obstruction (≥5) at 24 mo.
DFS superiority not met (futility bound crossed); QoL split, bowel favored SBRT while urinary irritation did not. Effect sizes in the tables above.
| Endpoint | SBRT | MH-IMRT | Effect / p |
|---|---|---|---|
| 5y DFS | 89% (85-92%) | 92% (89-95%) | HR 1.38 (0.91-2.09), p=0.13 |
| 3y cum. biochemical failure | 8% (5.2-11.0) | 4% (2.3-7.0) | p=0.037 |
| 5y OS | 91% (85-95%) | 94% (90-97%) | p=0.66 |
| Domain · MCID decline | SBRT | MH-IMRT | p |
|---|---|---|---|
| Bowel, 2y | 35% | 44% | 0.034 |
| Urinary irritation/obstruction, 2y | 35% | 34% | 0.68 |
| Bowel, 1y | 33% | 46% | 0.002 |
| Sexual, 1y | 34% | 44% | 0.026 |
| Urinary incontinence, 2y | 26% | 35% | 0.023 |
| AE (any grade unless noted) | SBRT | MH-IMRT | p |
|---|---|---|---|
| G≥3 GU | 0.6% | 2.5% | 0.04 |
| Rectal hemorrhage | 10.5% | 17.3% | 0.01 |
| Fatigue | 39.2% | 50.8% | 0.0025 |
Investigator-reported toxicity favored SBRT: fewer G≥3 GU events, less rectal hemorrhage, less fatigue (all p<0.05). Table above.
Consistent with PACE-B: both show lower urinary-incontinence decline with SBRT vs MH-IMRT. MH-IMRT SOC anchored by RTOG 0415.
Non-blinded, so patient-reported QoL endpoints are unblinded. SBRT was designed to prove superiority and failed it; 3y biochemical failure ran numerically higher with SBRT.
Prespecified phase III; SBRT failed DFS superiority (futility crossed) and did not beat MH-IMRT on the urinary-irritation co-primary. Confirms SBRT as a safe equivalent option, not an upgrade.
In localized intermediate-risk prostate cancer weighing definitive RT fractionation, this supports 5-fraction SBRT as a shorter option with comparable disease control and a bowel and GU-toxicity edge over moderate hypofractionation; it does not establish SBRT as more effective.
- Durability of SBRT biochemical control beyond 3 years n=310 · primary completion 2025-12 · phase 3 prostate SBRT, bDFS primary endpoint
- Whether rectal spacer drives the bowel QoL benefit n=150 · primary completion 2027-09 · perirectal spacer efficacy in localized prostate RTn=500 · primary completion 2027-12 · SpaceOAR Vue for late GI toxicity in prostate SBRT
📚 Sources · 📄 2 papers
Abstract
Abstract
SUPREMO
ForpT1-2N1, pT3N0, or pT2N0 grade 3/LVI breast; post-mastectomy + systemic Rx
81.4% vs 81.9% (10-yr OS)
HR 1.04, 95% CI 0.82-1.30, P=0.80; did not meet OS
TL;DR10-yr OS 81.4% vs 81.9% (HR 1.04, P=0.80): chest-wall RT gives no OS benefit in intermediate-risk post-mastectomy breast cancer.
The RT read is local control without survival: CWI halved chest-wall recurrence (9 vs 20, HR 0.45) but the absolute gap stayed under 2 points and never reached OS or DFS. Fields were chest-wall-only (SCF 12%, IMC 1.5%), so this supports omitting CWI in intermediate-risk pN1 on modern systemic therapy, not nodal-RT calls.
Also covered Jul 9
8 details 5 trials watching
Phase 3 open-label RCT, 1:1, N=1607 ITT (808 CWI vs 799 no CWI) across 173 UK, European, and international sites. Median follow-up 9.6y, with 295 OS events (150 vs 145).
Intermediate-risk early breast: pT1N1, pT2N1, pT3N0, or pT2N0 with grade 3 and/or LVI. All had mastectomy, an axillary procedure, and adjuvant systemic therapy.
CWI 40-50 Gy to the chest wall. Supraclavicular fossa irradiated in only 97/808 CWI pts and IMC in 12/808 — this was chest-wall-only treatment, not comprehensive regional nodal RT.
Contemporary systemic backbone: 85% chemotherapy, 79% endocrine therapy, 19% trastuzumab.
OS, DFS, and DMFS were all null; the only endpoint favoring CWI was chest-wall recurrence (see table).
| Endpoint | CWI | No CWI | Effect |
|---|---|---|---|
| Overall survival | 81.4% | 81.9% | HR 1.04 (0.82-1.30), P=0.80 |
| Disease-free survival | 76.2% | 75.5% | HR 0.97 (0.79-1.18) |
| Distant MFS | 78.2% | 79.2% | HR 1.06 (0.86-1.31) |
| Chest-wall recurrence | 9 (1.1%) | 20 (2.5%) | HR 0.45 (0.20-0.99) |
EBCTCG PMRT meta-analysis (Lancet 2014) showed reduced recurrence and breast-cancer mortality in node-positive disease; SUPREMO finds no OS benefit in the intermediate-risk 1-3 node group treated in a modern systemic era.
Open-label; SCF/IMC coverage was sparse and non-standardized, so it does not test comprehensive regional nodal RT. Enrolment 2006-2013 predates some contemporary systemic regimens.
Adequately powered phase 3, prespecified OS endpoint, 10-yr f/u; null result diverges from EBCTCG-based routine PMRT for intermediate-risk 1-3 node disease.
In intermediate-risk post-mastectomy breast (pT1-2N1, pT3N0, or pT2N0 grade 3/LVI) on contemporary systemic therapy, this supports omitting chest-wall RT for survival; it does not extend to ≥4 positive nodes or to the comprehensive regional-nodal RT question.
- Does CWI omission hold in HER2+ and triple-negative intermediate-risk subgroups n=1106 · primary completion 2026-12 · phase 3 PMRT omission in pN1, 7y DFS non-inferiority
- Role of comprehensive regional nodal RT vs chest-wall-only in this population recruiting Evaluating Omitting of Internal Mammary Irradiation Among Early Stage Intermediate Risk (N1) Breast Cancer Phase NAn=214 · primary completion 2025-10 · omits IMN RT in N1 intermediate-riskactive Postmastecomy Internal Mammary Nodal Irradiation for High-risk Breast Cancer Patients Phase 3n=2400 · primary completion 2025-11 · phase 3 postmastectomy IMN RT vs none, DFSrecruiting The T-REX Trial: Tailored Regional External Beam Radiotherapy in Clinically Node-negative Breast Cancer Patients With 1-2 Sentinel Node Macrometastases. Phase NAn=1350 · primary completion 2028-12 · omits regional RT in 1-2 node macrometsrecruiting RecurIndex Guided Avoidance of Regional Nodal Irradiation for Node Positive Breast Cancer Phase NAn=540 · primary completion 2029-08 · RecurIndex-guided RNI vs none in N1
- Local control durability beyond 10 years
📚 Sources · 📄 1 paper
Abstract
ARTO NCT03449719
ForOligomet CRPC, ≤3 mets, no prior systemic mCRPC therapy, on abiraterone
TL;DRmOS NR vs 50mo, HR 0.55 (0.33-0.92, p=0.021) adding SBRT to all mets to abi+ADT in oligomet CRPC (unplanned OS analysis).
Ablative dose is the transferable read: BED ≥100 Gy in 1-5 fractions to ALL oligomet sites, and MDT added no excess grade 3-4 toxicity (the only treatment-related death was in the control arm). Extends the oligomet-MDT OS signal from hormone-sensitive disease into CRPC on an abiraterone backbone, informing whether to irradiate all sites when starting an ARSI.
Also covered Jun 12
9 details 4 trials watching
Phase 2, open-label, randomised 1:1, N=157, 16 Italian academic/community centres; stratified by centre, ECOG PS, and number of metastases. Median follow-up 53 mo (IQR 43-60). This OS read is an unplanned long-term analysis.
Prostate adenocarcinoma with metastatic castrate-resistant disease, ≤3 metastatic sites, and no prior systemic therapy for mCRPC. Control n=82, experimental n=75.
Both arms received ADT plus oral abiraterone acetate 1000 mg daily. The experimental arm added SBRT.
SBRT to all sites of metastatic disease, 1-5 fractions, biologically effective dose ≥100 Gy (ablative).
Primary: 6-month biochemical response (PSA drop ≥50%), previously met and reported. This paper reports an unplanned overall survival analysis at long-term follow-up.
OS median NR (95% CI 55-NR) experimental vs 50 mo (36-NR) control, HR 0.55 (0.33-0.92), p=0.021.
G3-4 infectious complications 5 (control) vs 0 (experimental); cardiovascular disorders 3 vs 3. One treatment-related death (myocardial failure) in the control arm. No excess toxicity from MDT.
Prior oligomet-MDT RCTs (STOMP, ORIOLE) enrolled castration-sensitive disease; ARTO extends the metastasis-directed RT signal into the CRPC setting on an ARSI backbone.
Unplanned OS analysis with post-hoc power recalculation; the trial was powered for 6-month biochemical response, not survival. Open-label, small N (157), phase 2.
Unplanned OS analysis (trial powered for 6-mo biochemical response, not survival); phase 2, N=157, open-label. Positive but hypothesis-generating pending a survival-powered phase 3.
In oligometastatic CRPC (≤3 sites, no prior systemic mCRPC therapy) starting abiraterone, this supports adding metastasis-directed SBRT; the signal does not extend to higher-volume mCRPC or the castration-sensitive oligomet setting.
- Does the OS benefit hold in a phase 3 powered for survival? recruiting Metastasis-directed Therapy in Oligoprogressive Castration-refractory Prostate Cancer Phase 3n=246 · primary completion 2029-01 · phase 3 MDT in oligoprogressive CRPC
- Optimal SBRT dose, fractionation, and site coverage in oligomet CRPC recruiting HIghly MetAstatic Life Prolonging Therapy-Resistant Prostate Cancer: Role of Stereotactic Radiotherapy for Bone and Lymph Node Metastases (HIMARS) Phase NAn=18 · primary completion 2028-05 · phase 1 SBRT max-tolerated-volume escalationrecruiting OligoCare TwiCs (Trials Within Cohorts) Trial Comparing Acute Toxicity in Single-fraction vs Multiple-fraction SBRT for Metastasis-directed Treatment (SPRINT) Phase NAn=302 · primary completion 2029-02 · single- vs multi-fraction SBRT for oligomets
- Which oligomet CRPC pts benefit most from MDT n=18 · primary completion 2023-07 · PSMA PET tests predictive value for MDT
📚 Sources · 📄 1 paper
Abstract
EORTC 22033-26033
ForHigh-risk WHO grade 2 low-grade glioma, first-line
No PFS or OS difference between arms
ns regardless of molecular subtype
TL;DRNo PFS/OS difference between first-line RT and TMZ in high-risk WHO grade 2 LGG; only IDH-wildtype favored TMZ (HR 0.47).
Upfront RT (28 × 1.8 Gy) and TMZ were survival-equivalent in every IDH-mutant subtype, including radiosensitive codeleted oligodendroglioma (OS 12.9 vs 14.9 yr, HR 0.88). The lone modality signal favored TMZ in IDH-wildtype (OS 4.7 vs 2.5 yr, HR 0.47), so molecular status, not modality, gates the first-line choice; combined-modality is now standard for IDH-mutant astrocytoma.
6 details 2 trials watching
Phase 3 RCT (EORTC 22033-26033 with NCIC-CTG/TROG/MRC-CTU), N=478 clinical high-risk WHO grade 2 LGG, randomized to RT vs dose-dense TMZ. Mature results, with post-hoc 2021 WHO molecular reclassification in 73% (351/478).
RT 28 × 1.8 Gy, standard fractionation, as the single-modality comparator arm.
Dose-dense TMZ 75 mg/m² once daily, 21 of 28 days, up to 12 cycles.
Primary: progression-free survival; overall survival co-reported. No significant difference in PFS or OS between arms.
Neither PFS nor OS differed by arm overall; molecular-subgroup OS is in the detail table, with only IDH-wildtype favoring TMZ.
| Subgroup (2021 WHO), n | RT OS | TMZ OS | HR (95% CI), p |
|---|---|---|---|
| Astrocytoma IDHmt non-codel, n=178 | 6.6-6.7 yr | 6.6-6.7 yr | HR CI 0.67-1.44, P=.93 |
| Oligo IDHmt codel, n=109 | 12.9 yr (9.4-NR) | 14.9 yr (10.1-NR) | 0.88 (0.52-1.49), P=.63 |
| IDH-wildtype, n=64 | 2.5 yr (1.8-3.3) | 4.7 yr (2.2-7.2) | 0.47 (0.27-0.82), P=.0068 |
Combined-modality (RT + chemo) was not tested here but has since become standard for IDH-mutant astrocytoma (e.g. RTOG 9802, RT+PCV).
Molecular subtypes are post-hoc reclassification (tissue in 73%); the IDH-wildtype subgroup is small (n=64). Combined-modality untested.
Mature phase 3; the null modality comparison confirms combined-modality's rise as SOC. Molecular subgroups reclassified post-hoc, so no single-modality practice change lands.
In high-risk WHO grade 2 IDH-mutant glioma, this supports that first-line RT versus TMZ monotherapy does not change PFS or OS; it does not extend to IDH-wildtype tumors, where a small post-hoc subgroup favored TMZ.
- Combined-modality vs single-modality first-line in IDH-mutant low-grade glioma active Radiation Therapy With or Without Temozolomide in Treating Patients With Low-Grade Glioma Phase 3n=540 · primary completion 2026-12 · phase 3 RT vs RT+TMZ, grade 2 glioma
- Does temozolomide outperform RT in IDH-wildtype grade 2 glioma? recruiting Chemotherapy and Radiation Therapy for the Treatment of IDH Wildtype Gliomas or Non-histological (Molecular) Glioblastomas Phase 2n=40 · primary completion 2026-12 · TMZ+RT in IDH-wildtype lower-grade glioma
📚 Sources · 📄 1 paper
Abstract
ReCOG/ESTRO/ASTRO HNSCC Reirradiation Consensus
TL;DRExpert consensus on reRT for recurrent/2nd-primary HNSCC in previously irradiated fields; 17-panel vote, guidance on selection, delineation, dose accumulation, toxicity.
The dose-accumulation and target-delineation domains are the real value: reRT toxicity is gated by cumulative OAR dose from the first course, and this is the first multi-society attempt to standardize how you sum the two plans and draw the reRT target. It sequences salvage surgery first, then postoperative or definitive reRT, so it shapes selection, not a dose prescription.
8 details 4 trials watching
Policy Review / expert-consensus statement. A 10-member core (6 radiation oncologists, 3 physicists, 1 research fellow) drafted, then an international panel of 17 radiation oncologists cast a single formal vote. Consensus predefined as high ≥85%, moderate 70-84%, low <70%, with no-opinion kept in the denominator.
Recurrent or second-primary HNSCC within a previously irradiated region, a setting with scarce options. Background: 15-50% of HNSCC pts recur or develop a second primary.
Covers definitive and postoperative reRT with modern conformal technique (IMRT, VMAT, proton, SBRT). Guidance spans patient selection, imaging, target delineation, treatment planning, dose accumulation, and toxicity management; salvage surgery preferred when feasible.
Evidence base is low-level (much at Oxford level 3-4, retrospective / expert consensus); single voting round with no reconciliation, and a radiation-oncologist-only panel.
In a pt with an in-field HNSCC recurrence or second primary (non-nasopharyngeal) being weighed for reRT, this frames selection, dose accumulation, and delineation; it does not extend to first-course or nasopharyngeal disease.
- Role of modern reRT (IMRT/proton/SBRT) undefined absent randomised trials active SBRT +/- Pembrolizumab in Patients With Local-Regionally Recurrent or Second Primary Head and Neck Carcinoma Phase 2n=86 · primary completion 2027-07 · phase 2 SBRT reRT +/- pembrolizumabrecruiting Prospective Evaluation of Pencil Beam Scanning Proton Therapy for Previously Irradiated Tumors Phase NAn=1800 · primary completion 2028-01 · prospective PBS proton reRT, prior-irradiatedrecruiting Carbon Ion Re-Radiotherapy in Patients With Recurrent or Progressive Locally Advanced Head-and-Neck Cancer Phase NAn=72 · primary completion 2030-07 · randomised carbon ion vs photon reRTrecruiting Re-Radiochemotherapy and Pembrolizumab vs. Immuno(Chemo)Therapy for Locoregionally Recurrent PD-L1 Positive (CPS≥1) HNSCC Phase 3n=214 · primary completion 2032-12 · phase 3 randomised reRCT vs pembrolizumab
- Optimal dose accumulation method across two RT courses
- Selection for definitive vs postoperative reRT
📚 Sources · 📄 1 paper
NRG/RTOG 1112 NCT01730937
ForLocally advanced HCC, macrovascular invasion (74%), 1L systemic candidates
15.8 vs 12.3 mo
HR 0.77 (90% CI 0.59-1.01), 1-sided P=.06, ns; adjusted HR 0.72, P=.04
TL;DRAdding SBRT to sorafenib: mOS 15.8 vs 12.3mo (HR 0.77, 1-sided P=.06, ns primary); mPFS 9.2 vs 5.5mo, HR 0.55, P<.001.
The RT read is PFS, not the ns OS primary: mPFS 9.2 vs 5.5mo (HR 0.55, P<.001), a locoregional-control signal in a cohort 74% macrovascular-invasion, where liver-directed RT is hardest. Personalized 27.5-50Gy/5fx, no excess G3+ toxicity. Open decision: does SBRT still add over a modern IO backbone (sorafenib obsolete)?
8 details 3 trials watching
Phase 3 open-label RCT, 1:1, 193 randomized (177 eligible), stratified by performance status, liver function, degree of metastases, and macrovascular invasion. Accrual stopped early after first-line systemic SOC shifted.
Locally advanced HCC unsuitable for or refractory to standard locoregional therapy, fit for first-line systemic. 84.7% male, median age 66; macrovascular invasion in 74%.
Personalized SBRT, 27.5 to 50 Gy in 5 fractions, dose adapted to liver function, delivered before sorafenib.
Primary: overall survival. Secondary: progression-free survival, adverse events, quality of life.
Primary OS trend favored SBRT but missed the prespecified 1-sided threshold (P=.06); stratification-adjusted OS and the secondary PFS were both significant. See the endpoint table.
| Endpoint | SBRT+sorafenib | Sorafenib | Effect (HR/P) |
|---|---|---|---|
| mOS | 15.8 mo | 12.3 mo | HR 0.77 (90% CI 0.59-1.01), 1-sided P=.06 |
| mPFS | 9.2 mo | 5.5 mo | HR 0.55 (0.40-0.75), P<.001 |
| G3+ TRAE | 47% (39/83) | 42% (37/88) | P=.52 |
G3+ treatment-related AEs similar (47% vs 42%, P=.52). Treatment-related deaths: 2 with sorafenib (liver failure, death NOS), 1 with SBRT+sorafenib (lung infection). No excess RT-attributable toxicity.
Predates modern first-line combinations (atezolizumab-bevacizumab, durvalumab-tremelimumab); the sorafenib-alone comparator is now obsolete, leaving open whether SBRT adds over an IO backbone.
Open-label; accrual stopped early (underpowered); primary OS not significant unadjusted; comparator superseded; QoL assessed in small subsets (n=17-20).
Randomised phase 3 argues for adding SBRT to systemic in MVI-heavy HCC, but primary OS not significant (1-sided P=.06), stopped early, sorafenib comparator obsolete.
In locally advanced HCC with macrovascular invasion refractory to or unsuitable for standard locoregional therapy, this supports adding SBRT to first-line systemic as contested evidence; it does not establish benefit over a modern IO-based first-line backbone.
- Does SBRT add over modern IO-based first-line systemic therapy? recruiting Testing Immunotherapy With or Without Stereotactic Body Radiation Therapy in Patients With Advanced Liver Cancer, HELIO-RT Trial Phase 3n=226 · primary completion 2029-03 · phase 3 IO+SBRT vs IO alone
- Optimal SBRT dose and fractionation with impaired liver function recruiting A Pilot Study of Liver Protection Using Prednisone for Patients Receiving Stereotactic Body Radiation Therapy for Hepatocellular Carcinoma Phase 2n=20 · primary completion 2026-08 · prednisone liver-protection during SBRTn=18 · primary completion 2026-12 · phase 1 repeated-dose SBRT dose escalation
📚 Sources · 📄 1 paper
Abstract
BART
ForHigh-risk (T3-4/N+/R+) MIBC, post-cystectomy + chemo, no immunotherapy
HR 0.43
95% CI 0.20-0.96, p=0.04; 2y LRFFS 87.1% vs 76.0% (ITT)
TL;DR2y locoregional FFS 87.1% vs 76.0% (HR 0.43, p=0.04) with adjuvant pelvic RT post-cystectomy; OS not significant (HR 0.78, p=0.31).
Reported via UroToday →
The LRFFS benefit concentrates in the pN+ and T3+ subgroups (2y HR 0.22 and 0.25), and per-protocol it widens to HR 0.27 (93.2% vs 75.0%) once the 14 who never received RT are analysed as observation. Standard 50.4Gy/28fx to bed plus pelvic nodes transfers directly, so this moves the adjuvant-pelvic-RT decision for node-positive or margin-positive disease.
9 details 2 trials watching
Phase 3 multicentre RCT, 1:1, N=153 (RT 77 / obs 76), enrolled 2016-2024, stratified by nodal stage (N0/N+) and chemotherapy. Median follow-up 47 mo. Underpowered: accrual fell short of the sample-size goal.
High-risk (T3-4, N1-3, or R+) non-metastatic urothelial MIBC after radical cystectomy. 62% pT3-4, 41% pN+, 28% variant-histology component; median age 57, median 20 nodes dissected, 4.6% positive margins, 2.6% neobladder.
50.4 Gy / 28 fx to cystectomy bed plus pelvic nodes (common / internal / external iliac, presacral, obturator). Stoma- and bowel-sparing IMRT with daily onboard image guidance.
Primary: 2-year locoregional failure-free survival. Secondary: bladder-cancer-specific survival, DFS, overall survival. Fine-Gray competing-risk analysis (distant mets, non-cancer death).
Primary met; the time-to-event secondaries (DFS, BCSS, OS) all favoured RT numerically but none reached significance.
| Endpoint (2y) | Adjuvant RT | Observation | HR (95% CI), p |
|---|---|---|---|
| LRFFS (ITT) | 87.1% | 76.0% | 0.43 (0.20-0.96), p=0.04 |
| LRFFS (per-protocol) | 93.2% | 75.0% | 0.27 (0.10-0.71), p=0.008 |
| DFS | 71.6% | 58.7% | 0.62 (0.36-1.05), p=0.07 |
| BCSS | 79.6% | 65.0% | 0.59 (0.33-1.10), p=0.09 |
| OS | 70.4% | 57.4% | 0.78 (0.49-1.26), p=0.31 |
| Subgroup | HR (95% CI) |
|---|---|
| T3+ and N+ | 0.25 (0.07-0.84) |
| N+ disease | 0.22 (0.06-0.75) |
| Adverse event | Adjuvant RT | Observation |
|---|---|---|
| Late G3+ | 8.4% | 10.5% (p=0.60) |
| Acute G3 GI | 1.6% | 4.1% |
| Acute G2 GI | 17.5% | 1.4% |
Late grade 3+ toxicity comparable between arms; acute grade 2 GI higher with RT while grade 3 GI was lower, with no toxicity-related discontinuation.
Adjuvant RT after cystectomy is not routine (historic locoregional recurrence ~30% in high-risk pts); BART is the largest RCT in this space. A planned MERCY individual-patient-data meta-analysis will test the OS question.
Underpowered, OS not significant (HR 0.78, p=0.31) on a locoregional surrogate primary. 14/77 RT-arm pts never received RT, so the ITT HR (0.43) understates the per-protocol effect (HR 0.27). No immunotherapy used.
Randomised phase III, prespecified 2y LRFFS primary hit, diverging from the current no-adjuvant-RT norm. Underpowered and OS not significant, so short of practice-changing.
In pN+ or margin-positive high-risk MIBC after cystectomy and cisplatin chemo, this supports weighing adjuvant pelvic RT for locoregional control; it does not establish an OS benefit and does not extend to low-risk node-negative, margin-negative disease.
- OS benefit of adjuvant RT (planned MERCY IPD meta-analysis) n=76 · primary completion 2018-10 · adjuvant EBRT post-cystectomy, ≥pT3 high-riskactive Adjuvant Radiotherapy in Patients With Pathological High-risk Bladder Cancer (GETUG-AFU 30) Phase NAn=81 · primary completion 2027-12 · randomised adjuvant pelvic RT post-cystectomy, survival
- Adjuvant RT plus immunotherapy after cystectomy
📚 Sources · 📄 1 paper
Abstract
DOREMY NCT02106312
ForLocalized translocation-confirmed myxoid liposarcoma, trunk/extremity
TL;DR5yr local recurrence-free survival 97.4% after de-escalated 36Gy/18fx preop RT in myxoid liposarcoma; wound complications 21%.
The RT read is dose de-escalation: 36Gy/18fx (vs the standard 50Gy/25fx) held 5yr LRFS at 97.4% in translocation-confirmed MLS, with wound complications 21% and G3 late toxicity 3%. Exploiting MLS radiosensitivity trims ~14Gy without a local-control cost, moving the preop-dose decision for this histology specifically.
7 details 4 trials watching
Phase 2 single-group nonrandomized trial, N=90, 9 tertiary sarcoma centers (Europe + US), enrolled 2010-2020. Median follow-up 66.4 mo (IQR 48.8-87.5).
Adults with biopsy-proven, translocation-confirmed localized MLS of trunk or extremity. Mean age 47, 56% male.
36 Gy in once-daily 2-Gy fractions (18 fx) preoperatively, against the standard 50 Gy/25 fx for soft-tissue sarcoma. Delivered per protocol in all 90 pts, then resection.
5yr LRFS 97.4% (95% CI 93.9-100) is the standout; PFS 81.0%, DSS 89.5%, OS 88.5% (full set in table). 3 pts (3%) progressed to metastasis before surgery.
| Endpoint (5yr) | Rate | 95% CI |
|---|---|---|
| Local recurrence-free survival | 97.4% | 93.9-100 |
| Progression-free survival | 81.0% | 72.6-89.4 |
| Disease-specific survival | 89.5% | 82.6-96.4 |
| Overall survival | 88.5% | 81.2-95.8 |
Wound complications in 18 pts (21%), 14 (16%) needing intervention. Late toxicity: G2 in 13 (15%), G3 in only 3 (3%).
Standard preoperative dose for soft-tissue sarcoma is 50 Gy/25 fx. MLS is highly radiosensitive, which motivates cutting ~14 Gy to 36 Gy while preserving local control.
Single-arm, no randomized comparator vs 50 Gy; equivalence inferred, not proven. Rare cancer makes a phase 3 impractical (authors' argument).
Single-arm nonrandomized phase 2; no randomized comparator vs standard 50Gy. Long follow-up, but efficacy equivalence is inferred, not tested. Single-arm design caps the read.
In localized, translocation-confirmed myxoid liposarcoma of the trunk or extremity, this supports reduced-dose 36Gy preop RT as an option; it does not extend to other soft-tissue sarcoma histologies that lack this radiosensitivity.
- Non-inferiority vs standard 50Gy preop RT unproven n=300 · primary completion 2031-01 · prospective MLS registry: 36Gy vs 50Gy preop RT
- Generalizability to non-myxoid soft-tissue sarcoma histologies n=15 · primary completion 2027-05 · hypofrac preop RT in mixed extremity/trunk STSn=150 · primary completion 2028-11 · 14x3Gy hypofrac preop RT across STS histologiesrecruiting Assessment of the Long-term Efficacy of Moderately Hypofractionated Neoadjuvant Radiotherapy Soft Tissue Sarcoma in the Limbs or Trunk Wall Phase 2n=135 · primary completion 2032-06 · mod-hypofrac neoadj RT, all STS grades, LC endpoint
📚 Sources · 📄 1 paper
Abstract
GEC-ESTRO APBI Patient Selection Recommendations
TL;DRExpanded APBI eligibility: now unifocal/multifocal ≤2cm, pTis/T1-2 ≤30mm, pN0/pN1mi, all histologies; BRCA1-2, TNBC, ≥pN1a, age <40 contraindicated.
The expansion is the actionable read: pN1mi, multifocal ≤2cm, DCIS (pTis), and all histologies now qualify as good APBI candidates, widening who you can offer partial-breast over whole-breast RT. BRCA1-2 carriers, TNBC, ≥pN1a nodes, and age <40 stay hard contraindications.
5 details 5 trials watching
Systematic review with consensus recommendations. PubMed/Medline/Scopus/Cochrane searched 2010-2024; 618 articles screened to 10 prospective RCTs and 7 retrospective comparative studies (median follow-up ≥5 yr), then supplemented with expert opinion.
Consensus, not a comparative trial: the eligibility expansion blends RCT evidence with expert opinion, with no randomized test of expanded vs restrictive criteria. Patient selection only, no APBI dose, fractionation, or modality specified.
| Criterion | Low-risk (good APBI candidate) | High-risk (contraindicated) |
|---|---|---|
| Age | >40 yr | <40 yr |
| Tumor | Unifocal/multifocal ≤2cm; pTis, T1-2 ≤30mm | Multicentric or >30mm |
| Nodal | pN0 or pN1mi | ≥pN1a, or pNx (unknown status) |
| Histology | All types | Triple-negative |
| Margins | Negative (≥2mm for DCIS) | Positive (<2mm for DCIS) |
| EIC / LVI | Absent | EIC+ or extensive LVI |
| BRCA1-2 | Non-carrier | Mutation carrier |
In a woman >40 with T1-2 ≤30mm, pN0/pN1mi, margin-negative breast cancer of any histology, this supports offering APBI over whole-breast RT; it does not extend to BRCA carriers, TNBC, ≥pN1a disease, or age <40.
- Long-term outcomes in newly eligible groups (pN1mi, multifocal, DCIS) n=139 · primary completion 2025-12 · 10y local/regional recurrence registry, incl DCISn=250 · primary completion 2027-07 · enrolls pN1mi; clinical outcomes + late toxicityrecruiting Single-fraction APBI for Early-stage Breast Cancer With Favorable Histological Subtypes (Breast-1F) Phase NAn=311 · primary completion 2029-06 · single-fraction non-inferiority RCT incl pTis/DCIS
- Optimal APBI modality and dose for expanded-eligibility patients n=121 · primary completion 2029-03 · head-to-head IORT/brachy/3D-CRT/SBRT APBIactive PBI for Breast in Situ Carcinoma of Intermediate Low Risk As Local Adjuvant Treatment Phase NAn=150 · primary completion 2029-12 · EBRT vs brachytherapy for low/intermed DCIS
📚 Sources · 📄 1 paper
Abstract
ORIOLE NCT02680587
ForRecurrent HSPC, 1-3 conventional-imaging mets, off ADT ≥6mo
19% vs 61%
P=.005; SABR vs observation
TL;DR6-mo progression 19% vs 61% favoring SABR (P=.005); mPFS NR vs 5.8mo, HR 0.30 (0.11-0.81) in oligomet HSPC.
Surfaced from a review's discussed trials
The RT read is completeness, not SABR alone: among SABR pts, leaving any PSMA-avid lesion untreated collapsed DMFS to 6.0 vs 29.0 mo (HR 0.19, 0.07-0.54). Conventional imaging under-stages, so PSMA-PET staging plus total consolidation, not partial MDT, is the decision this moves. SABR dose/fractionation not reported in source.
9 details 5 trials watching
Phase 2 randomized trial, 2:1 SABR vs observation, N=54 at 3 US radiation centers. Primary: composite progression at 6 mo. Median follow-up 18.8 mo.
Recurrent hormone-sensitive prostate cancer, 1-3 asymptomatic mets ≤5 cm on conventional imaging, prior definitive treatment of the primary. No ADT within 6 mo. Median age 68.
SABR to all conventional-imaging metastases; PSMA-PET obtained but blinded to planning. Dose/fractionation not reported in source. Local control 98.9% at 6 mo.
Because PET was blinded, 16/36 SABR pts had untreated PET-avid lesions; any untreated lesion collapsed DMFS to 6.0 vs 29.0 mo (HR 0.19). Total consolidation, not SABR per se, drove the benefit.
Concordant with STOMP (phase 2 MDT in oligomet PC): both show metastasis-directed therapy delays progression and defers ADT. The pooled ORIOLE+STOMP analysis reinforced the signal.
Phase 2, N=54; composite surrogate primary read at 6 mo, not OS-powered. Open-label observation control. Conventional-imaging staging misses PET-avid disease.
| Endpoint | SABR | Observation | Effect |
|---|---|---|---|
| 6-mo progression (composite) | 7/36 (19%) | 11/18 (61%) | P=.005 |
| 6-mo PSA progression | 4/36 (11%) | 9/18 (50%) | P=.005 |
| Median PFS | Not reached | 5.8 mo | HR 0.30 (0.11-0.81), P=.002 |
| Median biochemical PFS | Not reached | 6.4 mo | HR 0.31 (0.13-0.75), P=.002 |
| Endpoint | No untreated | Any untreated | Effect |
|---|---|---|---|
| 6-mo progression | 1/19 (5%) | 6/16 (38%) | P=.03 |
| Median PFS | Not reached | 11.8 mo | HR 0.26 (0.09-0.76), P=.006 |
| New mets 180d | 3/19 (15.8%) | 10/16 (62.5%) | P=.006 |
| DMFS | 29.0 mo | 6.0 mo | HR 0.19 (0.07-0.54), P<.001 |
Phase 2, N=54; composite progression primary read at only 6mo. Randomised but small, short f/u. Concordant with STOMP MDT signal; awaits phase 3.
In recurrent HSPC with 1-3 conventional-imaging mets and off ADT ≥6mo, this supports metastasis-directed SABR to defer systemic therapy; it does not extend to higher-volume or castration-resistant disease.
- Overall survival benefit of metastasis-directed SABR recruiting Stereotactic Ablative Radiotherapy (SABR) for the Treatment of Patients With Metastatic Cancer, ID-COMET Trial Phase 3n=800 · primary completion 2032-09 · phase 3 SABR vs 3-mo delay, survival endpoint
- Role of PSMA-PET staging before consolidative SABR n=140 · primary completion 2025-05 · PSMA vs fluciclovine PET for RT planningactive Multicenter Randomized Trial of 68Ga-PSMA-11 PET/CT Based SRT After Radical Prostatectomy Phase 3n=193 · primary completion 2027-07 · randomized 68Ga-PSMA PET-guided RT vs standard
- SABR benefit in higher-volume or ADT-dependent disease active Androgen Deprivation Therapy for Oligo-recurrent Prostate Cancer in Addition to radioTherapy Phase 3n=280 · primary completion 2027-10 · phase 3 MDRT ± ADT vs MDRT alone, MPFSrecruiting HIghly MetAstatic Life Prolonging Therapy-Resistant Prostate Cancer: Role of Stereotactic Radiotherapy for Bone and Lymph Node Metastases (HIMARS) Phase NAn=18 · primary completion 2028-05 · SBRT volume-escalation in high-volume mets
📚 Sources · 📄 1 paper
Abstract
WOLVERINE
ForOligometastatic prostate cancer (≤5 mets), predominantly castration-sensitive
TL;DRPFS HR 0.44, rPFS HR 0.60 favor MDT added to SOC in oligomet prostate; OS HR 0.63 non-sig (p=0.051).
Surfaced from a review's discussed trials
MDT here is predominantly SBRT, and the RT-attributable read is that benefit held in the sensitivity analysis excluding observation-only-SOC trials (PFS HR 0.46, CRFS HR 0.46), so MDT adds on a systemic backbone, not just vs nothing. OS stayed non-significant (HR 0.63, p=0.051): the gain is delaying progression and castration resistance, not proven survival.
7 details 5 trials watching
IPD meta-analysis (PROSPERO CRD42023479078) of 7 phase 2 RCTs; the primary MDT-efficacy analysis pooled 6 trials randomizing 472 men to MDT+SOC (n=248) vs SOC (n=224). Median follow-up 40.7 mo (IQR 25.6-53.7).
Oligometastatic (up to 5 mets) prostate cancer; 65% castration-sensitive (n=375), ARTO entirely CRPC and EXTEND baskets CRPC-enriched. 85.5% (n=491) had prior definitive local therapy; median PSA 1.9 both arms.
MDT is delivered per each component trial (EXTEND, STOMP, ORIOLE, ARTO, COMET-SABR), predominantly SBRT-based. Dose, fractionation, target volume, and modality breakdown are not reported in this meta-analysis, so the technique-transfer question can't be answered from source.
Coprimary: PFS and OS. Secondary: rPFS and castration resistance-free survival (CRFS).
MDT plus SOC improved PFS, rPFS, and CRFS across both trial- and patient-level analyses; overall survival did not reach significance (effect sizes in the table above).
STOMP and ORIOLE (observation-controlled SBRT trials) drove the early MDT signal; this pooled IPD extends the PFS/CRFS benefit across 6 trials and shows it persists on a systemic-therapy backbone in the observation-excluded sensitivity analysis.
All 7 component trials are phase 2 with non-blinded randomization ('some concerns' RoB) and open-label PSA-driven endpoints. OS non-significant (p=0.051). SOC arm slightly older (71 vs 68) and more often on 2nd-gen ARPI (59.8% vs 50.4%).
IPD meta-analysis of 6 phase-2 non-blinded RCTs; PFS/rPFS/CRFS clearly hit but OS non-significant. Reinforces the emerging MDT-for-oligomet signal (STOMP, ORIOLE), doesn't establish survival.
In castration-sensitive oligometastatic prostate cancer, up to 5 mets and mostly post definitive local therapy, the pooled evidence supports MDT plus SOC to delay progression and castration resistance; it does not establish a survival benefit nor extend to the CRPC-predominant setting.
- Does MDT extend overall survival in oligometastatic prostate cancer? active Prostate-cancer Treatment Using Stereotactic Radiotherapy for Oligometastases Ablation in Hormone-sensitive Patients Phase 3n=550 · primary completion 2026-06 · phase 3 SBRT + SOC vs SOC in oligomet HSPCrecruiting Veterans Affairs Seamless Phase II/III Randomized Trial of STAndard Systemic theRapy With or Without PET-directed Local Therapy for Oligometastatic pRosTate Cancer Phase 2/3n=464 · primary completion 2026-09 · phase 2/3 systemic ± PET-directed local therapy
- Optimal MDT (SBRT) target volume and dose across trials recruiting HIghly MetAstatic Life Prolonging Therapy-Resistant Prostate Cancer: Role of Stereotactic Radiotherapy for Bone and Lymph Node Metastases (HIMARS) Phase NAn=18 · primary completion 2028-05 · phase 1 max-tolerated-volume SBRT escalationrecruiting OligoCare TwiCs (Trials Within Cohorts) Trial Comparing Acute Toxicity in Single-fraction vs Multiple-fraction SBRT for Metastasis-directed Treatment (SPRINT) Phase NAn=302 · primary completion 2029-02 · single- vs multi-fraction SBRT for mets
- MDT benefit in CRPC vs castration-sensitive disease recruiting Metastasis-directed Therapy in Oligoprogressive Castration-refractory Prostate Cancer Phase 3n=246 · primary completion 2029-01 · phase 3 MDT in oligoprogressive CRPC
📚 Sources · 📄 1 paper
Abstract
ARTO NCT03449719
ForOligometastatic CRPC, ≤3 nonvisceral mets, first-line abiraterone
92% vs 68.3%
OR 5.34 (95% CI 2.05-13.88), P=.001
TL;DRAdding SBRT to abiraterone lifted 6-mo PSA response to 92% vs 68.3% (OR 5.34) and cut progression (PFS HR 0.35) in oligomet CRPC.
Surfaced from a review's discussed trials
The RT read is total metastatic consolidation: SBRT to all ≤3 CRPC sites concurrent with abiraterone more than doubled complete PSA response (56% vs 23.2%) and cut progression risk (HR 0.35). It pushes MDT beyond hormone-sensitive oligomet (ORIOLE/STOMP) into first-line CRPC, moving the decision to irradiate every lesion, not defer.
Also covered Jul 7
6 details 5 trials watching
Multicenter randomized phase II, 1:1, N=157, enrolled Jan 2019-Sep 2022. Primary: 6-month biochemical response.
Oligometastatic castration-resistant prostate cancer with ≤3 nonvisceral metastatic lesions, in the first-line abiraterone setting.
Both arms received abiraterone acetate + prednisone (AAP). The experimental arm added concomitant SBRT.
SBRT to all sites of disease, concomitant with AAP. Dose/fractionation not reported in source.
Primary: biochemical response (PSA drop ≥50% at 6mo). Secondary: complete BR (PSA <0.2 ng/mL), PFS.
Primary endpoint and PFS both met, favoring the SBRT arm (see results table).
| Endpoint (6mo) | AAP+SBRT | AAP alone | Effect size |
|---|---|---|---|
| Biochemical response (PSA ≥50% drop) | 92% | 68.3% | OR 5.34 (2.05-13.88), P=.001 |
| Complete BR (PSA <0.2 ng/mL) | 56% | 23.2% | OR 4.22 (2.12-8.38), P<.001 |
Extends the metastasis-directed SBRT benefit seen in ORIOLE/STOMP (hormone-sensitive oligomet) into first-line CRPC.
Phase II, N=157. Primary endpoint is a PSA surrogate with no OS reported; dose/fractionation and long-term durability not in source.
Randomized phase II, primary hit, named comparator (AAP alone); primary is a PSA surrogate, so supportive of the emerging oligomet MDT paradigm rather than practice-setting.
In oligometastatic CRPC (≤3 nonvisceral mets) starting first-line abiraterone, this supports adding SBRT to all sites for deeper PSA response and longer PFS; it does not extend to visceral or polymetastatic disease.
- OS benefit of adding SBRT in oligomet CRPC recruiting Metastasis-directed Therapy in Oligoprogressive Castration-refractory Prostate Cancer Phase 3n=246 · primary completion 2029-01 · phase 3 MDT vs SOC in oligoprogressive CRPCrecruiting Treatment With Darolutamide +/- Radiation Therapy for Patients With a Castration Resistant Cancer and Metastases Detected by Functional Imaging Phase 3n=336 · primary completion 2029-10 · phase 3 darolutamide ± SBRT in metastatic CRPC
- Optimal SBRT dose/fractionation for CRPC metastases recruiting OligoCare TwiCs (Trials Within Cohorts) Trial Comparing Acute Toxicity in Single-fraction vs Multiple-fraction SBRT for Metastasis-directed Treatment (SPRINT) Phase NAn=302 · primary completion 2029-02 · single- vs multi-fraction SBRT for oligomets
- Does MDT delay next systemic therapy in CRPC? n=102 · primary completion 2027-04 · SBRT to postpone 2nd-line systemic tx in CRPCn=66 · primary completion 2030-11 · SBRT + darolutamide to defer 2nd-line in M0CRPC
📚 Sources · 📄 1 paper
Abstract
EAU 2026: What Evidence Do We Have from Intensification with SBRT?
TL;DRMDT/SBRT delays progression in oligorecurrent HSPC; ARTO the lone randomized OS signal (CRPC); de novo evidence pending (STAMPEDE2).
Reported via UroToday →
The RT-actionable split is by oligomet state: MDT/SBRT evidence is strongest in metachronous oligorecurrence (STOMP, ORIOLE), while de novo rests on pending RCTs (STAMPEDE2, PLATON, OLIGOPRESTO). ARTO is the lone randomized OS signal, but in castration-resistant disease. Adding Ra-223 to MDT (RAVENS) gave no PFS/MFS benefit.
9 details 5 trials watching
- 🔍 EAU 2026 thematic session (V. Fonteyne, Ghent radonc): MDT/SBRT evidence across oligometastatic prostate cancer states
- 🔍 Most evidence is metachronous oligorecurrent HSPC; de novo / synchronous evidence remains thin
- 🔍 De novo oligomet RCTs pending: STAMPEDE2 (SBRT), PLATON, TERPS, OLIGOPRESTO
- 💊 De-escalation: SOLAR (n=21, synchronous) tested stopping ADT post-MDT, more favorable than SATURN (metachronous); hypothesis-generating
- 🔍 LUNAR (Lu-177) ongoing in the same MDT-plus-radioligand question
- 🔍 Selection debated: ≤5-lesion cutoff crude; PSMA PET burden (PP3) + biomarkers proposed to refine
- 📊 MDT trial landscape by oligometastatic setting (directional; no effect sizes reported in source)
Trial Setting Key finding STOMP + ORIOLE Metachronous oligorecurrent HSPC Excellent local control, delayed progression, minimal toxicity RADIOSA Oligomet HSPC ADT + MDT improved PFS vs MDT alone WOLVERINE Oligometastatic HSPC MDT improved PFS + rPFS, delayed CRPC; OS not significant ARTO Oligometastatic CRPC MDT + SOC improved PFS; signal for OS + PCSS RAVENS Oligometastatic Ra-223 + MDT: no PFS or MFS benefit - 📊 RAVENS: adding Ra-223 to MDT improved neither PFS nor MFS vs MDT alone
- ⚠️ Small trials, heterogeneous inclusion + endpoints; guideline integration remains difficult
In metachronous oligorecurrent HSPC with ≤5 lesions, the evidence supports SBRT-MDT to delay systemic therapy; it does not yet extend to de novo synchronous oligomets, where randomized data (STAMPEDE2, OLIGOPRESTO) are pending.
- Optimal patient selection for MDT beyond lesion count
- MDT benefit in de novo synchronous oligometastatic HSPC recruiting Veterans Affairs Seamless Phase II/III Randomized Trial of STAndard Systemic theRapy With or Without PET-directed Local Therapy for Oligometastatic pRosTate Cancer Phase 2/3n=464 · primary completion 2026-09 · randomized SST +/- local therapy, de novo armrecruiting MDRT in Prostate Cancer Treated With Long-term Androgen Deprivation Therapy in the STAMPEDE Trial (METANOVA) Phase 2n=200 · primary completion 2028-12 · MDRT at diagnosis (synchronous), phase 2 vs ADTrecruiting Metastasis Directed Stereotactic Body Radiotherapy for Oligo Metastatic Hormone Sensitive Prostate Cancer Phase NAn=118 · primary completion 2031-12 · phase 3 MD-SBRT, incl de novo oligomet HSPC arm
- Whether radioligand therapy added to MDT improves outcomes n=107 · primary completion 2030-10 · 225Ac vs 177Lu-PSMA added to SBRT, oligomet PCaactive 177-Lutetium-PSMA Before Stereotactic Body Radiotherapy for the Treatment of Oligorecurrent Prostate Cancer, The LUNAR Study Phase 2n=93 · primary completion 2032-09 · 177Lu-PSMA before SBRT, control rate EP (LUNAR)
📚 Sources · 📄 1 paper
Abstract
NRG Oncology/RTOG 0848 NCT01013649
ForResected pancreatic head adenocarcinoma, post adjuvant gemcitabine-based chemo
HR 0.96
90% CI 0.79-1.18, p=0.38 (1-sided log-rank); primary OS endpoint not met
TL;DROS HR 0.96 (90% CI 0.79-1.18), p=0.38: adjuvant chemoRT adds no OS benefit over chemo alone after pancreatic head resection.
The RT read is the node-negative subgroup: 5-yr OS 28.6→48.1% and median OS 3.0→3.9 yr with added CXRT (interaction p=0.022), while node-positive pts gained nothing (21.2 vs 20.9%). Subgroup-only (n=91), but it isolates who might still warrant adjuvant CXRT once modern systemic therapy is optimized.
7 details 3 trials watching
RT randomization of NRG/RTOG 0848 phase 3. After curative-intent resection and adjuvant gemcitabine-based chemo without progression, N=354 randomized to no further therapy (n=174) vs fluoropyrimidine-sensitized CXRT (n=180). Primary: overall survival.
Resected pancreatic head adenocarcinoma; mix of N0 (n=91) and N1 (n=263), predominantly T3 (n=288 vs T1/T2 n=66), mostly negative margins (n=295). Only pts completing adjuvant chemo without progression.
Adjuvant systemic backbone gemcitabine-based: gemcitabine alone (n=236), non-oxaliplatin gemcitabine combinations (n=18), gemcitabine+erlotinib (n=100). Added arm was fluoropyrimidine-sensitized CXRT.
CXRT was fluoropyrimidine-sensitized chemoradiotherapy delivered after completion of adjuvant chemo. RT dose, fractionation, and target volume not reported in source text.
Primary: overall survival. Prespecified 5-yr OS subgroup estimates with interaction tests by nodal status, T stage, margins, CA19-9, sex, age, and systemic regimen.
Primary OS negative: HR 0.96 (90% CI 0.79-1.18), p=0.38; median OS 2.6 vs 2.3 yr. Nodal-status interaction p=0.022 with a node-negative gain (see table).
| Nodal status | Chemo 5-yr OS | Chemo+CXRT 5-yr OS |
|---|---|---|
| N0 (n=91) | 28.6% (14.9-42.2) | 48.1% (33.3-62.9) |
| N1 (n=263) | 21.2% (13.8-28.5) | 20.9% (13.8-28.0) |
| Endpoint | Chemo | Chemo+CXRT |
|---|---|---|
| Median OS | 3.0 yr (2.2-4.0) | 3.9 yr (2.5-NR) |
| Median DFS | 1.5 yr (0.8-2.7) | 2.3 yr (1.4-NR) |
Gemcitabine backbone predates FOLFIRINOX-era adjuvant standard; authors note the node-negative signal needs confirmation in trials using FOLFIRINOX/FOLFOXIRI.
Node-negative OS benefit is a subgroup finding (n=91, interaction p=0.022), hypothesis-generating. Dated gemcitabine backbone; RT technique not reported in source.
Prospective phase III, primary OS endpoint not met (HR 0.96); reinforces omitting adjuvant CXRT. Node-negative benefit is subgroup-only (interaction p=0.022), needs independent confirmation.
In resected pancreatic head adenocarcinoma who completed adjuvant gemcitabine-based chemo, this supports omitting fluoropyrimidine-sensitized CXRT overall and in node-positive pts; the node-negative subgroup gain is hypothesis-generating, not yet grounds to add RT.
- Does adjuvant CXRT benefit node-negative resected pancreatic cancer? n=770 · primary completion 2028-06 · phase 3 adjuvant chemoRT vs chemo, resected PDACrecruiting Radiotherapy With GX Regimen as Adjuvant Therapy for High-risk Patients Following Pancreatic Cancer Surgery Phase 3n=288 · primary completion 2029-05 · phase 3 adjuvant RT+chemo vs chemo alone
- Confirmation with modern FOLFIRINOX adjuvant backbone active Testing the Use of the Usual Chemotherapy Before and After Surgery for Removable Pancreatic Cancer Phase 3n=358 · primary completion 2028-12 · peri-op vs adjuvant FOLFIRINOX, resectable PDAC
📚 Sources · 📄 1 paper
FIRESTORM
ForHigh-risk meningioma: WHO grade 2 STR or recurrent, postop RT
TL;DR5-yr PFS 65.8% vs 38.8% favoring dose-escalated RT (BED ≥79.2 Gy), HR 0.40; OS not improved.
The trade-off is the actionable read: escalating to BED ≥79.2 Gy (≈66 Gy/33 fx) roughly doubled 5-yr PFS (65.8% vs 38.8%) but tripled any-grade radionecrosis (33.9% vs 13.2%), with severe RN unchanged (5.1% vs 3.2%) and no OS gain. Benefit was largest after subtotal resection.
9 details 3 trials watching
Individual patient-level meta-analysis pooling 7 institutions, N=248 (59 DE-RT, 189 SD-RT). Retrospective, non-randomized; compared by Kaplan-Meier, Cox multivariable, and IPTW propensity analysis.
High-risk meningioma: 75.8% WHO grade 2, 41.5% recurrent (grade 3 the remainder), 75.2% subtotal resection.
DE-RT defined as biologically effective dose ≥79.2 Gy (equivalent 66 Gy/33 fx); SD-RT comparator conventionally fractionated 59.4 Gy/33 fx or 60 Gy/30 fx. Mixed photon/carbon vs photon-alone DE-RT showed no PFS difference (81.3% vs 92.0% at 3y, P=.34).
Primary: progression-free survival, DE-RT vs SD-RT. Also overall survival and CNS radionecrosis.
OS not improved despite the PFS gain: 5-yr OS 83.8% vs 68.4% (P=.056 UVA), non-significant on MVA (HR 0.66, P=.27) and IPTW (HR 0.77, P=.42).
| Endpoint | DE-RT | SD-RT |
|---|---|---|
| 3-yr PFS | 86.4% | 55.6% |
| 5-yr PFS | 65.8% | 38.8% |
| Adjusted HR (MVA) | 0.40 (0.24-0.69), P=.001 | ref |
| IPTW HR | 0.45 (0.24-0.83), P=.01 | ref |
| Radionecrosis | DE-RT | SD-RT |
|---|---|---|
| Any grade | 33.9% (20/59) | 13.2% (25/189) |
| Grade 3+ | 5.1% | 3.2% |
Any-grade radionecrosis higher with DE-RT (33.9% vs 13.2%, P=.001) but grade 3+ similar (5.1% vs 3.2%); most RN was low-grade.
Standard-dose postoperative meningioma RT (RTOG-0539 high-risk 60 Gy, EORTC-22042 60 Gy) sits at/below this cohort's SD-RT arm; the dose-response signal here motivates the ongoing randomized escalation question.
Retrospective non-randomized pooling: DE-RT allocation confounded, IPTW mitigates but cannot fully adjust. PFS gain without OS benefit; prior-RT and grade imbalance across arms.
Retrospective non-randomized IPD pooling; DE-RT allocation confounded despite IPTW. PFS-only gain, no OS benefit. Signal supports escalation but needs randomized confirmation.
In high-risk meningioma (WHO grade 2, subtotally resected or recurrent) receiving postoperative RT, this supports a higher dose (BED ≥79.2 Gy) for local control; it does not extend to gross-totally-resected grade 1 disease or establish an OS benefit.
- Randomized confirmation of dose-escalated RT for high-risk meningioma active A Trial of Increased Dose Intensity Modulated Proton Therapy (IMPT) for High-Grade Meningiomas Phase NAn=21 · primary completion 2027-08 · increased-dose IMPT for high-grade meningioman=90 · primary completion 2028-12 · proton dose-escalation, 5y RFS in grade II/III
- Whether the PFS gain translates to an OS benefit
- Optimal escalation technique and dose (photon vs particle) recruiting Long-term Cognitive and Functional Impact of Proton-therapy or Modern Fractionated Radiotherapy in Cavernous Sinus Meningioma: An Open-label Randomized 1:1 Phase III Study Phase NAn=160 · primary completion 2032-02 · randomized proton vs photon RT, phase 3
📚 Sources · 📄 1 paper
Abstract
RTOG 0539 NCT00895622
ForWHO grade 1-3 meningioma, post-resection, newly diagnosed or recurrent
TL;DR10-yr PFS 72.2% intermediate-risk (54Gy) and 42.5% high-risk (60Gy) meningioma on adjuvant RT; low-risk observed 85.2%.
The RT read is patient selection: low-risk grade 1 (GTR/STR) observed carried only 8.9% 10-yr cumulative progression, backing omission, while intermediate-risk earns 54Gy/30fx adjuvant. High-risk 60Gy still leaves 39.3% 10-yr progression, marking the ceiling of adjuvant RT alone in grade 2/3 disease.
7 details 5 trials watching
Prospective phase 2, multi-institutional (NRG/RTOG), risk-adapted by WHO grade, extent of resection, and recurrence status. 244 consented, 165 protocol-treated. Central pathology review; data cutoff 8/15/2023.
Adults ≥18, Zubrod 0-1, histologically confirmed unifocal WHO grade 1-3 meningioma, any resection extent. Low-risk n=60, intermediate n=52, high-risk n=53.
Intermediate-risk 54 Gy and high-risk 60 Gy, both in 30 fractions, adjuvant. Low-risk received no RT (observation). No hypofractionation or SRS arm.
Primary (3-yr PFS) reported previously. This analysis reports long-term PFS, OS, and cumulative incidence of progression (competing-risk) at ~12-yr median follow-up.
Per-cohort 10-yr PFS, OS, and cumulative-incidence values are in the table above. Median PFS not reached for low- and intermediate-risk.
| Cohort (management) | 10-yr PFS | 10-yr OS | 10-yr cum. incidence progression |
|---|---|---|---|
| Low-risk, observed | 85.2% | 94.1% | 8.9% (3.2-18.2) |
| Intermediate, 54Gy | 72.2% | 84.7% | 21.2% (10.8-33.9) |
| High-risk, 60Gy | 42.5% | 51.1% | 39.3% (25.8-52.5) |
RT-attributable grade 3+ toxicity 9.6% (intermediate, 5/52) and 15.1% (high-risk, 8/53). The observed low-risk cohort carried no RT toxicity.
No randomised RT-vs-observation trial in grade 2 meningioma has reported. ROAM/EORTC-1308 and NRG-BN003 (GTR grade 2) remain open; RTOG 0539 is the prospective benchmark.
Each risk cohort is single-arm, no randomised RT-vs-observation comparison; modest per-cohort N (~50-60); grading predates molecular integration into WHO CNS grading.
Prospective multi-institutional risk-adapted phase 2, 12-yr mature f/u, sets RT patient-selection benchmark. Each cohort single-arm; no randomised RT-vs-observation comparison.
In newly diagnosed grade 1 meningioma after gross or subtotal resection, this supports observation over adjuvant RT; it does not soften the case for 54-60Gy in recurrent grade 1, grade 2, or grade 3 disease.
- Randomised confirmation of RT omission after GTR of grade 2 meningioma not yet Efficacy of Postoperative Radiotherapy for Atypical Meningioma Without Venous Sinus Invasion After Gross-total Resection Phase NAn=140 · primary completion 2028-01 · postop RT need after GTR of atypical WHO II
- Role of dose escalation or systemic therapy for high-risk (grade 3) disease active An Open-Label Phase II Study of Nivolumab or Nivolumab/Ipilimumab in Adult Participants With Progessive/ Recurrent Meningioma Phase 2n=40 · primary completion 2024-12 · nivo/ipi for progressive/recurrent WHO IIIrecruiting Combination of Everolimus and 177Lu-DOTATATE in the Treatment of Grades 2 and 3 Refractory Meningioma: a Phase IIb Clinical Trial Phase 2n=28 · primary completion 2026-03 · everolimus + Lu-DOTATATE, refractory WHO 2/3active A Trial of Increased Dose Intensity Modulated Proton Therapy (IMPT) for High-Grade Meningiomas Phase NAn=21 · primary completion 2027-08 · IMPT dose intensification for high-grade WHO II/IIIn=90 · primary completion 2028-12 · proton dose escalation 68-72 Gy, WHO II/III
- Molecular grading integration to refine risk stratification
📚 Sources · 📄 1 paper
Abstract
RAPCHEM
ForSmall (<5cm) cN1 breast, post-neoadjuvant chemo + surgery, mostly ALND
TL;DR10-yr locoregional recurrence 2.9% (24/838) with radiotherapy de-escalated by nodal response to neoadjuvant chemo; no comparator arm.
Reported via The ASCO Post →
The RT read is the intermediate arm: pts with 1-3 residual nodes got breast RT with regional nodal RT omitted, yet 10-yr LRR held at 3.2%. With low-risk mastectomy pts left with no RT (2.4%), this is the uncontrolled signal behind omitting nodal RT after partial nodal response to NAC, the question B-51 will settle.
7 details 3 trials watching
Prospective, non-randomized multicentre cohort (BOOG 2010-03), 17 Dutch centres, enrolled 2011-2015. Single arm, no with-vs-without RT comparator. 10-year follow-up.
Small (<5 cm) breast cancer with 1-3 clinically involved nodes, treated with neoadjuvant chemotherapy then surgery. Most underwent axillary lymph node dissection. N=848 (838 with follow-up).
RT allocated by post-chemo nodal status. Low (node-negative): breast RT after BCS, RT omitted after mastectomy. Intermediate (1-3 residual nodes): breast/chest wall, regional nodal RT omitted. High (≥4 nodes): breast/chest wall plus nodal RT. Dose/fractionation not reported in source.
Locoregional recurrence (breast, chest wall, or nodal, without distant disease) at 10 years. No formal primary-endpoint statistic reported in source.
Overall 10-yr LRR 2.9% (24/838). Rates stayed low across all three tailored groups, including the de-escalated arms (see table).
| Risk group | RT approach | 10-yr LRR |
|---|---|---|
| Low (node-negative after chemo) | Breast RT after BCS; RT omitted after mastectomy | 2.4% (7/291) |
| Intermediate (few residual nodes) | Breast/chest wall, regional nodes not treated | 3.2% (12/370) |
| High (many residual nodes) | Breast/chest wall + regional nodal RT | 2.8% (5/177) |
Consistent with the de-escalation direction of trials testing nodal RT after NAC, but the randomized answer is **NSABP B-51/RTOG 1304 (NCT01872975)**, testing nodal RT in pts converting to ypN0, expected ~3 years.
Single-arm and uncontrolled: cannot show tailored RT is non-inferior to standard fields. ALND-era staging limits transfer to current SLNB practice. Dose/fractionation and per-group RT compliance not reported in source.
Single-arm, uncontrolled cohort with no with-vs-without RT comparator; cannot show tailored de-escalation is safe. Randomized answer (NSABP B-51) still pending.
In cN1 breast cancer with 1-3 residual nodes after neoadjuvant chemo, this uncontrolled 10-yr data supports reduced-field RT with regional nodes left untreated; it does not extend to pts with ≥4 residual nodes, who still received nodal RT.
- RNI omission after ypN1 vs standard nodal fields, non-inferior? recruiting Internal Mammary Lymph Nodes Irradiation in High-risk Breast Cancer After Neoadjuvant Chemotherapy Phase 3n=722 · primary completion 2032-07 · IMN irradiation vs omission in ypN+ post-NAC
- Post-mastectomy RT omission after nodal conversion to ypN0 active Standard or Comprehensive Radiation Therapy in Treating Patients With Early-Stage Breast Cancer Previously Treated With Chemotherapy and Surgery Phase NAn=1636 · primary completion 2023-09 · comprehensive nodal + chest wall RT vs standard
- Does risk-tailored RT transfer to an SLNB-staged axilla? recruiting Axillary Management in Breast Cancer Patients With Needle Biopsy Proven Nodal Metastases After Neoadjuvant Chemotherapy Phase NAn=1900 · primary completion 2030-02 · omit axillary RT if SLN ypN0 after NACT
📚 Sources · 📄 1 paper
Abstract
AREST
ForAdequately resected pT1-2N0 oral SCC with ≥1 intermediate-risk feature
HR 0.52
3-yr LRFS 89.2% vs 80.9%, 95% CI 0.30-0.91, p=0.02 (ITT)
TL;DR3-yr LRFS 89.2% vs 80.9%, HR 0.52 (0.30-0.91) p=0.02 favoring adjuvant RT in resected intermediate-risk pT1-2N0 oral SCC; no OS/DFS gain.
The move is observe-vs-treat in adequately resected pT1-2N0 OSCC with one adverse feature: 60Gy/30fx to tumor bed plus at-risk neck cut 3-yr loco-regional failure (HR 0.52), strongest in oral tongue over buccal mucosa (exploratory). The gain is loco-regional only, so weigh it against RT morbidity when baseline LRR risk is low.

| Arm | 3-yr LRFS | HR (95% CI) | p |
|---|---|---|---|
| Adjuvant RT | 89.2% (84.3-93.3) | 0.52 (0.30-0.91) | 0.02 |
| Observation | 80.9% (74.6-86.1) | ref | — |
8 details 2 trials watching
Phase 3, open-label, multicenter RCT (India); 1:1 to adjuvant RT vs observation, N=392 (191 RT, 201 observation), stratified by subsite, PNI/LVE, differentiation. Median follow-up 47.2 months.
pT1-2 pN0 OSCC with ≥1 intermediate-risk feature (DOI 5-10mm, PNI, LVE, or poor differentiation), after adequate surgery: margins ≥5mm and ipsilateral level I-III neck dissection with ≥16 nodes.
60Gy in 30 fractions over 6 weeks to the resected tumor bed and at-risk neck nodal region.
Primary: 3-yr loco-regional recurrence-free survival (LRFS), KM with log-rank. Secondary: DFS, OS, and cumulative incidence of loco-regional failure (competing-risk).
Per-protocol LRFS 91.1% vs 80.9%, HR 0.43 (0.23-0.80), p=0.01. DFS and OS not significantly different between arms.
| Analysis | Adjuvant RT | Observation | HR (95% CI), p |
|---|---|---|---|
| ITT | 10.6% (6.1-15.1) | 18.9% (13.3-24.6) | 0.52 (0.30-0.91), p=0.021 |
| Per-protocol | 8.7% (4.3-13.1) | 18.9% (13.3-24.6) | 0.43 (0.23-0.79), p=0.007 |
Prior evidence for adjuvant RT in this pN0 intermediate-risk setting was retrospective (per the abstract); AREST is the first randomized confirmation.
Open-label, abstract-only; benefit is loco-regional control only, no OS/DFS at 47.2-mo median. Observation LRFS (80.9%) exceeded the 70% powering assumption, so the absolute LRFS gain is modest.
First randomized backing for the guideline-listed retrospective signal that RT cuts LRR in adverse-feature pN0 OSCC; loco-regional benefit only, no OS/DFS, open-label abstract.
In an adequately resected pT1-2N0 oral tongue SCC with a single intermediate-risk feature, this supports adjuvant RT for loco-regional control but not survival, and it does not extend to buccal mucosa (weaker signal) or node-positive disease.
- Does loco-regional control benefit translate to survival with longer follow-up? n=85 · primary completion 2026-08 · postop RT vs PD-1 maintenance, survival endpoint
- Optimal adjuvant approach for buccal mucosa vs oral tongue subsites? recruiting A Study of Radiation Therapy After Surgery in People With Oral Tongue Squamous Cell Carcinoma Phase 2n=24 · primary completion 2027-06 · postop IMRT tailored to oral tongue subsite
- Which single intermediate-risk feature drives the RT benefit?
📚 Sources · 🐦 1 tweet · 📄 1 paper
#ASCO26
— Dr Rishabh Jain (@DrRishabhOnco) May 27, 2026
🗣️ The AREST trial tackles one of the biggest gray zones in oral cavity cancer.
After adequate surgery in pT1-2N0 OSCC with intermediate-risk features:
✅ Adjuvant RT improved loco-regional control
❌ No OS benefit observed
3-year LRFS:
🔹 89.2% vs 80.9%
🔹 HR 0.52… https://t.co/qsALPFX032 pic.twitter.com/F4XzTMETih
Abstract
LBA8005: Concurrent Thoracic RT + Chemoimmunotherapy in ES-SCLC
ForTreatment-naïve ES-SCLC, stage IV or III ineligible for curative chemoRT
HR 1.14
10.0 vs 11.8 mo, 95% CI 0.84-1.56, p=0.40; OS not met
TL;DROS 10.0 vs 11.8 mo, HR 1.14 (0.84-1.56), p=0.40: concurrent thoracic RT added no benefit to durvalumab-based chemoIO in ES-SCLC.
The tested RT is concurrent (30 Gy/10 fx, day 21-28 with chemoIO), not CREST's consolidative post-chemo RT in responders, so the consolidative question stays open. Even the low-burden subgroup without brain or liver metastases was null (HR 1.10). Adding concurrent thoracic RT to chemoIO carries no OS benefit.

| Arm | Median OS | HR (95% CI) | p |
|---|---|---|---|
| ChemoIO + TRT | 10.0 mo | 1.14 (0.84-1.56) | 0.40 |
| ChemoIO | 11.8 mo | n/a | n/a |
+2 more figures

| Subgroup | ChemoIO+TRT | ChemoIO | HR (95% CI) | p |
|---|---|---|---|---|
| Completed 4 chemoIO courses | 11.9 mo | 12.1 mo | 1.02 (0.72-1.44) | 0.92 |
| No brain/liver mets | 11.9 mo | 13.2 mo | 1.10 (0.65-1.87) | 0.72 |

| Arm | Median PFS | HR (95% CI) | p |
|---|---|---|---|
| ChemoIO + TRT | 5.1 mo | 1.10 (0.84-1.45) | 0.49 |
| ChemoIO | 5.0 mo | n/a | n/a |
7 details 5 trials watching
Randomized phase III, 1:1 (chemoIO+TRT n=115, chemoIO n=113). Stratified by liver and brain metastases. Primary: overall survival; secondary ORR, PFS, toxicity.
Treatment-naïve ES-SCLC, stage IV or stage III ineligible for curative chemoRT, ECOG 0-1, ≥1 measurable thoracic lesion. Asymptomatic or stable brain metastases allowed.
Four cycles durvalumab 1500 mg + carboplatin AUC 5 + etoposide (100 mg/m² IV days 1-3, or 200 mg/m² PO days 2-4) Q3W, then durvalumab 1500 mg Q4W maintenance.
Concurrent thoracic RT 30 Gy in 10 fractions, starting day 21-28. PCI 25-30 Gy offered to responders in both arms; WBRT 20-30 Gy for brain metastases per routine.
Primary OS not met and numerically favored chemoIO alone; PFS and both prespecified subgroups (course completers, no brain/liver metastases) were also null. Effect sizes in figures.
CREST (Slotman, Lancet 2015) used the same 30 Gy/10 fx but as consolidative RT after chemotherapy in responders, before immunotherapy, and suggested a survival benefit. Adding RT concurrently to chemoIO shows none.
Open-label (RT cannot be blinded). Tests only the concurrent schedule, not the consolidative timing prior data supported. No toxicity or RT-delivery data in source to explain the numerically inferior OS.
Randomised phase III, prespecified OS primary, null; contests the CREST-era expectation that thoracic RT benefits ES-SCLC, now tested concurrently with chemoIO.
In treatment-naïve ES-SCLC beginning durvalumab plus platinum/etoposide, this questions adding concurrent thoracic RT (no OS benefit); it does not extend to consolidative thoracic RT given after chemotherapy in responders.
- Does consolidative thoracic RT after chemoimmunotherapy still benefit ES-SCLC? n=150 · primary completion 2025-03 · RT to all residual lesions after chemoIO in ES-SCLCrecruiting Phase II Trial of Consolidative Thoracic Radiotherapy for ES-SCLC After Standard Care of Chemo-immunotherapy Phase NAn=104 · primary completion 2025-09 · single-arm consolidative TRT after PD-1/L1 chemoIOrecruiting Association of Thoraco-mediastinal Radiotherapy With Maintenance Immunotherapy Treatment With Atezolizumab Phase 2n=37 · primary completion 2026-12 · thoraco-mediastinal RT + maintenance atezolizumab
- Optimal timing and sequencing of thoracic RT with chemoimmunotherapy active Low-dose Radiotherapy Combined With Durvalumab, Chemotherapy(EP) in the Treatment of ES-SCLC Phase 2n=30 · primary completion 2023-02 · low-dose RT concurrent with 1L durvalumab chemon=46 · primary completion 2027-12 · sequential TRT after 1L durvalumab chemoIO
📚 Sources · 🐦 1 tweet
🚨 #ASCO26 | #️⃣LBA8005⁰☢️ Concurrent thoracic radiotherapy + chemoimmunotherapy in ES-SCLC
— Masahiro TORASAWA, MD. PhD. (@M_Torasawa) June 2, 2026
👥 ES-SCLC⁰Durvalumab + platinum/etoposide⁰± concurrent thoracic radiotherapy⁰TRT: 30 Gy / 10 fractions, starting day 21–28
📊 Randomized phase III⁰ChemoIO + TRT: n=115⁰ChemoIO… pic.twitter.com/TDA5amz59e
COMPPARE
ForDe novo localized prostate cancer, excl very-high-risk and metastatic
TL;DRProton vs IMRT: no difference in bowel urgency (6% vs 5.7%), ≥G2 GI tox, or 3-yr biochemical control in localized prostate.
The RT read is that rectal spacer use, not proton vs photon, moved GI toxicity: 2-yr G2+ fell to ~4.4-4.7% with a spacer vs 7.2-8.7% without (p=0.009), similar across modalities. Protons showed no toxicity or 3-yr biochemical-control edge, arguing against the proton premium for localized disease.

| Endpoint | IMRT | Proton | P |
|---|---|---|---|
| Bowel urgency (EPIC) | 6% | 5.7% | 0.28 |
| Bowel frequency (EPIC) | 4% | 3.5% | 0.43 |
| GI tox ≥G2 (CTCAE) | 5.6% | 5.2% | 0.60 |
| 3-yr FFDP (PSA) | 97.9% | 98.0% | 0.90 |
+1 more figure

| Group | 2-yr G2+ GI toxicity (95% CI) |
|---|---|
| IMRT, no spacer | 7.2% (5.0%, 9.9%) |
| Proton, no spacer | 8.7% (5.0%, 14%) |
| IMRT, spacer | 4.4% (2.8%, 6.4%) |
| Proton, spacer | 4.7% (3.6%, 6.0%) |
6 details 5 trials watching
Prospective comparative effectiveness study (COMPPARE, PCORI-funded), non-randomized proton vs photon cohorts across 51 centers. 2524 accrued July 2018-October 2022. Early results, short follow-up.
De novo localized prostate cancer, excluding very-high-risk and metastatic. Proton cohort n=1500, photon (IMRT) cohort n=1000.
Proton therapy vs IMRT; rectal spacer use captured as a covariate (FDA-approved 2015). Dose/fractionation and target volume not reported in source.
Co-primary patient-reported bowel urgency and frequency (EPIC) and ≥G2 GI toxicity (CTCAE v5), each powered 90%. Exploratory: 3-yr freedom from PSA progression.
No significant proton advantage on any endpoint (all p ≥ 0.28). Observed toxicity fell far below design assumptions (hypothesized IMRT GI tox 29%, actual 5.6%).
Rectal spacer reduced 2-yr cumulative G2+ GI toxicity in both arms (p=0.009); the spacer effect exceeded any proton-vs-IMRT difference.
Directionally consistent with PARTIQoL (randomized proton vs IMRT, localized prostate), which found no bowel-QoL advantage for protons.
Non-randomized cohorts (selection bias, residual confounding); short follow-up leaves late GU/GI toxicity and long-term control unanswered; dose/fractionation not reported.
Prospective but non-randomized cohorts (selection bias); early results, short f/u leave late toxicity and long-term control open. Null aligns with randomized PARTIQoL non-superiority.
In localized prostate cancer (de novo, excluding very-high-risk and metastatic), these early data question routine proton use over IMRT for GI toxicity or 3-yr control; they do not yet speak to late toxicity or long-term outcomes.
- Late GU/GI toxicity beyond 3 years n=454 · primary completion 2025-12 · proton vs IMRT, side-effect head-to-headactive A Prospective Comparative Study of Outcomes With Proton and Photon Radiation in Prostate Cancer Phase NAn=3000 · primary completion 2026-02 · 3000-pt proton vs IMRT QOL + toxicity cohortn=400 · primary completion 2027-03 · proton vs photon, primary late GI toxicity
- Long-term biochemical and metastasis-free control with protons vs IMRT active A Prospective Comparative Study of Outcomes With Proton and Photon Radiation in Prostate Cancer Phase NAn=3000 · primary completion 2026-02 · proton vs IMRT cohorts, disease-control endpointn=303 · primary completion 2026-12 · proton vs IMRT hypofx, improve cancer control
📚 Sources · 🐦 1 tweet
#COMPPARE early results: in localized #ProstateCancer, #proton therapy vs #IMRT showed no sig difference in pt-reported bowel urgency/frequency, ≥G2 GI toxicity, or 3-year biochemical control. Longer follow-up needed for late toxicity/long term outcomes #ASCO2026 pic.twitter.com/yli4l8nEOY
— QianJanieQin (@QianJanieQin) May 31, 2026
ROADS
ForResected brain metastasis > 2 cm, post-op cavity RT candidates
NR vs 17 mo
Surg bed recurrence 1% GammaTile vs 12% SRS
TL;DRSurgical bed recurrence 1% vs 12% and 2yr OS 62% vs 36% favoring intraoperative GammaTile brachytherapy over post-op SRS for resected brain mets >2cm.
The safety tradeoff the headline buries: leptomeningeal disease ran 10% with GammaTile vs 3% with SRS, even as surgical-bed recurrence fell to 1% vs 12%. Radiation necrosis was comparable (8% vs 7%). This moves the intraoperative-brachytherapy-vs-staged-cavity-SRS decision for resected mets >2 cm, where SRS local control is weakest.

| Endpoint | GammaTile | SRS |
|---|---|---|
| Time to surg bed recurrence | NR | 17 mo |
| Surg bed recurrence-free survival | NR | 11 mo |
| 2-yr OS | 62% | 36% |
8 details 2 trials watching
Randomized trial, N=230, resected brain metastasis > 2 cm. GammaTile (Cs-131 collagen-tile brachytherapy) placed in the cavity at resection vs post-op stereotactic radiosurgery. ASCO 2026 final results. Primary: time to surgical bed recurrence and surgical-bed recurrence-free survival.
Resected brain metastasis > 2 cm, the larger-cavity setting where single-fraction post-op SRS local control is weakest. Histology / primary tumor not specified in source.
Experimental: intraoperative permanent Cs-131 seed brachytherapy (GammaTile) at resection. Control: post-op cavity SRS. Dose, fractionation, and cavity margin not reported in source.
Both primary endpoints and 2yr OS favored GammaTile. Safety: radiation necrosis comparable (8% vs 7%), leptomeningeal disease higher with brachytherapy (10% vs 3%).
Post-op cavity SRS is the current standard for resected brain mets (N107C, Mahajan). ROADS challenges it, favoring intraoperative brachytherapy on local control.
Abstract-only, not yet peer-reviewed; open-label. The 2yr OS advantage is large for a local therapy and OS was not a stated primary endpoint, raising the question of baseline arm imbalance.
Randomized, primary endpoint (surg bed control) hit favoring intraop brachy over the post-op SRS standard; but abstract-only, open-label, and the large OS gain warrants scrutiny.
In pts with a resected brain metastasis >2 cm needing cavity radiotherapy, this supports intraoperative brachytherapy as an alternative to post-op SRS for local control; it does not extend to intact (unresected) mets or cavities ≤2 cm.
- Whether the large OS gain reflects arm imbalance vs true benefit active Post-Surgical Stereotactic Radiotherapy (SRT) Versus GammaTile-ROADS (Radiation One and Done Study) Phase 3n=230 · primary completion 2029-08 · randomized phase 3 GammaTile vs SRT
- Leptomeningeal failure risk with intraoperative brachytherapy active Intracavitary Carrier-embedded Cs131 Brachytherapy for Recurrent Brain Metastases: a Randomized Phase II Study Phase 2n=103 · primary completion 2026-12 · randomized brachytherapy vs surgery-alone safety
- Applicability to resection cavities ≤ 2 cm
📚 Sources · 🐦 1 tweet
🚨🚨 ASCO 2026 Final Results Randomized trial resected brain met Brachytherapy vs Post-Op SRS🚨
— PDBrown (@PDBrownOnc) May 30, 2026
- Incredible Surg Bed Control with Brachy (↑↑OS as well)
- Surg bed recurrence 12% SRS vs 1% GammaTile pic.twitter.com/PCTsCluyUd
SPIN Score (Celiac Plexus SRS) NCT03323489
ForPancreatic cancer, intractable retroperitoneal pain, celiac SRS candidates
TL;DR89% pain response at SPIN 2 vs 32% at SPIN 0 for celiac SRS; post-hoc selection score, n=90.
Response is threshold-gated on baseline pain (>6 → 65.8%, rising to 85.7% at >8), and the strongest predictor was neurotoxic-chemo exposure (multivariate OR 5.1). The RT decision this moves is timing: refer for celiac SRS before neurotoxic agents. SRS dose/fractionation not reported in source (parent Lancet Oncol trial).
9 details
Post-hoc predictor analysis of the pivotal single-arm phase 2 celiac plexus SRS trial (NCT03323489, Lancet Oncol 2024). 90 evaluable pts; univariate/multivariate logistic regression with 500-iteration bootstrap internal validation.
Pancreatic-cancer pts with intractable retroperitoneal (celiac) cancer pain treated on the phase 2 SRS trial. Age and BMI were the prior-reported predictors; median baseline values not in source.
Celiac plexus radiosurgery, target D12-L2. Dose and fractionation not reported in source (specified in the parent Lancet Oncol trial), so transferability of the technique can't be judged here.
Pain response = ≥2-point reduction in average BPI-SF pain from baseline to 3 weeks. Score performance judged by optimism-corrected AUC.
Two independent predictors (severe baseline pain, no prior neurotoxic chemo) build a 0-2 score with a monotonic response gradient (see tables). Discrimination modest, AUC 0.714 corrected.
| SPIN score | Pain response | n |
|---|---|---|
| 0 | 32% | 31 |
| 1 | 53% | 40 |
| 2 | 89% | 19 |
| Predictor | Univariate OR | Multivariate OR |
|---|---|---|
| Neurotoxic chemo exposure | 5.33 (2.13-13.4), p<0.001 | 5.1, p=0.009 |
| Baseline pain intensity | 1.73, p=0.003 | 1.8, p=0.003 |
| Age | 1.06, p=0.014 | dropped (collinearity) |
| Therapy line | 0.65, p=0.04 | dropped (collinearity) |
Celiac plexus SRS is a novel non-invasive palliative option recently added to NCCN guidelines. This analysis converts the parent trial's flat response into an actionable selection score and argues for earlier use, before neurotoxic chemotherapy.
Post-hoc, single-arm data; predictors are associative. Internal bootstrap validation only (optimism-corrected AUC 0.714), external validation required. Subjective 3-week pain endpoint; score not prospectively tested.
Post-hoc predictor modeling of a single-arm phase 2; internal bootstrap validation only, external validation pending. Associations, not a prospectively validated selection tool.
In pancreatic-cancer pts with severe retroperitoneal pain and no prior neurotoxic chemo (SPIN 2), this supports earlier celiac plexus SRS, where 89% (n=19) achieved pain response; it does not extend to SPIN-0 pts, whose response was 32% (n=31).
- External validation of the SPIN score in an independent cohort
- Whether earlier SRS before neurotoxic chemo improves outcomes prospectively
- Durability of pain response beyond 3 weeks
📚 Sources · 🐦 1 tweet
Celiac SRS = convenient, effective tx for intractable pain, but who benefits most?
— Dr. Nina Niu Sanford (@NiuSanford) May 30, 2026
Post-hoc Ph2 analysis identified 2 response predictors (SPIN score): severe baseline pain & no prior neurotoxic chemo.
Supports earlier use before potential chemo neuropathy. #ASCO26 @OncoAlert pic.twitter.com/3qFYU6N1iD
Wait or Treat? NCT05236946
ForAsymptomatic brain mets, EGFR/ALK-mutant metastatic NSCLC, on TKI + chemo
Sub-HR 0.35
95% CI 0.21-0.59, p<0.001; favors upfront RT
TL;DRUpfront cranial RT cut 2y intracranial progression (21.7% vs 50%, sub-HR 0.35) but no OS gain; survival numerically favored delayed (HR 1.45).
The primary endpoint actually favored upfront RT (2y intracranial progression 21.7% vs 50%, sub-HR 0.35), yet OS trended toward delayed (2y 48% vs 60%) with 6% radiation necrosis vs none. Better CNS control bought no survival and added toxicity, so upfront cranial RT can be safely deferred to intracranial progression.

| Endpoint | Upfront RT | Delayed RT |
|---|---|---|
| Events | 20 | 47 |
| 1-yr intracranial PD | 8.7% (2.9-14.5) | 25.7% (16.8-34.7) |
| 2-yr intracranial PD | 21.7% (12.6-30.8) | 50% (39.2-60.9) |
| Sub-HR (95% CI) | 0.35 (0.21-0.59), p<0.001 | ref |
8 details 4 trials watching
Phase 3 open-label RCT, 1:1, N=208 (105 upfront cranial RT vs 103 delayed) at a single center (Tata Memorial). Median follow-up 30.6 mo; stratified by GPA and synchronous vs metachronous BM.
Metastatic EGFR- or ALK-mutant NSCLC with radiologically measurable, completely asymptomatic brain metastases, ECOG 0-2. Both arms received TKI + chemotherapy.
Delayed arm held cranial RT until intracranial progression or patient request, with MRI brain q3mo for year 1 then q6mo. RT dose, fractionation, and technique (SRS vs WBRT) not reported in source.
Primary: intracranial PFS. Secondary: OS, PFS, toxicity, ORR, neurocognition, PROM.
Primary endpoint met for intracranial control but did not translate to survival; the OS trend and radiation-necrosis signal both favored deferral. See the intracranial-progression figure and survival table for effect sizes.
First randomized evidence on RT timing in this population. Consistent with the CNS-active TKI era (osimertinib, alectinib, lorlatinib), where strong systemic intracranial control supports deferring RT.
Open-label and single-institution. Powered for intracranial PFS, not OS, so the survival and necrosis signals favoring deferral are secondary. RT technique not reported.
Randomized phase 3, primary intracranial-PFS endpoint met, but no OS benefit and less necrosis with deferral; backs the emerging TKI-first, defer-RT approach in oncogene-driven NSCLC.
In asymptomatic brain metastases from EGFR/ALK-mutant metastatic NSCLC on TKI plus chemo, this supports deferring cranial RT until intracranial progression; it does not extend to symptomatic brain mets or oncogene-negative NSCLC.
- Neurocognition and PRO outcomes by RT timing (not reported in source)
- Does RT technique (SRS vs WBRT) change the deferral tradeoff? n=115 · primary completion 2026-07 · randomizes SRT vs hippocampal-sparing WBRT
- Durability of TKI-first intracranial control beyond 2 years n=162 · primary completion 2024-12 · osi alone vs early SRS, asymptomatic BMactive Study of Osimertinib + SRS vs Osimertinib Alone for Brain Metastases in EGFR Positive Patients With NSCLC Phase 2n=40 · primary completion 2025-04 · osimertinib-alone arm tests TKI-first controlrecruiting Early or Delayed Intervention of Brain Radiotherapy Combined With Almonertinib in EGFR Mutated NSCLC With Brain Metastases Phase 3n=232 · primary completion 2028-12 · randomizes early vs delayed RT on EGFR-TKI
📚 Sources · 🐦 3 tweets
#ASCO26 | Wait or Treat? Brain RT in EGFR/ALK+ NSCLC
— OncLive.com (@OncLive) May 29, 2026
Presented by Dr Anil Ramakant Tibdewal.
A landmark Phase III randomized trial from @TataMemorial addressed a long-standing question: should asymptomatic brain metastases in oncogene-driven NSCLC receive upfront cranial RT or… pic.twitter.com/lRy9CfyQ8r
Should asymptomatic brain mets await systemic response in front line within EGFR/ALK context? I think yes. Despite reducing icPD, delayed brain RT OS looked better and radiation necrosis didn’t occur vs 6% #ASCO26 pic.twitter.com/O6d7GrvtU4
— Dr Riyaz Shah (@DrRiyazShah) May 29, 2026
No improvement in survival with up front radiation. OS favored delayed radiation with 2y OS 48% with early radiation vs 60% in late (OS HR 1.45). Also, radiation necrosis less common and less severe in delayed arm. Each case unique but delayed approach appealing #ASCO26 pic.twitter.com/wIhjqxhSaq
— Stephen V Liu, MD (@StephenVLiu) May 29, 2026
EORTC Cutaneous Lymphoma RT Recommendations
TL;DRLow-dose RT (8-12 Gy) recommended for indolent cutaneous lymphomas; MF 1-yr local control ≥92%, but no RCT defines a standard dose per entity.
The actionable read is the dose floor: 4 Gy (1-2 fx) underperformed vs 8-12 Gy, so 8-12 Gy stays the low-dose local standard for MF, 24 Gy reserved for large/refractory lesions or pre-autoSCT remission. Low-dose TSEBT trades durability for repeatability and lower toxicity, moving the de-escalation decision in indolent CTCL.
7 details 4 trials watching
EORTC cutaneous lymphoma tumour group expert-opinion / consensus recommendations, synthesizing retrospective case series and limited prospective registries. Proposes a treatment algorithm to standardize radiation dose across EORTC centres.
Modalities span electrons, photons, kilovoltage X-ray, brachytherapy. Low-dose regimens favored for low toxicity and repeatability on relapse; higher-dose TSEBT reserved for remission induction before autologous SCT.
No completed RCTs define the standard dose per entity; recommendations rest on retrospective series and expert consensus. Authors call a prospective trial urgently needed.
| Entity / setting | RT dose |
|---|---|
| MF plaque/tumour (local) | 8-12 Gy / 2-3 fx |
| Low-dose TSEBT (palliative) | 8-12 Gy |
| TSEBT pre-autoSCT | up to 24 Gy |
| Cutaneous DLBCL, leg type | 16-45 Gy (4 Gy/wk to ≤40 Gy) |
In indolent cutaneous lymphoma (MF plaque/tumour, pcALCL, cutaneous B-cell), this supports low-dose RT (8-12 Gy) as effective skin-directed treatment; it does not set a dose for aggressive CTCL variants, where low-dose RT has a limited role.
- Optimal radiation dose per cutaneous lymphoma entity n=52 · primary completion 2025-12 · 4 Gy low-dose RT in cutaneous B-cell lymphoman=50 · primary completion 2027-12 · phase 2 ultra-low-dose RT vs higher-dose in MF
- Durability of low-dose TSEBT vs higher-dose regimens not yet TOtal Skin Electron Beam Therapy (Low-dose) for Tumor Clone Eradication in Early-stage Mycosis Fungoides Phase 3n=78 · primary completion 2027-02 · phase 3 low-dose TSEBT, clone-eradication EP
- TSEBT combined with immunotherapy in Sézary syndrome recruiting Mogamulizumab + Low-Dose Total Skin Electron Beam Tx in Mycosis Fungoides & Sézary Syndrome Phase 2n=30 · primary completion 2026-12 · LD-TSEBT + mogamulizumab in MF/SS
📚 Sources · 📄 1 paper
DBCG IMN2 NCT06549920
ForNode-positive breast cancer, incl. 1-3 positive nodes; no neoadjuvant therapy
HR 0.85
95% CI 0.76-0.94, p=0.0016; 15yr OS 65.0% vs 60.8%
TL;DR15yr OS 65.0% vs 60.8% with IMNI, adjusted HR 0.85 (0.76-0.94); benefit persists under modern systemic therapy and 3D RT.
The 1-3 positive-node subgroup is the RT read: IMNI benefit held at the lowest nodal burden, no subgroup found for omission, moving elective IMN coverage where guidelines diverge. Reassuring on toxicity too: 15yr ischemic/valvular cardiac death 0.2% (right/IMNI) vs 0.7% (left) under 3D planning.
8 details 4 trials watching
Prospective nationwide population-based cohort, N=4541, 6 RT centres, treated 2007-14. IMNI assigned by tumour laterality: right-sided → IMNI, left-sided → no IMNI. Median follow-up 13.7 yr.
Node-positive breast cancer, including the 1-3 positive-node low-burden group. Excluded prior malignancy, bilateral cancer, neoadjuvant systemic therapy, pre-RT recurrence, non-standard RT.
Modern systemic backbone: taxane chemotherapy, trastuzumab, aromatase inhibitors, the era hypothesized to shrink absolute IMNI gain.
3D-based RT. IMNI delivered to right-sided tumours only; laterality allocation balances cardiac dose. Dose/fractionation not reported in source.
Primary: overall survival. Secondary: breast cancer mortality, distant metastasis.
IMNI improved all three endpoints (see table). Absolute 15yr OS gain 4.2% (65.0% vs 60.8%).
| Endpoint | Adjusted HR (95% CI) | p |
|---|---|---|
| Overall survival | 0.85 (0.76-0.94) | 0.0016 |
| Breast cancer mortality | 0.84 (0.74-0.95) | 0.0077 |
| Distant metastasis | 0.87 (0.78-0.98) | 0.026 |
| Study | Design | Signal |
|---|---|---|
| DBCG IMN1 (2003-07) | prospective cohort, n=3089 | +4.7% abs OS, f/u 14.8yr |
| EBCTCG meta-analysis | n=12,167 | +3% abs 15yr survival, regional node RT |
| Korean KROG 06-08 | 3D-RT, modern systemic | negative for IMNI |
Confirms DBCG IMN1 (+4.7% abs OS at 14.8 yr) and the EBCTCG meta-analysis (+3% abs 15yr survival, regional node RT); contradicts the negative Korean KROG 06-08 in the modern-therapy era.
Non-randomized: IMNI assigned by tumour laterality rather than randomization, so residual confounding is possible despite balanced baseline characteristics.
Large prospective laterality-allocated cohort, not randomized; confirms IMN1 + EBCTCG that IMNI benefit persists with modern systemic therapy. Non-random design caps it below practice-changing.
In node-positive breast cancer treated with upfront surgery then modern systemic therapy, especially 1-3 positive nodes, this supports including internal mammary nodes in the RT target; it does not extend to neoadjuvant-treated pts, who were excluded.
- Randomized confirmation of IMNI benefit in 1-3 node patients active Postmastecomy Internal Mammary Nodal Irradiation for High-risk Breast Cancer Patients Phase 3n=2400 · primary completion 2025-11 · phase 3 randomizing IMNI vs none, DFS endpoint
- IMNI value in neoadjuvant-treated patients (excluded here) recruiting Internal Mammary Lymph Nodes Irradiation in High-risk Breast Cancer After Neoadjuvant Chemotherapy Phase 3n=722 · primary completion 2032-07 · phase 3 IMNI vs none in post-NACT ypN+ pts
- IMNI cardiac safety with modern breath-hold or proton planning recruiting Robustness Evaluation of Deep Inspiration Breath-Hold (DIBH) Plans in Internal Mammary Irradiationn=25 · primary completion 2026-12 · DIBH plan OAR dose in IMN irradiationn=750 · primary completion 2027-12 · IMPT vs IMRT toxicity, heart among key OARs
📚 Sources · 📄 1 paper
PEACE V-STORM NCT03569241
ForPelvic nodal oligorecurrent prostate (≤5 nodes), post radical local Rx, PS 0-1
76% vs 63% at 4y
HR 0·62 (80% CI 0·44-0·86), p=0·063
TL;DR4-yr MFS 76% vs 63% favoring ENRT over MDT for pelvic nodal oligorecurrence, HR 0·62 (80% CI 0·44-0·86, p=0·063).
The RT read: whole-pelvis ENRT (45 Gy/25fx + SIB 65 Gy) beat node-only MDT on 4-yr MFS (76% vs 63%, HR 0·62), consistent with occult pelvic nodal disease driving the failures MDT leaves untreated. Moves the elective-nodal-coverage decision in ≤5-node pelvic recurrence.
7 details 1 trial watching
Phase 2, open-label, randomised (1:1) screening trial, 21 hospitals in 6 countries. 196 randomised (MDT 99, ENRT 97), 190 evaluable, modified ITT. Median follow-up 50 mo (IQR 42-58).
Men with PET-detected pelvic nodal oligorecurrence (≤5 nodes) after radical local prostate treatment; WHO PS 0-1, histologically confirmed adenocarcinoma. All male.
ENRT: 45 Gy/25fx whole pelvis + SIB 65 Gy to PET-positive nodes (or salvage LND). MDT: SBRT 30 Gy/3fx every other day (or salvage LND). Both + 6 mo ADT. Stratified by tracer (choline vs PSMA) and MDT type.
Primary: metastasis-free survival (any M1 on PET or death), modified ITT. Reported with 80% CIs, a phase 2 screening threshold, not the conventional 95%.
Grade 3 events low in both arms and numerically higher with ENRT (urinary incontinence, diarrhoea). No treatment-related deaths.
First randomised ENRT-vs-MDT comparison for nodal oligorecurrence. Prior oligomet RCTs (STOMP, ORIOLE) tested MDT vs observation, not elective nodal RT, so this adds the missing head-to-head.
Open-label; primary endpoint p=0·063 did not clear conventional significance and rests on a phase 2 screening design. Authors position ENRT as a potential standard awaiting phase 3.
| Endpoint | ENRT (80% CI) | MDT (80% CI) | HR (80% CI) |
|---|---|---|---|
| 4-yr MFS | 76% (69-81) | 63% (56-69) | 0·62 (0·44-0·86), p=0·063 |
| Grade 3 AE | ENRT | MDT |
|---|---|---|
| Urinary incontinence | 10% | 6% |
| Diarrhoea | 2% | 1% |
First randomised ENRT-vs-MDT comparison; ENRT's MFS edge diverges from MDT-favouring practice. Phase 2 screening design, p=0·063, awaits phase 3.
In men with PET-detected pelvic nodal-only oligorecurrence (≤5 nodes) after radical local treatment, this favors whole-pelvis ENRT over node-only MDT; it does not extend to extrapelvic M1, bone, or visceral oligometastatic recurrence.
- Phase 3 confirmation of ENRT superiority over MDT n=26 · primary completion 2029-07 · elective nodal SBRT added to MDT for nodal oligorecurrence
- Whether the MFS benefit translates to overall survival
- Long-term GU and GI toxicity of whole-pelvis ENRT with SIB
📚 Sources · 📄 1 paper
SWOG S1007
ForHR+/HER2− breast, 1-3 nodes, Oncotype RS ≤25
TL;DR5y LRR 0.55% without RNI vs 0.85% with; IDFS unchanged by RNI (HR 1.03 premenopausal, 0.85 postmenopausal) in RS ≤25 N1 breast.
The RT read: RNI omission after breast conservation carries low locoregional risk, 5y LRR 0.55% without RNI vs 0.85% with, in RS ≤25 N1 disease. Chemo omission alone is not an RNI indication, so this supports withholding RNI in biologically favorable N1, pending randomized confirmation.
6 details 3 trials watching
Secondary analysis of SWOG S1007 (RxPONDER), a phase 3 RCT of chemo omission by 21-gene recurrence score. RNI receipt was prospectively recorded, not randomized. Median follow-up 6.1y; survival landmarked at 1y.
HR+/HER2−, Oncotype RS ≤25, 1-3 positive nodes. 4871 had RT forms; 81% received RT, and 59% of those with target data received RNI (targeting ≥ supraclavicular region).
RNI defined as targeting at least the supraclavicular region. The 59/41 split in RNI use reflects genuine practice equipoise in favorable N1 disease.
LRR was low across every locoregional approach; only mastectomy without RT reached 1.7%. IDFS did not differ by RNI in either menopausal group (see tables).
| Locoregional therapy | 5y cumulative LRR |
|---|---|
| BCS + RT + RNI | 0.85% |
| BCS + RT, no RNI | 0.55% |
| Mastectomy + PMRT | 0.11% |
| Mastectomy, no RT | 1.7% |
| Menopausal status | IDFS HR | 95% CI | p |
|---|---|---|---|
| Premenopausal | 1.03 | 0.74-1.43 | 0.87 |
| Postmenopausal | 0.85 | 0.68-1.07 | 0.16 |
Consistent with MA.20 / EORTC 22922, where RNI's benefit was concentrated in higher-risk node-positive disease. TAILOR RT (MA.39) is randomizing RNI in exactly this RS-low N1 population.
RNI comparison is non-randomized: confounding by indication (higher-risk pts selected for RNI) can mask a true RNI effect. Landmarking at 1y and diverse-setting RT reporting add noise.
RNI vs no-RNI comparison is non-randomized within RxPONDER; confounding by indication limits the null IDFS and low-LRR read. Randomized RNI trial (TAILOR RT) pending.
In HR+/HER2− breast with 1-3 positive nodes and Oncotype RS ≤25, this supports omitting regional nodal irradiation given low LRR; it does not extend to higher recurrence-score or >3 node disease.
- Randomized confirmation of RNI omission in favorable-risk N1 disease recruiting Evaluating Omitting of Internal Mammary Irradiation Among Early Stage Intermediate Risk (N1) Breast Cancer Phase NAn=214 · primary completion 2025-10 · genomic model omits IMN irradiation in N1recruiting The T-REX Trial: Tailored Regional External Beam Radiotherapy in Clinically Node-negative Breast Cancer Patients With 1-2 Sentinel Node Macrometastases. Phase NAn=1350 · primary completion 2028-12 · RCT omitting regional RT, 1-2 macromets, ER+/HER2-recruiting RecurIndex Guided Avoidance of Regional Nodal Irradiation for Node Positive Breast Cancer Phase NAn=540 · primary completion 2029-08 · RecurIndex-guided RNI avoidance in N1 low-risk
- Durability of low LRR beyond 6 years without RNI
📚 Sources · 📄 1 paper
Abstract
EORTC 22922/10925
ForStage I-III breast, medial/central primary or axillary node-positive
HR 1.00
95% CI 0.90-1.10, p=.967; 20yr OS 61.0% vs 61.8% (ns)
TL;DR20yr OS 61.0% vs 61.8%, HR 1.00 (p=.967): IM-MS-RT cut breast cancer mortality (HR 0.82) but raised non-BC deaths (HR 1.26).
The RT read is competing mortality: IM-MS-RT's breast cancer mortality benefit (HR 0.82) is fully offset by excess cardiac and lung deaths (HR 1.26) at 20yr. With 1996-2004 planning the survival case nets to zero, so contemporary heart-sparing (DIBH/IMRT) is the variable that decides whether IM-MS nodal coverage still pays off.
7 details 5 trials watching
Phase 3 multicenter RCT with central RT quality assurance; 4004 women randomized 1996-2004 to added IM-MS nodal RT vs none. Prespecified for final analysis at 20yr on a delayed-benefit hypothesis; median follow-up 22.2yr.
Stage I-III breast adenocarcinoma, age ≤75. Eligible if central/medial primary (any nodal status) OR any-quadrant primary with axillary node involvement. Surgery was mastectomy or BCS plus ALND; median age 54.
Intervention added internal-mammary + medial-supraclavicular (levels 3-4) nodal irradiation on top of standard breast/chest-wall RT. 1996-2004 planning era (2D/3D, pre-DIBH/IMRT); dose and fractionation not specified in source text.
Primary: overall survival. Secondary: disease-free survival, distant metastasis-free survival, breast cancer mortality, any breast recurrence.
Primary OS was flatly null; the significant efficacy signals (lower breast cancer mortality, fewer breast recurrences) were offset in OS terms by excess non-breast-cancer deaths. Per-endpoint numbers in the table.
| Endpoint (20yr) | IM-MS-RT | Control | HR (95% CI), p |
|---|---|---|---|
| Overall survival | 61.0% | 61.8% | 1.00 (0.90-1.10), p=.967 |
| Disease-free survival | 48.2% | 49.0% | 0.97 (0.89-1.06), p=.515 |
| Distant metastasis-free | 58.9% | 59.8% | 0.97 (0.88-1.08), p=.578 |
| Breast cancer mortality | 18.6% | 22.4% | 0.82 (0.72-0.95), p=.006 |
| Non-BC/unknown deaths | 20.4% | 15.8% | 1.26, p=.002 |
| Late morbidity | IM-MS-RT | No IM-MS-RT |
|---|---|---|
| Lung fibrosis | 6.3% | 3.2% |
| Cardiac fibrosis | 2.7% | 1.7% |
| Cardiac disease | 15.2% | 11.7% |
| Severe cardiac (G3-4) | 1.9% | 1.7% |
| Severe lung (G3-4) | 0.3% | 0.0% |
Excess late lung fibrosis, cardiac fibrosis, and cardiac disease with IM-MS-RT is the mechanism behind the competing non-breast-cancer mortality; severe grade 3-4 cardiac and lung events stayed rare in both arms (table).
Aligns with the 10-yr EORTC 22922 report (Poortmans, NEJM 2015) and MA.20 in showing regional nodal RT improves disease control more than OS. The new 20yr signal: late cardiopulmonary deaths neutralize the breast cancer mortality gain.
1996-2004 planning predates modern cardiac-sparing, so the non-breast-cancer-death penalty likely overstates contemporary risk. Systemic therapy followed era standards (tamoxifen era), not current regimens. OS as primary is a high bar a single nodal-RT field rarely clears.
Large randomized phase 3, OS-primary, 22yr f/u: internally valid to contest the IM-MS-RT survival rationale, which the mortality-toxicity tradeoff nullifies. Divergence is the headline.
In a woman with a medial/central or node-positive stage I-III breast tumor, this tempers the survival rationale for adding the internal-mammary + medial-supraclavicular field specifically; it does not change breast/chest-wall or axillary RT indications.
- Does modern heart-sparing RT (DIBH/IMRT) preserve the mortality benefit without the cardiac penalty? recruiting Robustness Evaluation of Deep Inspiration Breath-Hold (DIBH) Plans in Internal Mammary Irradiationn=25 · primary completion 2026-12 · DIBH heart sparing while covering IMNn=500 · primary completion 2029-11 · IMPT vs IMRT toxicity for nodal breast RT
- Which subgroups still net an OS gain from IM-MS-RT coverage? active Postmastecomy Internal Mammary Nodal Irradiation for High-risk Breast Cancer Patients Phase 3n=2400 · primary completion 2025-11 · IMN vs no-IMN on DFS in high-risk pts
- Optimal patient selection for internal-mammary chain coverage in the contemporary era recruiting Evaluating Omitting of Internal Mammary Irradiation Among Early Stage Intermediate Risk (N1) Breast Cancer Phase NAn=214 · primary completion 2025-10 · clinical-genomic model to omit IMI in N1recruiting Radiotherapy Dose Adaptation Based on Tumor Biology in Patients With cN2b-N3 Breast Cancer Phase NAn=120 · primary completion 2028-03 · dose adaptation for IM/SCV nodal mets
📚 Sources · 📄 1 paper
Abstract
Bladder Adjuvant Radiotherapy Trial
ForHigh-risk MIBC post-cystectomy (pT3-4, N+, or margin+), chemo-treated
HR 0.43
2y LRFS 87.1% vs 76.0%; 95% CI 0.20-0.96, P=.04
TL;DR2y LRFS 87.1% vs 76.0%, HR 0.43 (0.20-0.96) P=.04 favoring adjuvant pelvic IMRT after cystectomy; DFS/BCSS/OS all NS.
Locoregional control is the RT read: 2y LRFS 87.1% vs 76.0% (HR 0.43) with stoma-sparing IG-IMRT 50.4Gy/28fx to the cystectomy bed plus pelvic nodes, no added severe toxicity. DFS, BCSS, and OS all trended toward RT but none significant at N=153, reopening adjuvant pelvic RT for high-risk MIBC without settling survival benefit.
8 details 3 trials watching
Phase 3 multicenter RCT, 1:1, N=153 (RT=77 vs Obs=76); stratified by nodal involvement and chemotherapy timing (neoadjuvant/adjuvant/none). Median follow-up 47 mo.
High-risk nonmetastatic urothelial MIBC after radical cystectomy: any of pT3-4, N1-3, margin-positive, or ≤10 nodes dissected. Enrolled 62% pT3-4, 41% pN+.
Stoma-sparing IG-IMRT, 50.4Gy in 28 fractions to the cystectomy bed and pelvic nodes.
Over 90% received perioperative chemotherapy (71% neoadjuvant, 20% adjuvant). None received immunotherapy.
Primary: 2-year locoregional recurrence-free survival. Secondary: disease-free survival, bladder-cancer-specific survival, overall survival.
Primary LRFS met (HR 0.43, P=.04); DFS, BCSS, and OS all favored RT but none reached significance (see table).
| Endpoint | RT | Obs | HR (95% CI) |
|---|---|---|---|
| 2y LRFS (1°) | 87.1% | 76.0% | 0.43 (0.20-0.96), P=.04 |
| DFS | 71.6% | 58.7% | 0.62 (0.36-1.05) |
| BCSS | 79.6% | 65.0% | 0.59 (0.33-1.10) |
| OS | 70.4% | 57.4% | 0.78 (0.49-1.26) |
No additional severe toxicity reported with adjuvant pelvic IMRT versus observation.
Reopens the adjuvant-RT-after-cystectomy question that prior Egyptian NCI trials raised for local control; first randomized test in the modern IG-IMRT era.
Small (N=153); primary endpoint is a locoregional-control surrogate, and survival endpoints were underpowered and nonsignificant. No immunotherapy-era comparator.
Randomised phase III hit prespecified primary LRFS endpoint favoring adjuvant RT (non-standard); but N=153 and DFS/BCSS/OS all NS. Field reopened, not settled.
In high-risk post-cystectomy MIBC (pT3-4, N+, or margin+) after perioperative chemo, this supports adjuvant pelvic IMRT as a locoregional-control option but not a proven survival gain; it does not extend to organ-confined, node-negative low-risk disease.
- Does the locoregional control benefit translate to overall survival in a larger trial? active Adjuvant Radiotherapy in Patients With Pathological High-risk Bladder Cancer (GETUG-AFU 30) Phase NAn=81 · primary completion 2027-12 · randomized adjuvant post-cystectomy RT, survival EP
- How does adjuvant RT integrate with adjuvant immunotherapy (nivolumab)? active Adjuvant Nivolumab Following Chemo-Radiation in Localized Muscle-Invasive Bladder Cancer Phase 2n=200 · primary completion 2025-02 · adjuvant nivolumab after chemoRT, 2y FFS EPrecruiting Adjuvant Concurrent Immunotherapy and Radiotherapy for the Treatment of Bladder Cancer Phase 1n=10 · primary completion 2027-04 · adjuvant concurrent IO + RT for bladder cancer
- Which high-risk subgroup (pN+ vs margin+) benefits most from adjuvant RT?
📚 Sources · 📄 1 paper
Abstract
Proton vs Photon PMRT Capsular Contracture
ForPostmastectomy implant-based reconstruction (TE/I or DTI) receiving PMRT
TL;DRProton PMRT trended toward higher capsular contracture vs IMRT photon (univariate HR 2.3; MVA HR 1.76 ns); proton+DTI worst, 50% 2yr CC.
The interaction is the read: DTI reconstruction, not modality, dominates CC risk (HR 3.0), and proton+DTI stacks to 50% 2yr CC vs 12% for photon+TE/I. When proton is chosen for cardiac/pulmonary sparing, reconstruction choice (favor TE/I over DTI) is the modifiable lever.
8 details 2 trials watching
Retrospective, IRB-approved, 2 centers within one institution, Jan 2017 to Dec 2023. N=175 (89 proton, 86 photon). CC estimated by Kaplan-Meier; Cox proportional hazards for HRs, logistic regression to verify. Median follow-up 42 mo (proton), 47 mo (photon).
Breast cancer pts with subpectoral 2-stage tissue expander/implant (TE/I) or direct-to-implant (DTI) reconstruction receiving PMRT. Median age 49 (24-78); 63% Hispanic. All TE/I pts had the expander irradiated. Groups imbalanced on laterality (P<.001) and reconstruction type (P<.001).
PBS proton vs IMRT photon PMRT. Dose and fractionation not reported in source. In TE/I, the tissue expander itself was the irradiated target.
Proton vs photon CC: univariate HR 2.3 (1.26-4.30, P=.007), attenuating to HR 1.76 (0.93-3.32, P=.083, ns) on multivariable. DTI vs TE/I: HR 3.0 (1.7-5.5, P<.001), the dominant driver. Per-group 2yr CC rates in the table.
| Modality + reconstruction | n | 2-yr CC rate |
|---|---|---|
| Proton + DTI | 36 | 50% |
| Photon + DTI | 15 | 35% |
| Proton + TE/I | 53 | 23% |
| Photon + TE/I | 71 | 12% |
Prior proton PMRT evidence centered on improved cardiac and pulmonary dosimetry; head-to-head capsular-contracture data proton vs photon were scarce. This is the largest proton reconstruction cohort reported to date.
Retrospective, single-institution, N=175, with groups imbalanced on reconstruction type and laterality. The proton effect lost significance after adjustment (P=.083), so residual confounding (reconstruction type driving both proton selection and CC) cannot be excluded.
The modifiable variable is reconstruction, not beam: DTI carries roughly 3x the CC hazard, and proton stacked on DTI reaches 50% 2yr CC. Where proton is chosen for heart or lung sparing, staged TE/I may blunt the CC penalty; a prospective comparison is needed to confirm.
Retrospective single-institution cohort; groups imbalanced on reconstruction type and laterality; proton effect lost significance on multivariable (HR 1.76, P=.083). Signal, not confirmation.
In a postmastectomy pt weighing DTI vs staged TE/I reconstruction who will receive proton PMRT, the CC signal is concentrated in DTI (proton+DTI 50% vs proton+TE/I 23% 2yr); it does not resolve proton vs photon overall, which was ns on multivariable.
- Prospective proton vs photon PMRT capsular contracture comparison
- Whether staged TE/I reconstruction mitigates proton capsular contracture risk n=300 · primary completion 2023-08 · 2-stage expander/implant, capsular contracture EPrecruiting Breast Reconstruction and Radiotherapyn=750 · primary completion 2027-08 · recon timing + type vs RT complication risk
- Mechanism: proton dose distribution vs selection bias driving contracture
📚 Sources · 📄 2 papers
Abstract
High-Dose Hyperfractionated SIB RT vs Standard RT for LS-SCLC NCT03214003
ForLS-SCLC, age 18-70, ECOG 0-1, ≤1 prior chemo course
TL;DRmOS 60.7 vs 39.5mo, HR 0.55 (0.37-0.72), p=0.003 favoring dose-escalated 54Gy BID SIB over standard 45Gy BID in LS-SCLC.
The escalation route is the RT read: 54Gy/30fx twice-daily via SIB beat the 45Gy BID standard (HR 0.55) where prior once-daily escalation (CONVERT, CALGB 30610) didn't, with grade 3-4 oesophagitis (13% vs 12%) and pneumonitis (5% vs 6%) flat. Moves the dose-escalation decision toward hyperfractionation, not once-daily.
7 details 3 trials watching
Open-label phase 3 RCT at 16 Chinese public hospitals, randomised 1:1 (54Gy n=108, 45Gy n=116), N=224. Median follow-up 46 mo. DSMB stopped the trial early for benefit (Apr 2021).
LS-SCLC, age 18-70, ECOG 0-1, previously untreated or ≤1 course of platinum-etoposide. Median age 64 (IQR 58-68), 54% male. Stratified by ECOG, stage, prior chemo course and choice.
Both arms VMAT twice-daily, 10 fx/week, PTV 45Gy/30fx. Experimental arm adds a simultaneous integrated boost to 54Gy/30fx to the gross tumour volume. PCI 25Gy/10fx for responders.
Primary: overall survival in the ITT population. Safety analysed as-treated.
mOS 60.7 mo (95% CI 49.2-62.0) with 54Gy vs 39.5 mo (27.5-51.4) with 45Gy, HR 0.55 (0.37-0.72), p=0.003.
Grade 3-4 oesophagitis 13% vs 12% (p=0.84) and pneumonitis 5% vs 6% (p=0.663), no excess with dose escalation. One treatment-related death (MI) in the 54Gy arm.
Prior escalation via once-daily RT (CONVERT, CALGB 30610) did not beat 45Gy BID; this instead escalates the twice-daily schedule with a SIB and shows an OS gain.
Open-label; early DSMB termination for benefit can overestimate the effect. Single-country, modest N=224, and predates adjuvant durvalumab consolidation (ADRIATIC).
Randomised phase 3, primary OS hit (HR 0.55), diverges from the 20-yr 45Gy BID standard. Open-label and DSMB-stopped-early temper it, but design is valid for the divergence.
In fit LS-SCLC pts aged 18-70 with ECOG 0-1 on concurrent chemoradiation, this supports 54Gy/30fx twice-daily thoracic RT over the 45Gy standard; it does not extend to pts over 70, ECOG 2+, or the durvalumab-consolidation era.
- Generalizability beyond age ≤70, ECOG 0-1, Asian cohort
- Optimal RT dose alongside durvalumab consolidation n=65 · primary completion 2027-01 · SIB high-dose RT then PD-L1 maintenance, LS-SCLC
- Confirmation in a multinational trial given early stopping active Two Schedules of Hyperfractionated Thoracic Radiotherapy in Limited Disease Small Cell Lung Cancer Phase NAn=177 · primary completion 2020-07 · randomised 45 vs 60Gy BID hyperfractionated TRTrecruiting Dose-Escalation Radiotherapy in Limited-Stage Small Cell Lung Cancer: A Phase III Randomized Trial Phase 3n=300 · primary completion 2028-09 · phase 3 RCT: 45 vs 60 vs SIB 45-54Gy BID
📚 Sources · 📄 1 paper
Single-fraction SABR for primary NSCLC and lung oligomets (pooled, n=1687)
ForPrimary NSCLC or pulmonary oligometastases, SABR candidates
TL;DR2-yr local control 90-93% and G3+ AEs 2-3% across 1687 pts (1200 primary NSCLC, 487 oligomets) treated with single-fraction SABR.
The transfer gate is the fraction size the source omits: outcomes are labeled single-fraction but no Gy dose is given, so you cannot map this 2y LC of 90-93% onto a specific regimen before offering one visit instead of a multi-fraction course. Toxicity (G3+ 2-3%) comes from 2 of 3 sites only. Moves the single- vs multi-fraction choice for lung SABR.
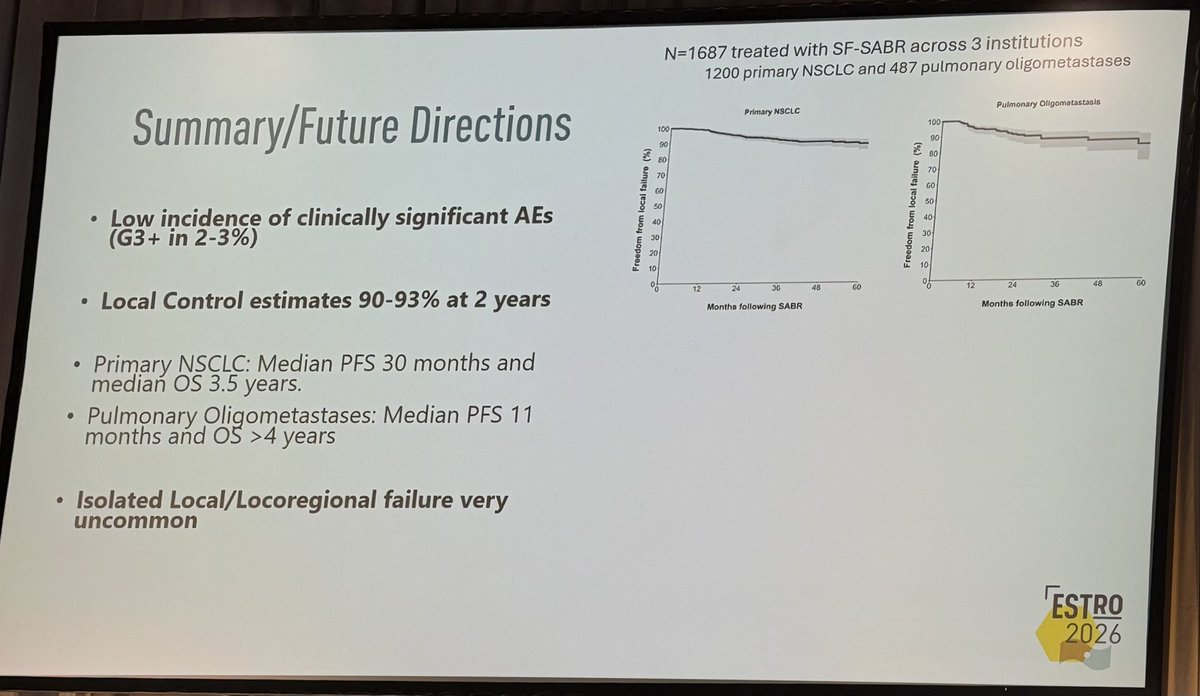
+2 more figures
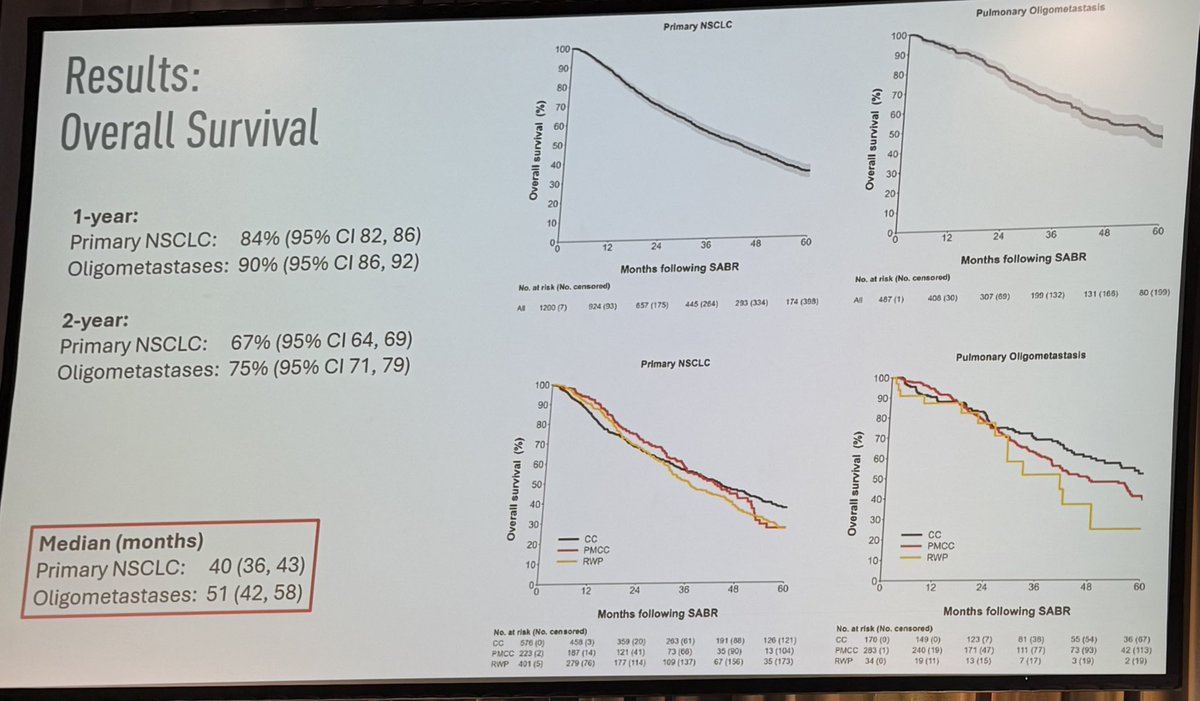
| Endpoint | Primary NSCLC | Oligomets |
|---|---|---|
| 1-yr OS | 84% (82-86) | 90% (86-92) |
| 2-yr OS | 67% (64-69) | 75% (71-79) |
| Median OS | 40 mo (36-43) | 51 mo (42-58) |
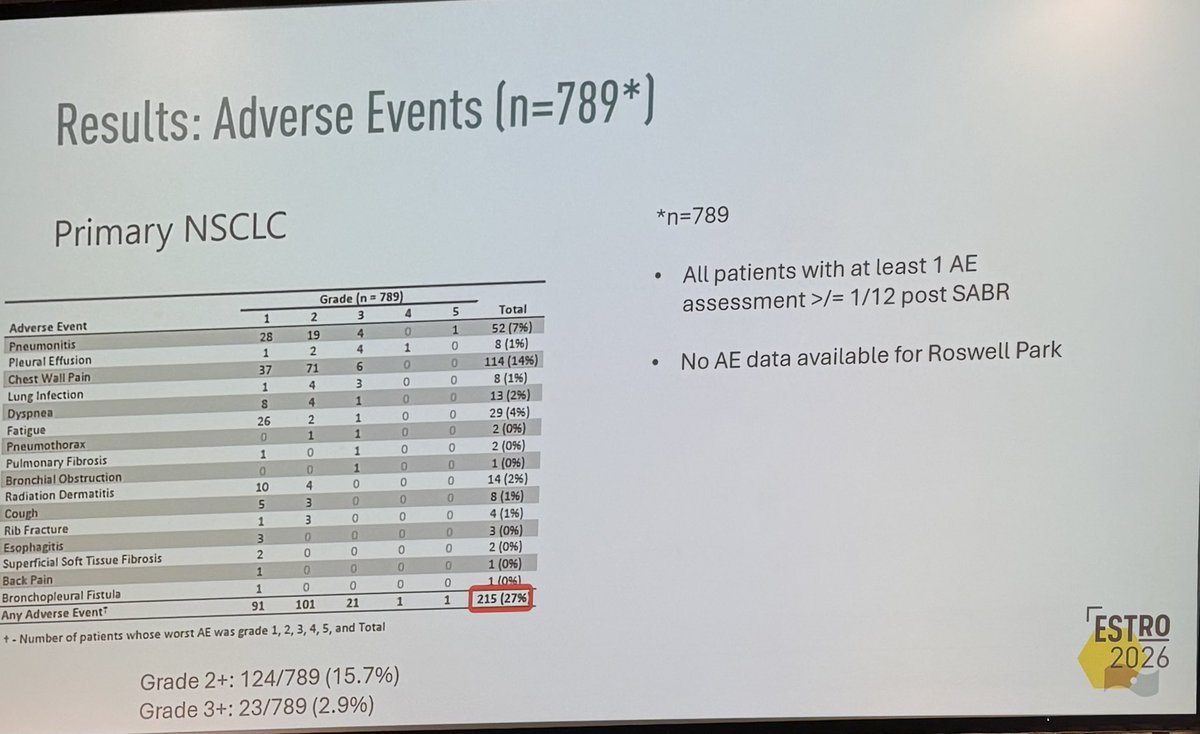
7 details 1 trial watching
Pooled retrospective analysis of 3 institutions (Peter MacCallum, Cleveland Clinic, Roswell Park). N=1687 (1200 primary NSCLC, 487 pulmonary oligometastases). No randomisation, no comparator arm; survival curves out to 60 months.
Primary NSCLC (n=1200) and pulmonary oligometastases (n=487) treated with single-fraction SABR. Stage, tumour location, and specific eligibility criteria not reported in source.
Single-fraction SABR across all pts. The Gy dose is not reported in source (single fraction only), so the specific regimen behind these outcomes is unknown, gating whether the result transfers to a given practice.
No prespecified primary endpoint stated. Reported: local control, overall survival, PFS, and adverse events.
2y local control 90-93%; isolated local/locoregional failure very uncommon. Median PFS 30 mo (NSCLC) vs 11 mo (oligomets). OS by cohort shown in the figure.
G3+ AEs 2-3% (23/789, 2.9% in the assessed NSCLC subset); G2+ 124/789 (15.7%), any AE 215/789 (27%). AE data from 2 of 3 sites only (no Roswell Park).
Consistent with SAFRON II (TROG 13.01) and RTOG 0915 supporting single-fraction lung SABR, but those were randomised; this pooled cohort carries no comparator.
Retrospective, no randomised/matched comparator. Single-fraction Gy dose unstated. AE denominator excludes one of three sites (n=789 of 1687).
Pooled retrospective single-arm cohort, no randomised or matched comparator vs multi-fraction SABR; single-fraction Gy dose unstated. Consistent with SAFRON II / RTOG 0915.
In pts with primary NSCLC or a pulmonary oligometastasis being considered for SABR, this supports single-fraction delivery as a lower-visit option with high local control; it does not establish it over a multi-fraction schedule, which this cohort did not compare against.
- Single-fraction vs multi-fraction SABR in a randomised comparison active A Pilot Study of Single Fraction Stereotactic Body Radiation Therapy (SBRT) in Central Non-Small Cell Lung Cancer Phase NAn=30 · primary completion 2028-03 · single-fx vs multi-fx SBRT in central NSCLC
- Optimal single-fraction dose across primary NSCLC and pulmonary oligometastases
📚 Sources · 🐦 1 tweet
👏🏽👏🏽👏🏽@neildwallaceie at #ESTRO26 - 1687 patients receiving single fraction SABR for #lungcancer and pulmonary oligomets, @PeterMacRadOnc / @ClevelandClinic / @RoswellPark. Fantastic local control, and low adverse rates. Should we be using “one stop” SABR more often #radonc ? pic.twitter.com/w2IlGKRU5o
— Shankar Siva (@_ShankarSiva) May 18, 2026
OPERA Trial (5-year)
ForRectal cancer, post-neoadjuvant therapy
TL;DR76% achieved a good clinical response at W14 (DRE+rectoscopy); nCR matched cCR for 5yr organ preservation (77% vs 81%), enabling early W&W selection.
nCR carries the same 5yr organ-preservation prognosis as cCR (77% vs 81%) and reflects RT-related mucosal change, not residual tumor, so an nCR at reassessment shouldn't route a patient to salvage TME. Early W14 clinical exam (DRE+rectoscopy) matched MRI TRG1-2 in 98%, letting W&W selection move up from W24.
8 details 3 trials watching
Post-hoc analysis of the randomised OPERA trial, N=141 evaluable. Tests an earlier response timepoint (W14, ~1 mo after NAT end) against the protocol W24 triad, scoring clinical tumor response (CTRE) by DRE + rectoscopy as cCR / nCR / PR.
OPERA randomised the boost after neoadjuvant chemoradiotherapy (EBRT boost vs contact X-ray brachytherapy boost); these slides don't label which arm is which. The higher early good-response rate in one arm did not translate to a 5yr organ-preservation difference (see table).
Post-hoc, non-randomised comparison of response groups; W14 selection not prospectively validated against the protocol W24 assessment. Single-trial, modest N; 5yr OP differences underpowered (p=0.24).
Authors' RT-relevant read: nCR reflects radiation change, not residual tumor, and matches cCR for organ preservation (77% vs 81%), so an nCR should not trigger salvage TME. Early DRE + rectoscopy can move W&W selection up to W14 with MRI confirmation.
| Endpoint | Arm A | Arm B | p |
|---|---|---|---|
| W14 good response (cCR+nCR) | 65% | 88% | 0.004 |
| 5yr organ preservation | 75% | 83% | 0.24 |
Post-hoc analysis of an alternate (W14 vs protocol W24) timepoint; response-group comparison non-randomised and not prospectively validated for W&W selection.
In a rectal-cancer pt with a near-complete clinical response after chemoradiotherapy, this supports continued watch-and-wait over radical TME; the 24% with only a partial response stay surgical candidates and aren't covered.
- Prospective validation of W14 vs W24 response assessment for W&W selection active Short RT Versus RCT,Followed by Chemo.and Organ Preservation for Interm and High-risk Rectal Cancer Patients Phase 3n=702 · primary completion 2023-09 · candidate match
- Optimal RT boost technique to maximise early complete clinical response active Short RT Versus RCT,Followed by Chemo.and Organ Preservation for Interm and High-risk Rectal Cancer Patients Phase 3n=702 · primary completion 2023-09 · candidate match
- Long-term regrowth risk in nCR pts managed by watch-and-wait recruiting Organ Preservation First Strategy and Intentional Watch and Wait for MRI Defined Low-risk Rectal Cancer Phase NAn=96 · primary completion 2025-09 · candidate match
📚 Sources · 🐦 1 tweet
Day FOUR of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 18, 2026
Five-year Results of the OPERA Trial: When and How to Assess Tumor Response to Guide Rectal Preservation Presented by Syrine Ben Dhia 🇫🇷 #RadOnc ☢️
This post-hoc analysis of the OPERA trial evaluated early tumor response… pic.twitter.com/KUanFTxeFh
HEAT Trial NCT01794403
ForLocalized low- to intermediate-risk prostate cancer, IPSS <12
7% vs 7.4% (AHRT vs EHRT)
Non-inferior, P=0.007 at 4.25y; NI margin 12%
TL;DRAHRT 5fx non-inferior to EHRT 26fx for biochemical failure, 7% vs 7.4% (P_NI=0.007) at 4.25y; less acute GI toxicity.
The head-to-head prior SBRT trials skipped: 5fx AHRT (36.25 Gy, SIB 40 Gy) vs 26fx EHRT, both IMRT with ADT allowed, isolating fractionation from technique and hormones. Acute G2+ GI toxicity favored the 5fx arm at equal biochemical control, moving the ultrahypofractionation choice for low- to intermediate-risk pts.
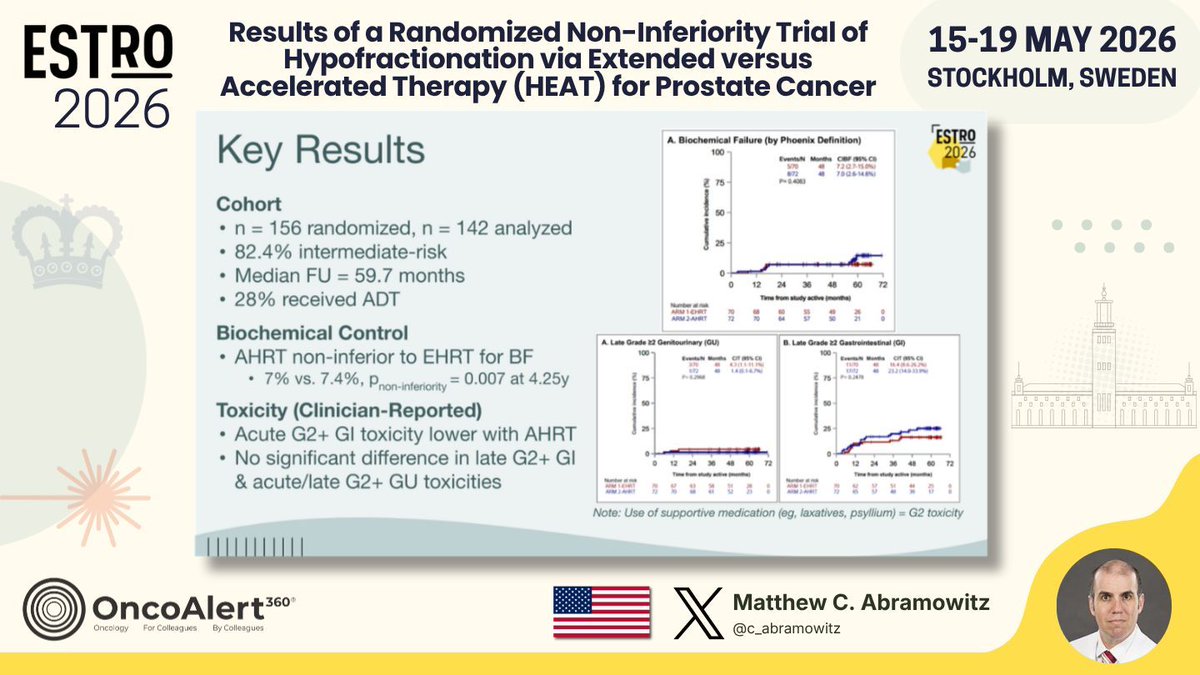
| Arm | Biochemical failure (4.25y) | P (NI) |
|---|---|---|
| AHRT | 7% | 0.007 |
| EHRT | 7.4% | ref |
+1 more figure
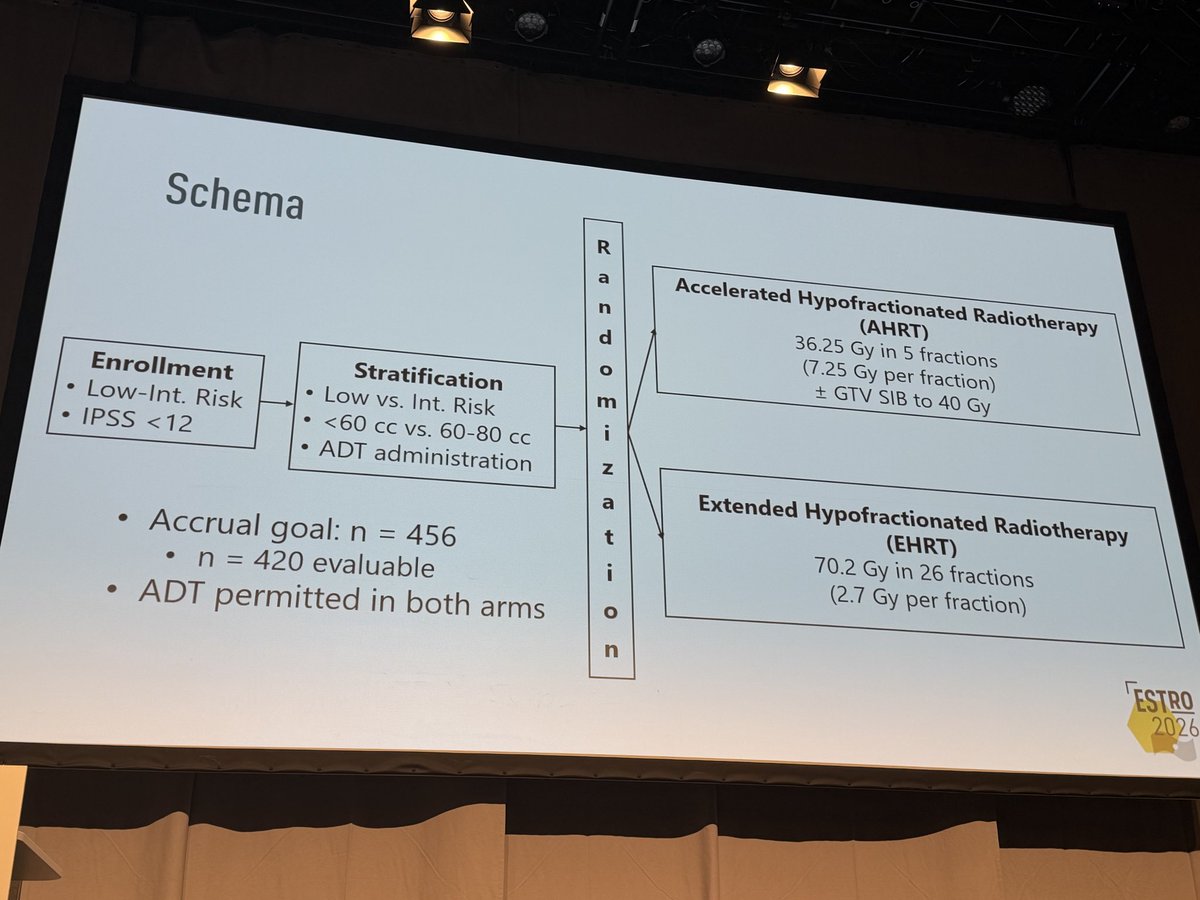
8 details 4 trials watching
Phase 3 international non-inferiority RCT, 1:1, biochemical failure (Phoenix) primary, NI margin 12%. Interim analysis at 142 analyzed of 456 planned; median follow-up 59.7 mo.
Localized low- to intermediate-risk prostate cancer, IPSS <12. 82.4% intermediate-risk; stratified by risk, gland volume (<60 vs 60-80cc), and ADT. 28% received ADT (≤6 mo, both arms).
AHRT 36.25 Gy/5 fx (7.25 Gy/fx) + GTV SIB to 40 Gy vs EHRT 70.2 Gy/26 fx (2.7 Gy/fx), IMRT in all patients.
AHRT non-inferior to EHRT for biochemical failure: 7% vs 7.4%, P non-inferiority=0.007 at 4.25y.
| Arm | Dose / fractionation | Boost / technique |
|---|---|---|
| AHRT | 36.25 Gy / 5 fx (7.25 Gy/fx) | GTV SIB to 40 Gy |
| EHRT | 70.2 Gy / 26 fx (2.7 Gy/fx) | IMRT all pts |
Acute G2+ GI toxicity lower with AHRT. No significant difference in late G2+ GI or acute/late G2+ GU toxicity. Supportive-med use (laxatives, psyllium) counted as G2.
First RCT comparing AHRT vs EHRT 1:1 with modern IMRT and ADT. Prior ultrahypofractionation trials (HYPO-RT-PC, PACE-B, NRG-GU005) used heterogeneous or no-ADT controls.
Interim analysis at roughly one-third of planned accrual; full pre-specified primary pending. Small analyzed N (142); biochemical, not clinical, endpoint.
Interim analysis at 142 of 456 planned pts; non-inferiority met but full pre-specified primary analysis pending. Underpowered vs accrual goal.
In localized low- to intermediate-risk prostate with IPSS <12, this supports 5fx AHRT as non-inferior to 26fx EHRT with less acute GI toxicity; it does not extend to high-risk disease or glands >80cc, which the trial excluded.
- Durability of biochemical control at full accrual and longer follow-up recruiting Androgen Suppression Combined With Nodal Irradiation and Dose Escalated Prostate Treatment Phase 3n=710 · primary completion 2032-10 · phase 3 SBRT vs EBRT + brachytherapy boostrecruiting PRO-BOOST-LC: Whole-Gland Boost Strategies Versus SBRT Monotherapy in PSMA-Staged Localized and Locally Advanced Prostate Cancer Phase 2/3n=1200 · primary completion 2033-12 · SBRT monotherapy vs whole-gland boost
- Does 5fx AHRT benefit extend to high-risk or larger-gland prostate? recruiting Testing Shorter Duration Radiation Therapy Versus the Usual Radiation Therapy in Patients With High Risk Prostate Cancer Phase 3n=1209 · primary completion 2036-03 · phase 3 5fx SBRT vs usual RT, high-risk
- Long-term late GU/GI toxicity with 5fx AHRT n=42 · primary completion 2028-01 · 5fx SABR, urethra/rectum-sparing, GU/GI AE
📚 Sources · 🐦 2 tweets
Day FOUR of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 18, 2026
Results of a Randomized Non-Inferiority Trial of Hypofractionation via Extended versus Accelerated Therapy (HEAT) for Prostate Cancer Presented by Matthew C. Abramowitz🇺🇸 #RadOnc ☢️ #ProstateCancer
HEAT is an international phase… pic.twitter.com/IkSTgQHwXK
The HEAT trial is another randomized demonstration of the safety & efficacy of SBRT compared to hypofractionted RT in #prostatecancer at #ESTRO26 pic.twitter.com/c9sNb3KOqo
— Pierre Blanchard, MD (@PBlanchardMD) May 18, 2026
PEACE 2
ForcN0 very-high-risk localized prostate (Gleason≥8, T3-4, or PSA≥20)
HR 0.81, ns
95% CI 0.63-1.03, p=0.088; primary endpoint not met
TL;DRPelvic nodal RT missed 1° endpoint: 7yr cPFS 67.1% vs 62.9% prostate-only, HR 0.81 (0.63-1.03) p=0.088; no MFS/PCSS/OS gain.
The RT decision is elective nodal coverage: a randomized head-to-head (n=380 vs 381) shows whole-pelvic RT adds no cPFS, MFS, PCSS or OS benefit over prostate-only in cN0 very-high-risk disease, with modern-technique toxicity minimal. Staging was conventional imaging/choline PET, not PSMA, so PSMA-defined N0 pts remain untested.
Also covered May 17

| Arm | 7yr cPFS (95% CI) | HR (95% CI) | p |
|---|---|---|---|
| Prostate-only RT | 62.9% [57.4-68.1] | ref | |
| Pelvic RT | 67.1% [61.6-72.2] | 0.81 [0.63-1.03] | 0.088 |
+1 more figure
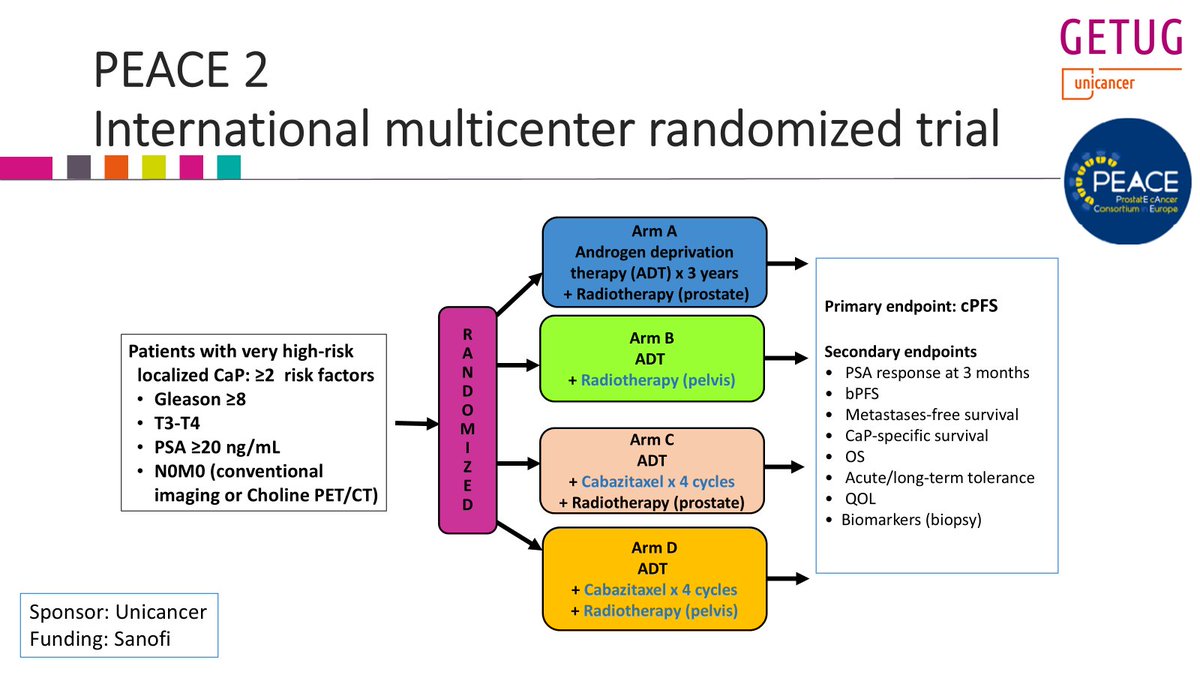
8 details 2 trials watching
Phase 3 randomized 2×2 factorial (pelvic vs prostate-only RT × cabazitaxel ×4 vs none), ADT ×3 yr in all arms. Pelvic-RT comparison n=380 vs 381, 7-year outcomes reported. Multicenter GETUG/Unicancer.
Very high-risk localized prostate: ≥2 of Gleason ≥8, T3-T4, PSA ≥20 ng/mL. N0M0 by conventional imaging or choline PET/CT, not PSMA.
High-dose RT to prostate vs whole pelvis. Dose, fractionation and nodal target volume not reported in source.
Primary: clinical PFS. Secondary: PSA response at 3 mo, bPFS, MFS, PCSS, OS, tolerance, QoL, biopsy biomarkers.
cPFS 7yr 67.1% pelvic vs 62.9% prostate-only, HR 0.81 (0.63-1.03), p=0.088, primary endpoint not met. No benefit on MFS, PCSS or OS per authors.
Authors report side effects minimal with modern RT technique; per-arm toxicity rates not reported in source.
POP-RT (2021) found whole-pelvic RT improved biochemical control in PSMA-staged high-risk N0. PEACE 2's conventionally-staged cohort shows no benefit.
Conference presentation, not peer-reviewed. Non-PSMA staging risks occult nodal misclassification. cPFS is a surrogate; RT dose/technique unspecified in source.
Randomized phase 3, prespecified cPFS not met (p=0.088); null across all clinical endpoints diverges from POP-RT's whole-pelvic benefit, so the WPRT question is contested.
In cN0 very-high-risk localized prostate staged by conventional imaging or choline PET, this questions routine elective whole-pelvic RT; it does not address PSMA-staged N0 or radiologic node-positive disease.
- Whether PSMA-staged N0 pts benefit from elective pelvic RT
- Cabazitaxel's effect and interaction with pelvic RT active A Phase III of Cabazitaxel and Pelvic Radiotherapy in Localized Prostate Cancer and High-risk Features of Relapse Phase 3n=761 · primary completion 2025-12 · phase 3 cabazitaxel + pelvic RT, high-risk localized
- A nodal-risk subgroup that still benefits from pelvic RT recruiting Abi/Pred + ADT vs ADT in PSMA-Positive, Conventionally Node-Negative Prostate Cancer Phase 2n=140 · primary completion 2033-04 · PSMA-avid occult nodes; RT + abiraterone ADT
📚 Sources · 🐦 1 tweet
Yesterday, I presented the @GETUG_Unicancer PEACE 2 trial at #ESTRO26 on the role of pelvic RT in very high risk #prostatecancer pts (staged with conventional imaging).
— Pierre Blanchard, MD (@PBlanchardMD) May 18, 2026
Twittorial below
Key conclusion: pelvic RT did not improve clinical outcomes (cPFS, MFS, PCSS, OS)...
1/n pic.twitter.com/ZKRt2QZzt1
TORPEdO
ForOropharyngeal SCC requiring bilateral-neck concurrent chemoradiotherapy
No between-arm difference
No effect size reported in source; assessed at 3/12/24mo post-RT
TL;DRUW-QoL physical composite similar IMPT vs IMRT at 3/12/24mo in OPSCC; no proton QoL-toxicity benefit (no effect size reported in source).
The proton premise, less QoL toxicity, didn't show: UW-QoL physical composite tracked identically IMPT vs IMRT from 6 weeks through 24 months, both arms at 70/56 Gy in 33fx. That undercuts routing OPSCC pts to protons for QoL benefit, though identical planning constraints and novel UK proton centres may have capped IMPT's achievable dosimetric edge.

+1 more figure

9 details 2 trials watching
Phase 3 multicentre RCT (CRUK/18/010), N=205 oropharyngeal SCC, 2:1 IMPT:IMRT, stratified by T-stage, N-stage, p16 status, and smoking history.
Oropharyngeal SCC requiring concurrent chemoradiotherapy with bilateral neck treatment. p16 status was a stratification factor, so both HPV-associated and HPV-independent disease are included.
70 Gy / 56 Gy in 33 fractions over 6.5 weeks, identical for both arms; IMPT vs IMRT is the only difference. Identical planning constraints applied across modalities.
Concurrent cisplatin 100 mg/m² on D1 and D22.
Co-primary PRO: UW-QoL physical composite at 12mo (saliva, taste, chewing, swallowing, appearance, speech). Co-primary clinician: CTCAE grade 3 weight loss (≥20% from baseline) or gastrostomy dependence at 12mo.
No between-arm difference in UW-QoL physical composite at 3/12/24mo, similar from 6 weeks post-CRT, with similar trajectories across multiple PRO questionnaires. No effect size reported in source.
Support for protons in OPSCC has rested on dosimetric and single-institution toxicity data; this randomised HR-QoL readout does not confirm a patient-reported advantage for IMPT.
Only the HR-QoL co-primary is presented; the clinician co-primary (weight loss/gastrostomy) and 5yr late-effects follow-up are unreported. No effect sizes or CIs given. Novel UK proton centres and identical constraints may cap IMPT's achievable edge.
Randomised co-primary QoL null (IMPT≈IMRT), consistent with IMRT-based CRT remaining standard. Only HR-QoL co-primary shown; clinician co-primary and 5yr late effects still maturing.
In oropharyngeal SCC planned for definitive cisplatin chemoradiotherapy, these HR-QoL data give no patient-reported reason to prefer IMPT over IMRT; they don't address the clinician co-primary (weight loss/gastrostomy) or unilateral-neck cases that could still differ.
- Does IMPT reduce 5-year late effects vs IMRT? recruiting Comparing an Investigational Scan (F-18 NaF PET/CT) to Standard of Care Imaging (F-18 FDG PET/CT) for Evaluating Vascular Complications in Patients Receiving Radiation Therapy for Head and Neck Cancer Phase Early 1n=20 · primary completion 2026-08 · candidate match
- Clinician co-primary (weight loss/gastrostomy at 12mo) result?
- Does IMPT advantage emerge only at high-experience proton centres? n=7 · primary completion 2024-11 · candidate match
📚 Sources · 🐦 2 tweets
Day FOUR of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 18, 2026
Health-related quality of life in the phase III trial of Toxicity Reduction using Proton Beam Therapy for Oropharyngeal Cancer (TORPEdO;CRUK/18/010) Presented by Matthew Tyler🇬🇧 #RadOnc ☢️
TORPEdO, a multicentre phase 3… pic.twitter.com/ZP6yK7RThL
TORPEdO. Misma planificación + constraints idénticas y centros UK noveles probablemente limitaron el potencial de #IMPT.
— Amadeo Wals (@AmadeoWals) May 18, 2026
Centros con alta experiencia se siguen viendo ventajas clínicas . La QA rigurosa del UK es una fortaleza, pero no maximiza la diferencia.#ESTRO26 #HNCSM https://t.co/rASp3QDIk1
Proton versus photon therapy for oropharyngeal cancer
TL;DRLancet correspondence on proton vs photon for oropharynx; no effect sizes reported in source (title/citation only).
- Re-ingest the full text (PDF or PMC) to get the trials named and any numbers
5 details 3 trials watching
- 🔍 Source is a PubMed citation record only: title, authors, journal, page (Lancet 2026;407:1917). No abstract or body text captured
- 🔍 Single-page Lancet item at p.1917 is the correspondence/comment page range, not a primary trial report
- 📊 No effect size reported in source: no HR, no median, no p-value, no N
- ⚠️ Cannot determine which trial(s) this comments on, or the direction of the argument, from the citation alone
- ⚠️ Do not read a proton-vs-photon verdict into this card; the underlying data are not in the source
- Proton vs photon toxicity and disease control in oropharynx n=100 · primary completion 2028-01 · 1:1 randomised photons vs protons, T1-2 tonsilactive Intensity Modulated Proton or X-Ray Therapy After Surgery for Treatment of Head and Neck Cancer, the HEADLIGHT Study Phase 2n=174 · primary completion 2028-02 · postop IMPT vs IMRT phase 2, QoL assessmentn=440 · primary completion 2031-12 · randomised phase 3 IMPT vs IMRT, stage III-IVB
📚 Sources · 📄 1 paper
INRT-AIR & DARTBOARD pooled analysis
ForOropharynx/larynx/hypopharynx HNSCC, stage I-IVB, excl T1-2N0 larynx
TL;DR5-yr solitary elective nodal recurrence 0% with ENI omission across 117 pts; 5-yr OS 87%, PFS 74%.
The failure pattern is what matters: solitary elective nodal recurrence was 0% at 5 yrs while 3-yr local recurrence ran 9.5% and distant 11%, so the residual risk sits in the primary and systemically, not in the uncovered elective levels. Node selection was AI-assisted off PET/CT plus neck CT, which gates whether the volume reproduces outside these trials.

| Endpoint | Timepoint | Value |
|---|---|---|
| Solitary elective nodal recurrence | 5-year | 0% |
| Local recurrence | 3-year | 9.5% |
| Regional recurrence | 3-year | 4.3% |
| Distant metastasis | 3-year | 11% |
| Overall survival | 5-year | 87% |
| Progression-free survival | 5-year | 74% |
| Composite MDADI (mean) | 12 months | 84.9 |
+1 more figure

10 details 5 trials watching
Patient-level pooled analysis of two prospective trials of involved nodal RT, INRT-AIR and DARTBOARD. N=117, median follow-up 3.4 years. No randomised ENI comparator arm.
HNSCC of oropharynx, larynx, and hypopharynx, stage I-IVB, excluding T1-2N0 larynx. Completed PET/CT and neck CT required for entry.
INRT omits elective nodal irradiation, treating involved nodes only, with an artificial-intelligence model assisting identification of suspicious lymph nodes. Dose, fractionation, and margin not reported in source.
5-yr solitary elective nodal recurrence 0%. 3-yr cumulative incidence: local 9.5%, regional 4.3%, distant 11%. 5-yr OS 87%, PFS 74%.
Mean composite MDADI 84.9 at 12 months, with no significant decline after treatment. No late G3+ toxicity, xerostomia, or feeding-tube rates reported in source.
Pooled single-arm data with no ENI control, so the 0% solitary elective recurrence carries no randomised contrast. Median follow-up 3.4 yrs underpins 5-yr estimates, and the AI nodal-selection step is not externally reproduced.
The dosimetric case for INRT rests on OAR sparing, but the only patient-reported outcome here is swallowing (MDADI 84.9), with no xerostomia or dysphagia comparison against ENI. Authors state randomized evidence is required before non-trial implementation.
Pooled single-arm prospective cohorts, N=117, no randomised ENI comparator; presenters explicitly require randomised evidence before non-trial use.
In PET/CT-staged oropharynx, larynx, or hypopharynx HNSCC (excluding T1-2N0 larynx) being planned for definitive chemoRT, this supports enrolling on an INRT trial rather than omitting elective nodal coverage off-protocol, and it does not speak to node-positive necks staged without PET/CT.
- Does INRT reduce late toxicity vs ENI in a randomized comparison? recruiting Dose De-escalation and Sentinel LN Mapping Driven Radiotherapy of Contralateral Neck in Ipsilateral Node Positive HNSCC Phase NAn=147 · primary completion 2027-01 · tests contralateral elective volume + dose reductionrecruiting Personalized Elective Neck Irradiation Guided by Sentinel Lymph Node Biopsy in Larynx and Pharynx Cancer. The PRIMO Study. Phase 3n=242 · primary completion 2029-12 · phase 3 SLNB-guided vs standard ENI, 242 pts
- Is the AI nodal-selection step reproducible outside these two trials? not yet SPECT-CT Guided ELEctive Contralateral Neck Treatment in Lateralized Oropharyngeal Cancer Phase NAn=128 · primary completion 2030-04 · SPECT-CT lymphatic mapping to select elective volume
- Does INRT hold for HPV-negative and oral cavity primaries? recruiting Personalized Neck Radiation Therapy Directed by Sentinel Lymph Node Biopsy for the Treatment of Oral Cavity Squamous Cell Carcinoma, PRECEDENT Trial Phase 2n=50 · primary completion 2030-07 · SLNB-directed neck RT in oral cavity SCC, cT1-4arecruiting Comparing Sentinel Lymph Node (SLN) Biopsy With Standard Neck Dissection for Patients With Early-Stage Oral Cavity Cancer Phase 2/3n=686 · primary completion 2031-04 · SLNB vs elective neck dissection, early oral cavity
📚 Sources · 🐦 1 tweet
Day FOUR of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 18, 2026
Omission of elective nodal irradiation in HNSCC: long-term results and patient-level pooled analysis from 2 prospective trials (INRT-AIR & DARTBOARD)
Presenter Sympascho Young 🇺🇸
A patient-level pooled analysis of 117 patients… pic.twitter.com/KaaT70nSNH
Multinational HCC EBRT IPD Cohort
ForVery early / early-stage HCC (BCLC-0 to A), Child-Pugh A predominant
TL;DRMedian OS 6.8y BCLC-0 and 4.6y BCLC-A across 4,913 EBRT-treated HCC pts, comparable to resection/ablation.
The treatment-naive BCLC-0 arm is the RT-relevant cell: median OS not reached (95% CI 8.6 to NR), i.e. first-line EBRT in a truly untreated very-early cohort, not salvage after failed ablation. Ablative dose independently predicted lower mortality, so this moves the dose-selection and BCLC-algorithm-placement decisions.
9 details 3 trials watching
Systematic review (search date December 15, 2022) of EBRT series meeting prespecified HCC technical standards and reporting OS, followed by individual patient data solicitation from corresponding authors. Kaplan-Meier OS and RMST stratified by BCLC stage and treatment status; random-effects Cox for covariates.
N=4,913 EBRT-treated HCC pts across a multinational author network, median follow-up 5.0 years. Stratified as treatment-naive vs treatment-experienced; BCLC stage, tumor burden, performance status, and Child-Pugh class all captured at patient level.
EBRT delivered per each contributing series; the pooling filter was prespecified technical standards for HCC. Ablative dose was independently associated with reduced risk of death, but specific dose/fractionation schedules and the ablative-dose threshold are not reported in the source abstract.
Median OS 6.8 years for BCLC-0 and 4.6 years for BCLC-A; among treatment-naive pts not reached for BCLC-0 and 5.4 years for BCLC-A. On multivariable modeling, advanced BCLC stage, higher tumor burden, worse performance status, and Child-Pugh B/C raised mortality risk; ablative dose and more recent treatment year lowered it.
| Cohort | BCLC-0 | BCLC-A |
|---|---|---|
| All pts | 6.8 yrs (95% CI 5.7-8.7) | 4.6 yrs (95% CI 4.1-5.1) |
| Treatment-naive | NR (95% CI 8.6-NR) | 5.4 yrs (95% CI 4.5-6.7) |
The authors position these OS figures as comparable with resection, thermal ablation, and other ablative locoregional therapies. That comparison is across literatures, not within a trial, so the usual selection differences (lesion location, vascular proximity, comorbidity burden) between an EBRT-referred and a resection-eligible population remain unadjusted.
No comparator arm: the resection/ablation equivalence claim is a cross-study inference. IPD came only from authors who responded, and the technical-standard filter selects for expert centers, both biasing toward better outcomes. Year-of-treatment effect confounds technique era with staging and systemic-therapy improvements.
The practical argument here is algorithmic placement: BCLC has historically routed early HCC to resection, ablation, or transplant with EBRT absent, and this is the largest patient-level dataset assembled to contest that omission. The treatment-naive BCLC-0 result matters most, since it isolates first-line EBRT from salvage-after-ablation-failure use.
Large multinational prospective-collected IPD across many sites with stage-stratified analyses, but non-randomised and no head-to-head comparator; supports EBRT's guideline-listed role rather than establishing it.
In BCLC-0 or A HCC where ablation or resection is unattractive on lesion location or comorbidity, this supports offering ablative-dose EBRT as a first-line locoregional option rather than a salvage one; it does not speak to BCLC-B/C or Child-Pugh B-C pts, where OS was worse.
- Randomised EBRT vs thermal ablation in early HCC recruiting Stereotactic Radiosurgery Versus Radiofrequency Ablation for Primary Liver Cancer Phase 2n=130 · primary completion 2025-01 · randomised SBRT vs RFA, inoperable primary liver caactive Stereotactic Body Radiotherapy Versus Radiofrequency Ablation for Unresectable, Small (≤ 3 cm) HCC Phase NAn=178 · primary completion 2026-12 · randomised SBRT vs RFA in unresectable ≤3 cm HCCn=218 · primary completion 2032-04 · SABR vs percutaneous ablation, BCLC 0/A, 2y FFLP
- Ablative dose threshold defining the OS benefit
- Generalizability beyond expert EBRT centers
📚 Sources · 📄 1 paper
Abstract
EXTEND Trial
ForOligometastatic solid tumors, 1-5 mets, on standard systemic therapy
HR 0.54
95% CI 0.41-0.72, p<0.001 (per-protocol, all baskets)
TL;DRMDT+SOC improved PFS across all baskets, HR 0.54 (0.41-0.72), p<0.001; RT delivered 98% of MDT.
The RT-relevant read is that this is essentially an SBRT trial (98% of MDT was radiotherapy) layered on top of continued systemic therapy, so the PFS gain is attributable to local ablation, not a systemic switch. The prostate-excluded HR 0.60 (0.40-0.89) is what matters for referrals outside prostate. Dose and fractionation are not in the source abstract, which gates transfer to practice.
Also covered May 17
9 details 5 trials watching
Multicenter randomized phase II basket trial, accrual 2018 to 2023. Six baskets (breast, pancreas, kidney, two prostate, "Other") each with basket-specific stratification and powering. Median follow-up 53 months.
Patients with 1-5 metastases from solid tumors, randomized to MDT+SOC vs SOC systemic therapy alone. Screened 521, randomized 350, 334 analyzed per protocol (MDT+SOC n=166; SOC n=168).
Radiotherapy was the MDT for 98% of metastases (370/379), so this reads as an ablative RT trial in all but name. Dose, fractionation, and technique are not reported in the source abstract.
Primary: PFS, pre-specified in the per-protocol set within each basket, across all baskets, and across all baskets excluding prostate. Exploratory: ctDNA and immune profiling.
Overall PFS HR 0.54 (0.41-0.72), p<0.001; excluding prostate baskets HR 0.60 (0.40-0.89). Basket-level superiority in pancreas, prostate, and "Other"; breast and kidney inconclusive. Per-basket effect sizes not reported in source.
Detectable ctDNA at enrollment tracked with shorter PFS and survival; 3-month ctDNA clearance tracked with improved survival, raising the option of a ctDNA-refined oligometastatic definition. Systemic immune activation after MDT was most pronounced in the baskets that showed PFS superiority, offered as a candidate mechanism.
Per-protocol, not ITT, primary analysis with 16 of 350 randomized patients excluded. Phase II with six baskets tested, so histology-specific claims are hypothesis-generating; no OS result reported in source.
Randomized phase II, primary PFS endpoint hit with 53mo f/u, but per-protocol analysis and basket design; histology signals explicitly framed as hypothesis-generating for phase III.
In pts with 1-5 metastases from pancreas or prostate primaries already on standard systemic therapy, this supports adding ablative MDT rather than systemic therapy alone; the breast and kidney baskets were inconclusive and do not carry the same read.
- Does MDT-driven PFS gain translate to overall survival recruiting Veterans Affairs Seamless Phase II/III Randomized Trial of STAndard Systemic theRapy With or Without PET-directed Local Therapy for Oligometastatic pRosTate Cancer Phase 2/3n=464 · primary completion 2026-09 · phase 2/3 SST +/- PET-directed local therapy, CRPC-FSn=873 · primary completion 2027-04 · phase 3 MDT +/- ADT/ARTA, n=873, PMFS endpointn=1200 · primary completion 2030-12 · n=1200 prospective LAT cohort, any-histology OMD
- Can ctDNA refine which oligometastatic pts benefit from MDT n=60 · primary completion 2027-12 · SABR cohort with ctDNA dynamics as biomarkerrecruiting Phase II Non-Randomized Study Evaluating POSLUMA-PSMA PET Response After Oligo- Metastatic/Progressive-directed Treatment With Radiotherapy (PROMPT-R) Phase 2n=50 · primary completion 2028-05 · ctDNA change after ablative RT vs PSMA-PET response
- Why were breast and kidney baskets inconclusive
📚 Sources · 📄 1 paper
Abstract
FASTRACK II NCT02613819
ForPrimary RCC ≤10 cm, medically inoperable or declined surgery, N0-N1
100% at 36, 60, and 84 mo
RECIST, intention-to-treat population; median f/u 62 mo
TL;DR100% freedom from local progression at 36, 60, and 84 months after single-fraction 26 Gy or 42 Gy/3fx SABR in inoperable primary RCC.
The size-adapted prescription is what transfers: 26 Gy × 1 for ≤4 cm, 42 Gy/3fx at 48 h intervals above that, in a cohort that was 65% T1b or higher (median 46 mm), not a small-tumour-enriched series. Two colonic obstructions place bowel as the constraint for central lesions.
10 details
Non-randomised phase 2, eight hospitals in Australia and the Netherlands (TROG 15.03, with ANZUP). Accrual July 28 2016 to Feb 27 2020: 71 enrolled, one withdrew consent before treatment, 70 treated. This report is the pre-planned final long-term follow-up, median 62 months (IQR 60-72).
Histologically confirmed primary RCC in pts who were medically inoperable, high risk, or declined surgery; ECOG ≤2; tumour ≤10 cm; N0-N1. Median age 77 (70-82), 70% male. Median tumour size 46 mm (37-55): T1a 34%, T1b 56%, T2a 9%, T3a 1%, with one N1 pt.
Size-adapted prescription: 26 Gy in a single fraction for tumours ≤4 cm, and 42 Gy in 3 fractions delivered 48 h apart for tumours >4 cm. No systemic therapy component.
Primary: freedom from local progression by RECIST, assessed in the intention-to-treat population, with safety co-assessed in ITT.
100% local control at 36, 60, and 84 months, with no local recurrences and no cancer-related deaths reported over median 62-month follow-up.
Seven pts (10%) had at least one treatment-related grade 3 event within 9 months: pain (abdominal/flank/tumour) 4 (6%), nausea and vomiting 3 (4%), colonic obstruction 2 (3%), diarrhoea 1 (1%). No grade 4 events, no treatment-related deaths, and no new long-term safety signals.
Single-arm and non-randomised: no head-to-head against partial nephrectomy, cryoablation, or radiofrequency ablation, which is the live comparison in the surgery-declining subset. N=70 with one N1 pt leaves nodal disease essentially untested. Industry co-funding (Varian) alongside Cancer Australia.
The value here is durability rather than magnitude: a flat 100% at 84 months in a cohort with median 46 mm tumours argues the ablative dose is adequate for lesions well beyond the small-renal-mass range where thermal ablation is usually deployed. The bowel events, not renal function, define the practical constraint for central tumours on the 3-fraction schedule.
Single-arm phase 2; no randomised comparator vs nephrectomy or thermal ablation. Long f/u and 100% local control do not lift a non-randomised design.
For a medically inoperable or surgery-declining pt with a T1b-T2a primary RCC ≤10 cm, this supports SABR as a definitive local option with durable 84-month local control; it does not address the surgically fit pt in whom partial nephrectomy remains untested against SABR.
- SABR vs partial nephrectomy in surgically fit pts
- SABR vs thermal ablation for T1b tumours
- Long-term renal function after single-fraction 26 Gy
📚 Sources · 📄 1 paper
Abstract
NRG/RTOG 1005 NCT01349322
ForHigh-risk early breast cancer post-lumpectomy, receiving WBI plus cavity boost
HR 1.31
90% CI 0.84-2.04, P=.037; NI margin 2.12
TL;DR7-yr IBR 2.6% vs 2.2%, HR 1.31 (90% CI 0.84-2.04): concurrent boost noninferior to sequential, cutting WBI+boost to 15 fractions.
The transferable parameter is the boost itself: 8 Gy in 15F at 0.53 Gy per day, a lower cavity total than 12 Gy/6F sequential, with 7-yr IBR 2.6% vs 2.2%. Blinded photo cosmesis at 3y numerically favored concurrent (72.0% vs 64.2%, p=0.11). This moves boost technique, not whether to boost.
9 details 4 trials watching
Randomized, unblinded, phase 3 noninferiority trial across 278 sites in North America and 6 other countries. 2,354 randomized May 2011 to June 2014, 2,255 eligible for analysis. Median follow-up 7.3 years.
Higher risk of IBR after lumpectomy and axillary surgery. Median age 55 (IQR 47-64), 35.6% under 50; 96.8% invasive, 52.7% grade 3, 29.6% ER-negative, 16.3% node-positive, 16.7% LVI, 16.7% close (<2 mm) or focally positive margins. 61.8% received chemotherapy.
Concurrent arm: WBI 40 Gy/15F with concurrent boost 8 Gy/15F at 0.53 Gy per day. Sequential arm: WBI 50 Gy/25F (52.4%) or 42.7 Gy/16F (47.6%), then 12 Gy/6F (84.9%) or 14 Gy/7F. 3DCRT in 59%, photons in 73.8%; QART scored 92.8% of contours and 91.9% of dose plans per protocol or acceptable variation.
Primary: IBR as first recurrence, noninferiority defined as an HR upper 90% CI limit below 2.12. Secondary: DFS, OS, adverse events, and cosmesis (BCTOS, physician Global Cosmesis Score, blinded central digital photo review).
56 IBR events, 24 sequential and 32 concurrent. Noninferiority held on cause-specific hazards, Fine-Gray (HR 1.31, 90% CI 0.84-2.03), and against each sequential WBI fractionation separately; the triggered superiority test was not significant. 7-yr regional nodal recurrence 1.2% (95% CI 0.8-1.7) with no difference by arm, and no differences in DFS, DDFS, or OS.
| Endpoint | Sequential (n=1,118) | Concurrent (n=1,137) |
|---|---|---|
| 5-yr IBR | 2.1% | 1.9% |
| 7-yr IBR | 2.2% (90% CI 1.5-3.0) | 2.6% (90% CI 1.9-3.5) |
| IBR HR (90% CI) | reference | 1.31 (0.84-2.04), P=.037 |
Toxicity above grade 2 was uncommon, with no significant difference in grade 3-4 events (p=0.81); radiation dermatitis, fatigue, and breast pain were most prevalent. 3-yr excellent/good cosmesis by physician rating 85.9% vs 82.4% (p=0.34) and by central photo review 64.2% vs 72.0% (p=0.11).
IMPORT HIGH tested a simultaneous integrated boost in 15 fractions against a sequential boost in the same setting; its effect sizes are not in this source. This is the larger North American test of the same question, enriched for grade 3 and node-positive disease.
Unblinded. The noninferiority margin (HR 2.12) was set under a protocol redesign against an assumed 1.59% 5-yr IBR, and the point estimate favored sequential (HR 1.31) on 56 total events. Cosmesis response rates fell to 50.5% (physician) and 47.1% (central photo) by 3 years.
Randomized phase 3, prespecified noninferiority met at 7.3-yr median follow-up; wide NI margin (HR 2.12) and a point estimate favoring sequential keep it below practice-changing.
In high-risk early breast cancer after lumpectomy (grade 3, ER-negative, node-positive, or close margins) this supports a 15-fraction concurrent boost in place of a sequential boost; it does not address boost omission, partial breast irradiation, or post-mastectomy RT.
- Durability of the concurrent boost beyond 7 years recruiting 5 fr Ultrahypofractionated WBI and SIB for Breast Cancer With Unfavorable Characteristics Phase NAn=458 · primary completion 2029-06 · randomised 5fr WBI+SIB vs 15fr WBI+SIB noninferiority
- Whether a concurrent boost transfers to regional nodal irradiation active Hypofractionated Loco-regional Adjuvant Radiation Therapy of Breast Cancer Combined With a Simultaneous Integrated Boost Phase NAn=2963 · primary completion 2021-07 · loco-regional hypofx with SIB, late morbidity 1° EPrecruiting Ultra-Hypofractionated vs Moderate Hypofractionated Radiotherapy for Regional Lymph Nodes in High Risk Breast Cancer Phase NAn=1950 · primary completion 2034-03 · randomised ultrahypofx vs moderate hypofx RNI, n=1950
- Boost omission versus concurrent boost in high-risk pts n=400 · primary completion 2025-11 · WBI +/- tumor bed boost in HER2+, 7y IBTR endpoint
📚 Sources · 📄 1 paper
Abstract
POP-RT vs PEACE-2
TL;DRWPRT bFFS HR 0.50 in POP-RT vs bPFS HR 0.97 in PEACE-2; pelvic nodal RT benefit vanishes with 3yr ADT and higher prostate dose.
POP-RTPEACE-2
The two trials differ on multiple axes at once, so the null in PEACE-2 cannot be attributed to WPRT alone: 36 vs 24 months ADT and 78 vs 74-76 Gy EQD2 to prostate. That confounding is the whole elective-nodal decision.

| Endpoint | POP-RT HR (95% CI), p | PEACE-2 HR (95% CI), p |
|---|---|---|
| bFFS / bPFS | 0.50 (0.42-0.61), p<0.001 | 0.97 (0.81-1.16), p=0.73 |
| cFFS / cPFS | 0.74 (0.61-0.90), p=0.002 | 0.81 (0.63-1.03), p=0.09 |
| MFS | 0.72 (0.58-0.89), p=0.002 | 0.93 (0.74-1.17), p=0.54 |
9 details 3 trials watching
Two independent phase III open-label randomized trials compared side by side in a curator-made graphic, not a head-to-head. Both randomized whole-pelvis RT plus prostate boost vs prostate-only IMRT in N0M0 disease.
POP-RT enrolled high / very high-risk localized prostate cancer; PEACE-2 restricted to very high-risk only. PEACE-2 staged N0M0 by conventional imaging or choline PET/CT (pre-PSMA-PET era), so PSMA-detectable occult N1 disease would have sat in both arms.
POP-RT: IMRT whole pelvis plus prostate boost, prostate dose 74-76 Gy EQD2. PEACE-2: dose-escalated IMRT whole pelvis plus boost, prostate dose 78 Gy EQD2. Same target-volume question, different dose intensity.
ADT duration is the other separating variable: 24 months (GnRH analog plus antiandrogen) in POP-RT vs 36 months in PEACE-2.
Primary: bFFS in POP-RT, biochemical PFS in PEACE-2. Secondary in both: clinical progression-free survival, MFS, OS, toxicity; PEACE-2 adds CSS.
See the efficacy table. POP-RT positive across bFFS, cFFS, and MFS; PEACE-2 no significant improvement in bPFS, MFS, CSS, or OS, with only a borderline cPFS trend.
| Endpoint | POP-RT | PEACE-2 |
|---|---|---|
| bFFS / bPFS | HR 0.50 (0.42-0.61), p<0.001 | HR 0.97 (0.81-1.16), p=0.73 |
| cFFS / cPFS | HR 0.74 (0.61-0.90), p=0.002 | HR 0.81 (0.63-1.03), p=0.09 |
| MFS | HR 0.72 (0.58-0.89), p=0.002 | HR 0.93 (0.74-1.17), p=0.54 |
Both trials reported comparable grade ≥2 late GU toxicity between arms. No significant increase in toxicity with whole-pelvis RT in either trial.
Cross-trial comparison with two major confounders (ADT duration, prostate dose), so the WPRT effect cannot be isolated. PEACE-2 is an interim analysis at median ~5.5 years vs 6.3-7.2 years in POP-RT, and biochemical endpoints mature earlier than MFS.
The graphic's own read is that longer ADT and intensified local therapy may reduce the incremental benefit of elective pelvic RT in very high-risk disease. Plausible, but with only two trials and confounding by ADT duration and dose the WPRT effect cannot be isolated.
In very-high-risk N0M0 pts committed to 3 years of ADT, this comparison questions routine elective pelvic coverage; it does not speak to pts planned for shorter ADT, where POP-RT's bFFS benefit still stands.
- Does WPRT benefit persist with PSMA-staged N0 disease? n=250 · primary completion 2031-05 · randomises PORT vs whole-pelvis RT in PSMA-N0M0recruiting PRO-BOOST-LC: Whole-Gland Boost Strategies Versus SBRT Monotherapy in PSMA-Staged Localized and Locally Advanced Prostate Cancer Phase 2/3n=1200 · primary completion 2033-12 · 1200 pts, cN0 on baseline PSMA PET, RT strategies
- Is 36mo ADT substituting for elective nodal coverage? n=60 · primary completion 2032-07 · 6mo vs 24mo ADT with EBRT in high-risk localized
- Will mature PEACE-2 follow-up change the MFS read?
📚 Sources · 🐦 1 tweet
POP RT Vs PEACE II
— Rohit Malde (@roxboxfix) May 18, 2026
2 years ADT + WPRT
Vs 3 years ADT + Prostate Only RT
Tough to choose or you already have a choice ?? pic.twitter.com/42kdSKQYKW
PRIME NCT03561961
ForHigh-risk, very high-risk and/or node-positive non-metastatic prostate, 2y ADT
Not yet mature
Interim: no signal of inferiority for SBRT arm; 4-5y data awaited
TL;DRInterim data: 36.25 Gy/5 fx SBRT with whole-pelvis RT and 2y ADT shows no inferiority signal vs 68 Gy/25 fx; BFFS immature.
The transferable point is the pelvic dose: 25 Gy / 5 fx elective nodal with SIB permitted to involved nodes, grade 3+ under 1%, which is the constraint question that has kept 5-fraction prescribing confined to node-negative prostate-only. HYPO-RT-PC never tested nodes or ADT, so this extends the ultrahypofractionation toxicity envelope, not its efficacy.

| Toxicity (Grade ≥2) | SBRT (5 fx) | Moderate Hypo (25 fx) | p |
|---|---|---|---|
| Acute GU | ~5.4% | ~4.0% | 0.59 |
| Acute GI | ~2.2% | ~3.7% | 0.20 |
| Late GU | ~10-12% | ~9-11% | NS |
| Late GI | ~5-7% | ~4-6% | NS |
| Grade 3+ GU/GI | <1% | <1% | n/a |
+1 more figure

| HYPO-RT-PC | PRIME | |
|---|---|---|
| Experimental arm | 42.7 Gy / 7 fx | 36.25 Gy / 5 fx |
| Control arm | 78 Gy / 39 fx | ~68 Gy / 25 fx |
| Accrual | 2010 - 2015 | 2018 - 2023 |
| Primary endpoint result | 10y FFS 72% vs 65%, HR 0.84 (0.69-1.03) | Not yet mature |
10 details 5 trials watching
Phase III, open-label, randomized non-inferiority trial, Tata Memorial Centre and collaborating Indian centers. Accrual 2018-2023, completed at N~434, randomized 1:1 stratified by risk group and nodal status. Median follow-up is interim, 1-2 years.
High-risk, very high-risk and/or node-positive non-metastatic prostate cancer; ECOG 0-2; life expectancy 10 years. PSMA PET/CT staging permitted, which matters for how the node-positive stratum was defined relative to older conventionally-staged trials.
Arm A 36.25 Gy in 5 fractions (7.25 Gy/fx), every other day; Arm B ~68 Gy in 25 fractions (2.7 Gy/fx) over ~5 weeks. Both arms received prostate plus whole-pelvis elective nodal RT at 25 Gy / 5 fx (or equivalent), with SIB to positive nodes allowed in the SBRT arm. Delivered in the modern IMRT/VMAT with daily IGRT era.
Long-course ADT, ~2 years, in both arms. ADT is not a randomized variable here, so the trial isolates fractionation, not the systemic question.
Primary: biochemical failure-free survival (Phoenix, nadir + 2 ng/mL). Secondary: acute and late toxicity (RTOG/CTCAE v4.0/5.0), OS, MFS, clinical failure-free survival, QoL (QLQ-C30, QLQ-PR25, IPSS), cost-effectiveness.
Interim only. Source reports no signal of inferiority for the SBRT arm on BFFS and no difference in MFS or OS in early follow-up; no HR, CI, or non-inferiority margin is reported in source. OS data explicitly immature.
No significant difference in grade ≥2 toxicity between arms: acute GU ~5.4% vs ~4.0% (p=0.59), acute GI ~2.2% vs ~3.7% (p=0.20); late grade ≥2 GU ~10-12% vs ~9-11% and GI ~5-7% vs ~4-6%, both NS. Grade 3+ under 1% in both arms, acute and late. Urinary and bowel QoL domains stable and comparable.
HYPO-RT-PC established ultrahypofractionation non-inferiority (10y FFS 72% vs 65%, adjusted HR 0.84, 95% CI 0.69-1.03) but in node-negative disease, prostate plus proximal seminal vesicles only, no pelvic RT, no ADT, mostly 3D-CRT. PRIME is testing a different question: 5 fractions with elective nodal coverage on top of 2y ADT.
Interim analysis at 1-2 years against a BFFS primary read under 2 years of ADT, where testosterone suppression flattens both curves and early concordance is close to uninformative. Toxicity is reported as approximate ranges rather than point estimates with CIs. Open-label, though toxicity grading and PSA endpoints are only modestly susceptible to that.
Interim analysis at 1-2y of a BFFS primary that needs 4-5y maturity; safety-only read. Interim data cannot promote past early-signal regardless of clean design.
In high-risk or node-positive non-metastatic prostate going to whole-pelvis RT with long-course ADT, this supports 5-fraction SBRT as tolerable but not yet as an efficacy-equivalent substitute; it says nothing about omitting ADT or treating without pelvic coverage.
- Mature 4-5y BFFS and non-inferiority margin recruiting Androgen Suppression Combined With Nodal Irradiation and Dose Escalated Prostate Treatment Phase 3n=710 · primary completion 2032-10 · ph3 nodal RT + prostate SBRT vs EBRT/brachy boost
- Late GU toxicity beyond 2y with nodal SIB active Hypofractionated Whole-Pelvis Radiotherapy (WPRT) vs Conventionally-Fractionated WPRT in Prostate Cancer Phase 2n=58 · primary completion 2024-03 · 5fx vs 25fx whole-pelvis RT, QoL primaryrecruiting Phase III Adaptive Adaptive Stereostactic Body Radiotherapy (SBRT) With Dose Escalation for High-Risk Prostate Cancer Phase NAn=390 · primary completion 2033-04 · adaptive SBRT with WPRT plus DIL boost, 5y outcomes
- Whether pelvic nodal RT itself adds benefit in this population n=224 · primary completion 2017-08 · whole-pelvis vs prostate-only RT, high risk, 5y EPrecruiting A Trial of 5 Fraction Prostate SBRT Versus 5 Fraction Prostate and Pelvic Nodal SBRT Phase 3n=1128 · primary completion 2028-06 · randomises 5fx prostate vs prostate+pelvic nodal SBRT
📚 Sources · 🐦 1 tweet
PRIME trial
— Rohit Malde (@roxboxfix) May 18, 2026
Can we safely deliver ultra-short SBRT including pelvic nodal irradiation in biologically aggressive disease treated with ADT?
With Pelvic RT
Moderate hypofractionation:
~68 Gy/25#/5w
Vs
Extreme hypofractionation/SBRT:
36.25 Gy / 5 # /1-2w
Compare HYPO RT PC pic.twitter.com/7NABknLsD5
PIVOTALboost
ForHigh-risk localised prostate, 20-fraction IMRT candidates
TL;DRLate 2yr G2+ bowel 8.2% / 8.7% / 6.5% and bladder 19.5% / 24.1% / 16.5% across prostate, +boost, +pelvic nodes arms.
The late bladder G2+ signal sits with the boost, not the nodes: 24.1% in P+B vs 19.5% prostate-only and 16.5% in PPN+B, so adding elective nodal volume did not track with worse 2yr bladder or bowel toxicity. That makes the 20-fraction focal boost plus pelvic node volume a tolerable technique choice while the biochemical/clinical failure endpoint matures.

| Arm (n) | Bowel G2+ (95% CI) | Bladder G2+ (95% CI) |
|---|---|---|
| Prostate (n=281) | 8.2% (5.7-11.7) | 19.5% (15.5-24.4) |
| Prostate+Boost (n=345) | 8.7% (6.3-12.1) | 24.1% (20.2-28.7) |
| Prostate+Nodes+Boost (n=347) | 6.5% (4.5-9.5) | 16.5% (13.1-20.6) |
+2 more figures
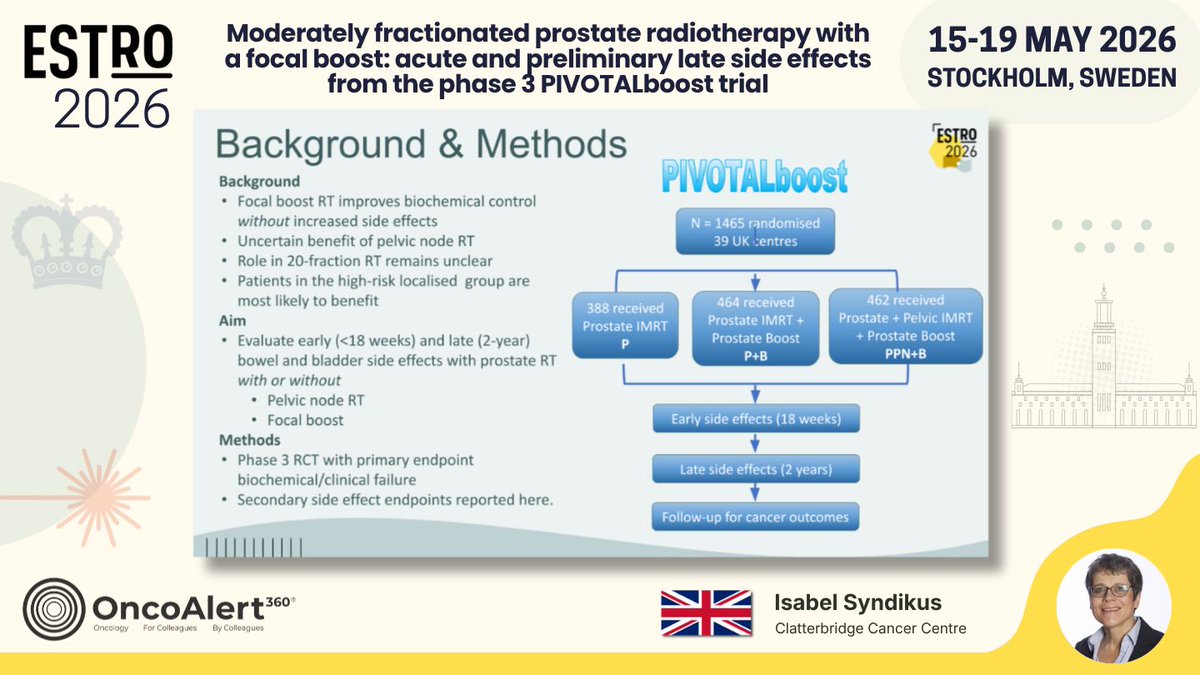
| Arm | Received |
|---|---|
| Prostate IMRT | 388 |
| Prostate IMRT + Boost (P+B) | 464 |
| Prostate + Pelvic IMRT + Boost (PPN+B) | 462 |

8 details 5 trials watching
Phase 3 RCT, N=1465 randomised across 39 UK centres. Primary endpoint: biochemical/clinical failure; the side-effect endpoints presented here are secondary.
Localised prostate cancer; the trial rationale states high-risk localised pts are most likely to benefit from pelvic node RT. Full eligibility criteria not reported in source.
20-fraction moderately hypofractionated IMRT. Arms as received: prostate alone (388), prostate + focal prostate boost (464), prostate + pelvic nodes + boost (462). Boost dose and nodal dose not reported in source.
Reported here: early bowel and bladder side effects (<18 weeks) and late (2-year, 6-24 month) G2+ events. Cancer-outcome follow-up is ongoing.
Nodal RT increased early bowel side effects, which resolved by 18 weeks post-RT. At 2 years G2+ bowel and bladder rates were similar across arms, with the numerically highest late bladder rate in the boost-without-nodes arm.
Late analysis covers only the 973 (74%) with ≥2yr follow-up, and no between-arm p-values are reported in source. The efficacy primary endpoint is unreported, so the toxicity read cannot yet be set against a benefit.
Randomised phase 3, prespecified secondary toxicity endpoint, 2yr follow-up. Efficacy 1° EP not yet reported, so it supports safety only, not a practice change.
In high-risk localised prostate pts being planned for 20-fraction IMRT, this supports the safety of adding a focal intraprostatic boost and elective pelvic nodal coverage; it does not yet speak to whether either improves biochemical or clinical control.
- Does focal boost or pelvic nodal RT improve biochemical/clinical failure recruiting A Trial of 5 Fraction Prostate SBRT Versus 5 Fraction Prostate and Pelvic Nodal SBRT Phase 3n=1128 · primary completion 2028-06 · phase 3 prostate-only vs prostate + pelvic nodal SBRTn=250 · primary completion 2031-05 · PSMA-N0M0 high risk, PORT vs whole pelvis RTrecruiting Addition of Focal Boost to Primary Radiotherapy for Prostate Cancer in 12 or 20 Fractions Phase NAn=1016 · primary completion 2040-10 · tests if intraprostatic boost improves cure rates
- Do late toxicity differences emerge beyond 2 years n=700 · primary completion 2021-12 · longitudinal GI/GU toxicity after whole-pelvis IMRTn=68 · primary completion 2025-10 · 5y accumulated GI/GU toxicity, integrated index boost
- Boost and nodal dose/fractionation details for reproducibility
📚 Sources · 🐦 1 tweet
Day THREE of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 17, 2026
Moderately fractionated prostate radiotherapy with a focal boost: acute and preliminary late side effects from the phase 3 PIVOTALboost trial Presented by Isabel Syndikus 🇬🇧 #RadOnc ☢️
In the PIVOTALboost trial, we treated 1314… pic.twitter.com/cGuR1j2Qos
PACE-NODES
ForHigh-risk localised prostate (T3a-T4, Gleason 8-10, or PSA>20), planned 12-36mo…
28% vs 21%
PPN-SBRT vs P-SBRT; no difference at 12wk, symptoms resolved quickly
TL;DRGrade ≥2 GI toxicity 28% vs 21% with added pelvic nodal SBRT over 12wk; GU unchanged, symptoms resolved by 12wk.
The deliverability number is the buried read: 11% of PPN-SBRT pts never received the allocated treatment vs 4% prostate-only, mostly unmet constraints. Nodal dose was 25Gy/5f alongside 36.25Gy/5f prostate on alternate days. That gates whether 5f elective nodal coverage is exportable outside high-volume centres, before any efficacy signal arrives.

| Endpoint | PPN-SBRT | P-SBRT |
|---|---|---|
| CTCAE grade ≥2 GI to 12wk | 28% | 21% |
| Did not receive allocation | 11% | 4% |
+2 more figures
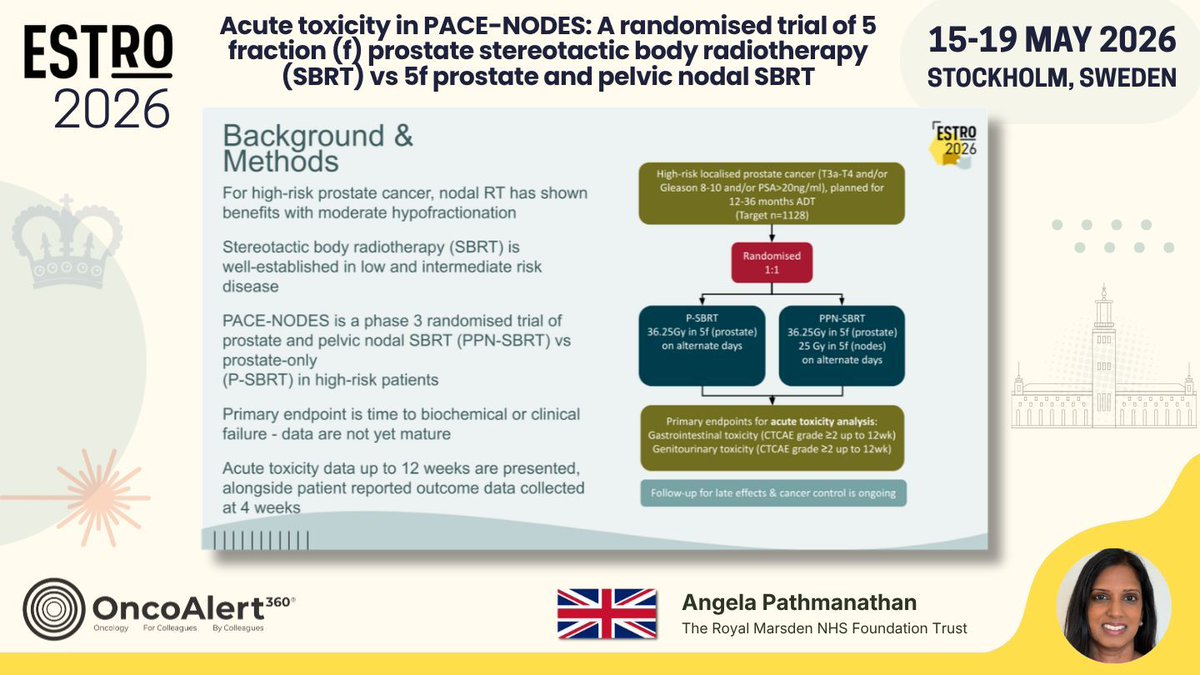

7 details 5 trials watching
Phase 3 randomised, 1:1, multicentre. 1166 pts randomised against a target of 1128. This report is the prespecified acute toxicity analysis; the trial's primary endpoint, time to biochemical or clinical failure, is not yet mature.
High-risk localised prostate cancer: T3a-T4 and/or Gleason 8-10 and/or PSA >20 ng/ml. All planned for 12-36 months ADT.
Both arms 36.25Gy in 5f to prostate on alternate days. PPN-SBRT adds 25Gy in 5f to pelvic nodes. 11% of PPN-SBRT vs 4% of P-SBRT did not receive allocation, mostly because dose constraints were not met.
Co-primary for this analysis: CTCAE grade ≥2 GI and GU toxicity to 12 weeks. Patient-reported EPIC-26 domain scores collected at 4 weeks.
Grade ≥2 GI symptoms were more frequent with PPN-SBRT (28% vs 21%) across the 12-week window, with no difference at 12 weeks. No difference in acute GU toxicity by clinician or patient report. EPIC-26 bowel domain at 4 weeks mirrored the clinician-scored GI gap.
Acute window only, capped at 12 weeks; late GI/GU effects and cancer control are still accruing. Toxicity scoring is unblinded, which matters most for clinician-graded GI events. Effect sizes for the GI difference (CI, p) were not reported in source.
Randomised, but this is an acute-toxicity readout only; the primary biochemical/clinical failure endpoint is explicitly immature. Safety supports feasibility, not adoption.
In high-risk localised prostate on long-course ADT, this supports 5f nodal SBRT as tolerable in the acute window; it does not yet inform whether to cover nodes, since the biochemical/clinical failure endpoint is immature.
- Late GI/GU toxicity beyond 12 weeks n=68 · primary completion 2025-10 · 5y cumulative GI/GU toxicity after prostate SBRTn=500 · primary completion 2027-12 · 1° EP is late GI toxicity after prostate SBRT
- Biochemical and clinical failure benefit from nodal coverage recruiting A Trial of 5 Fraction Prostate SBRT Versus 5 Fraction Prostate and Pelvic Nodal SBRT Phase 3n=1128 · primary completion 2028-06 · phase 3 prostate vs prostate+pelvic nodal SBRT, n=1128recruiting Phase II Trial of PSA Response-based Androgen Deprivation Therapy and Nodal Coverage for Prostate Cancer Early Salvage Radiotherapy (RANGER) Phase 2n=68 · primary completion 2030-11 · PSA-adapted sequential pelvic nodal RT in salvage fossarecruiting PRO-BOOST-N: Prostate-First Versus Combined Prostate and Nodal Dose Escalation in PSMA PET-Staged Node-Positive Prostate Cancer Phase 2/3n=1600 · primary completion 2033-12 · randomises nodal dose escalation in cN1M0 PSMA-staged
- Whether unmet nodal dose constraints limit delivery outside trial centres
📚 Sources · 🐦 1 tweet
Day THREE of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 17, 2026
Acute toxicity in PACE-NODES: A randomised trial of 5 fraction (f) prostate stereotactic body radiotherapy (SBRT) vs 5f prostate and pelvic nodal SBRT
Presented by Angela Pathmanathan 🇬🇧 #RadOnc ☢️ #ProstateCancer
PACE-NODES is a… pic.twitter.com/z9bAOiKSIy
PEACE-2
ForVery high-risk localized N0M0 prostate ca (≥2 of GS≥8, T3-T4, PSA≥20)
67.1% vs 62.9% at 7yr
HR 0.81, 95% CI 0.63-1.03, p=0.088; primary endpoint not met
TL;DR7yr cPFS 67.1% pelvic vs 62.9% prostate-only RT, HR 0.81 (0.63-1.03), p=0.088: primary endpoint not met.
The elective pelvic nodal decision in very high-risk N0 disease loses its randomized support: 4.2 absolute points of 7yr cPFS, HR 0.81, CI crossing 1. Staging was conventional or choline PET, so pts PSMA PET would now upstage sat in both arms, diluting any true nodal benefit. Toxicity by arm not reported in source.
Also covered May 18

| Arm | 7yr cPFS | HR (95% CI) | p |
|---|---|---|---|
| Pelvic RT | 67.1% (61.6-72.2) | 0.81 (0.63-1.03) | 0.088 |
| Prostate-only RT | 62.9% (57.4-68.1) | n/a | n/a |
+2 more figures


7 details 5 trials watching
International multicenter randomized trial with four arms crossing RT volume (prostate vs pelvis) with cabazitaxel ×4 cycles, all on ADT ×3 years. Readout presented at ESTRO 2026 with 7-year outcomes and follow-up extending to 120 months.
Very high-risk localized prostate cancer defined as ≥2 risk factors among Gleason ≥8, T3-T4, and PSA ≥20 ng/mL. N0M0 by conventional imaging or choline PET/CT.
The randomized comparison is target volume: prostate-only versus pelvic irradiation. Dose, fractionation, and nodal CTV definition are not reported in the source.
Primary: cPFS. Secondary: PSA response at 3 months, bPFS, metastasis-free survival, CaP-specific survival, OS, acute and long-term tolerance, QoL, and biopsy biomarkers.
Pelvic RT did not significantly improve cPFS on multivariable analysis. Secondary endpoints including MFS, CaP-specific survival, and OS are not reported in the source.
Effect estimate is from multivariable analysis; the 2×2 cabazitaxel randomization complicates attribution of the RT-volume effect. RT-attributable GU/GI toxicity by arm is not reported in source, which is the other half of the elective-nodal decision.
The investigators' own conclusion pivots from the RT question to the definition of "very high-risk": with <1 in 10 men dying of prostate cancer in the first decade, the population may be over-labeled. They call for biomarkers to guide intensification or de-intensification rather than uniform volume escalation.
Randomised, prespecified primary cPFS, mature 7yr readout, null result against a widely adopted practice. Design internally valid; the divergence is the headline.
In very high-risk localized N0M0 prostate cancer staged without PSMA PET, this questions routine whole-pelvis coverage over prostate-only RT with 3yr ADT; it does not speak to pts with PSMA-detected nodal disease, who were not enrolled.
- Does pelvic RT help when PSMA PET stages N0 more accurately? recruiting Extended vs. No Pelvic Lymph Node Dissection During Radical Prostatectomy. DISSECTION 2.0. Phase NAn=400 · primary completion 2027-02 · ePLND vs none in PSMA-PET node-negative high-riskn=250 · primary completion 2031-05 · randomises PORT vs whole-pelvis RT in PSMA-N0M0 pts
- RT-attributable late GU/GI toxicity by target volume n=700 · primary completion 2021-12 · longitudinal GU/GI/heme toxicity after WPRT, n=700n=400 · primary completion 2027-03 · late GI toxicity endpoint, whole-pelvis protons vs photons
- Biomarkers to select pts for treatment intensification vs de-intensification recruiting Treatment of High-Risk Prostate Cancer Guided by Novel Diagnostic Radio- and Molecular Tracers Phase 2/3n=493 · primary completion 2030-07 · tracer-guided darolutamide intensification + de-intens arm
📚 Sources · 🐦 1 tweet
📣@PBlanchardMD shows #ESTRO26 that pelvic #radiotherapy in high risk #prostatecancer does not have a large improve in outcomes.
— Shankar Siva (@_ShankarSiva) May 17, 2026
- With only 1 in 10 dying of prostate cancer in 10 years, are these patients truly “high risk”? #pcsm #radonc pic.twitter.com/D0XrGD6iNX
OLIGOMA NCT04495309
ForOligometastatic breast, ≤5 lesions, any line, mostly ER+/HER2- first line
35.8 vs 20.4 mo, HR 0.48
95% CI 0.25-0.91, p=0.021
TL;DRmPFS 35.8 vs 20.4mo, HR 0.48 (0.25-0.91), p=0.021 for MDT to all lesions in oligometastatic breast, QoL non-inferior.
The RT read is who was actually irradiated: 2/3 of lesions were bone and >80% of pts had 1-3 mets, so this is largely bone-directed ablative RT in first-line ER+ disease, not a visceral-oligomet population. Dose and fractionation are not reported in source, which gates transfer to practice. QoL non-inferiority at 12wk (-2.1, margin -10) removes the main argument against adding local therapy to a working systemic backbone.

+3 more figures

| Arm | QLQ-C30 mean at 12wk (95% CI) | Between-group change (ANCOVA) |
|---|---|---|
| Experimental | 72.2 (67.2-77.2) | -2.1 (-9.2-5.1) |
| Control | 74.3 (69.3-79.3) | n/a |


9 details 5 trials watching
Randomised trial (ARO-2021-09, NCT04495309) of systemic therapy alone vs systemic therapy plus local ablative radiotherapy to all metastatic lesions. Randomisation stratified by type of systemic therapy and treatment line. N=87 (43 experimental, 44 control).
Metastatic breast cancer, any treatment line, maximum 5 metastatic lesions, with the systemic regimen determined by multidisciplinary tumour board. Pts requiring palliative RT to all metastases were not eligible, though palliative RT to symptomatic sites was allowed. Median age 58 / 59; ECOG 0 in 76.7% of the experimental arm.
The intervention is local ablative radiotherapy to all metastatic lesions on top of the systemic backbone. Dose, fractionation, modality, and target-volume definition are not reported in the source slides, and 2/3 of treated lesions were bone metastases.
Co-primary: progression-free survival and quality of life (EORTC QLQ-C30) at 12 weeks post-randomisation. Secondary: overall survival, toxicity, compliance, QLQ-C30 and QLQ-BR23, and patient satisfaction with cancer care (EORTC PATSAT C33).
Both co-primaries read out in favour of adding MDT: PFS separated at HR 0.48 and the QoL summary score met non-inferiority against a -10 point margin. See the figure captions for the arm-level values.
Recruitment stopped early at <20% of the initial and <40% of the amended target, leaving N=87 and a wide HR CI (0.25-0.91). Open-label design with a patient-reported co-primary. No OS data reported in source, and the toxicity secondary endpoint is likewise absent from the presented slides.
The presenter frames this as the first RCT showing a PFS benefit from MDT in oligometastatic breast cancer, extending the STOMP / SABR-COMET line of evidence into a histology where systemic control is comparatively good. Eight further randomised trials are accruing, so the magnitude here should be read as provisional.
Randomised but stopped early at <20% of initial accrual target; N=87 with wide HR CI (0.25-0.91). Underpowered for a durable PFS estimate.
In ER+/HER2- breast cancer with 1-3 mostly bony metastases on first-line systemic therapy, this supports discussing ablative RT to all lesions as a PFS-directed addition; it does not extend to >5 lesions, heavily visceral disease, or pts needing palliative RT to every site.
- Does the PFS benefit translate to overall survival n=340 · primary completion 2026-11 · JCOG phase 3 MDT vs systemic alone, 340 pts
- Which oligometastatic breast subgroups benefit most active Standard Treatment +/- SBRT in Solid Tumors Patients With Between 1 and 5 Bone-only Metastases Phase NAn=168 · primary completion 2025-07 · SBRT vs none in 1-5 bone-only mets, breast inclrecruiting BreCLIM-2 - A RCT Investigating Local Treatment for Breast Cancer Liver Metastases Phase 3n=200 · primary completion 2029-12 · RCT of local tx in 1-4 breast liver metsnot yet Adding Surgery and Radiation to the Usual Treatment for HER2-Positive Breast Cancer That Had Already Spread at Diagnosis Phase 3n=562 · primary completion 2032-05 · HER2+ de novo stage IV, 1-5 mets, SBRT added
- Optimal RT dose and fractionation for bone-dominant oligomet breast recruiting OligoCare TwiCs (Trials Within Cohorts) Trial Comparing Acute Toxicity in Single-fraction vs Multiple-fraction SBRT for Metastasis-directed Treatment (SPRINT) Phase NAn=302 · primary completion 2029-02 · single-fraction vs multifraction SBRT, breast incl
📚 Sources · 🐦 3 tweets
📌 Metastases-directed treatment in Patients with Oligometastatic Breast Cancer: Results from the OLIGOMA-trial (ARO-2021-09, NCT04495309) @DavidKrugMD 👏🏻 #ESTRO26 @ESTRO_RT @OncoAlert #OncoAlertAF pic.twitter.com/YDMef0fXRm
— Elisabetta Bonzano MD, PhD (@to_be_elizabeth) May 17, 2026
❗️ The OLIGOMA trial results just dropped at #ESTRO26 and they are massive. A 15-month improvement in median PFS for OMD breast cancer (HR = 0.48). This adds to the growing mountain of evidence that MDT (Metastasis-Directed Therapy) works. Lets’s go 🧵 1/n pic.twitter.com/5uiEVSYtdH
— NonsparseOncologist (@5_utr) May 17, 2026
Here are some details!
— Jeff Ryckman (@jryckman3) May 17, 2026
On OLIGOMA, nearly 3/4 were first line endocrine or chemotherapy. #ESTRO26 #OncTwitter@CJTsaiMDPhD pic.twitter.com/r3kJzNNsyK
APBI-IMRT Florence NCT02104895
ForPost-BCS early breast cancer, pT <25mm, margins ≥5mm, age >40
7.7% vs 4.2% at 15yr
HR 1.57 (95% CI 0.82-3.04), p=0.17
TL;DR15yr IBTR 7.7% APBI vs 4.2% WBI, HR 1.57 (0.82-3.04) p=0.17; excess is new primaries, not true local relapse.
The 15yr excess sits in new ipsilateral primaries (5.9% vs 2.7%, p=0.09), not true local relapse (2.1% vs 1.6%). That splits the decision: 30Gy in 5# to the tumour bed holds the bed, but leaves untreated breast tissue at risk, which is a surveillance and endocrine-adherence question rather than an argument for whole-breast coverage.

| Endpoint (15-year) | APBI N (%) | WBI N (%) | P-value |
|---|---|---|---|
| Ipsilateral breast tumour recurrence | 20 (7.7) | 11 (4.2) | 0.14 |
| Local relapse | 5 (2.1) | 4 (1.6) | 0.75 |
| New ipsilateral breast cancer | 15 (5.9) | 7 (2.7) | 0.09 |
| Locoregional tumour recurrence | 20 (7.2) | 13 (5.0) | 0.28 |
| Contralateral breast tumour | 10 (3.8) | 13 (5.0) | 0.67 |
| Distant metastasis | 7 (2.7) | 12 (4.6) | 0.35 |
| Deaths | 56 (21.5) | 51 (19.6) | 0.66 |
+2 more figures


10 details 1 trial watching
Phase III equivalence trial, n=520, 1:1 randomisation, accrued 2005-2013, single institution. Powered on a 5-year estimated IBTR of 3% with a 5% equivalence margin and 80% power. Survival outcomes analysed ITT; toxicity and cosmesis per protocol after 14 withdrawals.
Post breast-conserving surgery, pT <25 mm, final surgical margins ≥5 mm, age >40 years. Nodal status and receptor subtype not specified in the source slides.
APBI arm: 30 Gy in 5 fractions IMRT to the partial breast. WBI arm: 50 Gy in 25 fractions plus a 10 Gy in 5 fraction tumour-bed boost. The comparator is a conventionally fractionated whole-breast course, not a modern hypofractionated 26 Gy/5 or 40 Gy/15 schedule.
IBTR HR 1.57 (95% CI 0.82-3.04), p=0.17 at 15 years. The gap widens across timepoints (5yr 2.3% vs 1.2%, 10yr 4.2% vs 2.7%, 15yr 7.7% vs 4.2%) but never reaches significance.
The only 5-fraction PBI dataset reporting to 15 years. IMPORT LOW and NSABP B-39 support PBI at shorter follow-up with different fractionation, so this trial carries the durability question for the ultrahypofractionated schedule specifically.
Powered for 5-year equivalence, so the 15-year read is descriptive rather than a met endpoint. Single institution. The local relapse vs new primary split that carries the interpretation is investigator-adjudicated, not molecularly confirmed.
Randomised phase III, prespecified 5yr equivalence endpoint, 15yr mature f/u, no significant divergence on any oncologic endpoint. Reinforces PBI as a listed option.
In the post-BCS pt over 40 with a pT <25mm tumour and ≥5mm margins, this supports 5-fraction PBI as a durable option out to 15 years; it does not extend to node-positive disease, close margins, or younger pts, and the untreated-breast new-primary rate is the tradeoff to counsel.
- Does the new-primary excess keep widening past 15 years
- Do modern hypofractionated WBI schedules change the comparison recruiting Ultra-hypofractionated for Whole Breast Irradiation (WBI) Compared to Partial Breast Irradiation (PBI) Phase 2n=100 · primary completion 2026-05 · randomised 26 Gy/5 fx WBI vs same-dose PBI
📚 Sources · 🐦 1 tweet
📌 Fifteen-year outcomes of the randomised APBI-IMRT Florence phase Ill trial of partial versus whole-breast irradiation in early breast cancer ✨
— Elisabetta Bonzano MD, PhD (@to_be_elizabeth) May 17, 2026
Excellent presentation led by @CarlottaB 👏🏻#ESTRO26 @Icro_Meattini @ESTRO_RT @OncoAlert #OncoAlertAF pic.twitter.com/1j4bIA2nyC
DBCG RT Natural
For≥60yr, pT1N0 unifocal non-lobular ER≥10% HER2-normal grade 1-2, margin ≥2mm
1.5% vs 9.8%
+RT 2/236 (0.3-5.1%) vs -RT 19/272 (5.9-14.9%)
TL;DR5yr invasive LR 1.5% with PBI vs 9.8% randomised no-PBI vs 8.2% self-selected no-PBI; RT+ET arm had zero events.
The RT read is the 2x2: +RT+ET was 0/105 events while -RT-ET hit 12.2%, and +RT-ET (3.0%) tracked -RT+ET (3.7%). PBI at 40Gy/15fr can therefore substitute for endocrine therapy in a woman who will not take or tolerate ET, rather than only supplement it.

| Study arm | Events/Total | CIF % (95% CI) |
|---|---|---|
| +RT | 2/236 | 1.5 (0.3-5.1%) |
| -RT | 19/272 | 9.8 (5.9-14.9%) |
| S-RT | 18/278 | 8.2 (4.5-13.3%) |
+2 more figures


10 details 4 trials watching
Phase III randomised Danish (DBCG) trial of PBI vs no PBI after breast conservation, stratified by institution and ET yes/no, with a third self-selecting no-PBI cohort. Planned 926 randomised, interim at 200 pts with 2yr f/u; median follow-up 4 years at this first report.
≥60 years, unilateral unifocal pT1N0 breast cancer, non-lobular, ER≥10%, HER2 normal, grade 1-2, limited DCIS, margin ≥2mm, treated with breast conservation. ET given per DBCG guideline (recommended for pT1c and/or grade 2).
Partial breast irradiation, 40Gy in 15 fractions. No whole-breast or nodal arm, so the result speaks to PBI specifically, not to omission of comprehensive breast RT.
Primary: 5-year invasive local recurrence, assumed 2% with an accepted maximum of 4%. Secondary: loco-regional side effects and QoL, neither reported in source.
All 41 recurrences were invasive, 36 isolated, and 39 of 41 occurred in pts without PBI. Distant failure was rare (4 events, 2 per group). The no-RT arms crossed the prespecified 4% threshold.
PRIME II and CALGB 9343 licensed RT omission in older low-risk pts on the strength of low absolute LR with ET, but both assumed ET adherence. Here the -RT -ET group reached 12.2%, which is the population omission actually creates when ET is declined or stopped.
Median f/u 4 years for a 5-year endpoint, and the trial was stopped early by the DMC, both of which favour an inflated effect estimate. The self-selecting no-PBI cohort is not randomised, and the 2x2 treatment-received analysis is not the randomised comparison. Toxicity and QoL, the secondary endpoints that would price the cost of PBI, are not in source.
The discussant framed it as RT or ET giving similar local control in low-risk pts, with surgery alone carrying high LR even here. That reframes the omission question from "can we drop RT" to "which single adjuvant modality, and what happens when the pt takes neither".
Randomised, prespecified LR endpoint, stopped early for excess recurrence without PBI. Directly contests RT omission in the ≥60yr low-risk group PRIME II / CALGB 9343 licensed.
In a woman ≥60 with pT1N0 grade 1-2 ER+ HER2-normal disease after breast conservation, this questions omitting PBI on PRIME II grounds, particularly where ET adherence is doubtful; it does not speak to lobular histology, ER<10%, or node-positive disease.
- Does the 1.5% LR hold at the full 5-year endpoint
- PBI toxicity and QoL vs endocrine therapy in this group n=168 · primary completion 2030-07 · 30 vs 26 Gy/5 fx APBI, 1° breast-related QoL
- Whether 5-fraction PBI reproduces this local control recruiting Accelerated Partial Breast Irradiation (APBI) Using Stereotactic Body Radiation Therapy (SBRT)n=200 · primary completion 2024-08 · 30 Gy/5 fx APBI registry, 5y f/u, n=200n=134 · primary completion 2029-08 · single-fx vs 5-fx APBI, 1° local controln=910 · primary completion 2029-11 · phase 3 5-fx PBI vs WBI, 1° LR non-inferiority
📚 Sources · 🐦 2 tweets
Another trial showing even for lR optimal local control with RT and ET and suboptimal adherence to ET. In era of 5 fraction decision making is easier # Estro2026 pic.twitter.com/nkvYl3iuTn
— Sushil (@Sushilberiwal) May 17, 2026
Danish #breastcancer partial breast #radiotherapy “natural” trial.
— Shankar Siva (@_ShankarSiva) May 17, 2026
➡️ No postoperative treatment had highest risk of recurrence
➡️either tamoxifen or #radonc reduced recurrence
➡️combined tamoxifen + RT had no recurrences
In context of EUROPA trial, RT has best QoL vs endocrine… pic.twitter.com/bDVmbDKRNb
EORTC IM-MS (22922/10925)
ForStage I-III breast cancer, incl. pN0, considering IM + medial supraclavicular RT
61.0% vs 61.8%
HR=1.00; 95% CI 0.90-1.10, P=0.967 (ns)
TL;DR20yr OS 61.0% vs 61.8%, HR 1.00 (0.90-1.10), P=0.967: early 15yr survival signal gone, BCM benefit offset by non-BCM deaths.
The mortality split is the RT read: BCM 18.6% vs 22.4% (HR 0.82) bought at a non-BCM cost of 20.4% vs 15.8% (HR 1.26), with cardiac disease 15.2% vs 11.7%. Since DBCG IMN2 heart doses ran 4-9× lower, the target-volume decision hinges on achievable MHD, not on abandoning IM coverage.

| Endpoint | IM-MS RT | No IM-MS RT | HR (95% CI) | P |
|---|---|---|---|---|
| BCM | 18.6% | 22.4% | 0.82; 0.72-0.95 | 0.006 |
| non-BCM | 20.4% | 15.8% | 1.26; 1.09-1.46 | 0.002 |
+3 more figures


| RT-related side effect | IM-MS RT | No IM-MS RT |
|---|---|---|
| Lung fibrosis | 6.3% | 3.2% |
| Cardiac fibrosis | 2.7% | 1.7% |
| Cardiac diseases | 15.2% | 11.7% |

| Endpoint (pN0) | IM-MS RT | No IM-MS RT | HR (95% CI) | P |
|---|---|---|---|---|
| DFS | 53.9% | 53.6% | 0.93; 0.81-1.07 | 0.318 |
| DMFS | 67.2% | 67.4% | 0.93; 0.78-1.10 | 0.397 |
8 details 5 trials watching
Randomised EORTC phase 3 (22922/10925), stage I-III breast cancer, ± internal mammary and medial supraclavicular irradiation. This is the 20-year ITT readout, presented as an ESTRO 2026 plenary, with a prespecified pN0 analysis.
The randomised question is target volume, not dose: adding IM-MS fields to standard breast/chest-wall treatment. Dose and fractionation are not reported in source. Mean heart dose is the operative technical variable, and the discussant contrasts it with DBCG IMN2 (MHD 1.2 Gy right-sided, 2.3 Gy left-sided, 4-9× lower than in this trial).
Primary: overall survival (ITT). Secondary reported here: DFS and DMFS (DATECAN definitions, so DFS includes all deaths and all breast events including DCIS and contralateral), breast-cancer mortality, non-breast-cancer mortality, second cancers, and late RT toxicity.
OS was flat at 20 years (HR=1.00, P=0.967), as were DFS 48.2% vs 49.0% (HR=0.97, P=0.515) and DMFS 58.9% vs 59.8% (HR=0.97, P=0.578). The signal sits in the competing-mortality split shown in the table above, not in any composite endpoint.
Cardiac disease 15.2% vs 11.7%, lung fibrosis 6.3% vs 3.2%, cardiac fibrosis 2.7% vs 1.7%. No statistical difference in second cancers or second breast cancers between arms, so the excess non-breast-cancer mortality tracks with cardiopulmonary late effects rather than second malignancy.
DBCG IMN2 (irradiation 2007-2014) reported reduced distant metastasis, reduced BCM and improved OS in node-positive pts at 15 years, with mean heart doses 4-9× lower than here. The two trials disagree on OS, and heart dose is the most plausible discriminator.
Toxicity and the competing-mortality penalty are technique-era dependent; RT dose, fractionation and delivery details are not reported in source. The pN0 analysis is a subgroup, though the null OS is the trial-level primary result.
The 15-year positive read did not hold to 20 years because non-breast-cancer deaths kept accruing. The clinical question shifts from whether IM-MS coverage works (it lowered BCM) to whether the heart dose it costs can be made small enough to let that benefit surface in OS.
Randomised, prespecified OS primary, 20y follow-up, now null after a positive 15y read. Divergence is internally valid; era-dependent heart dose is the caveat, not a design flaw.
In pN0 stage I-III breast cancer this does not support adding internal mammary and medial supraclavicular coverage (DFS HR 0.93, P=0.318); it does not settle the node-positive question, where modern low heart-dose technique still carries a 15-year benefit signal.
- Does IM-MS benefit survive at modern mean heart doses?
- Which node-positive subsets justify IM coverage? active Standard or Comprehensive Radiation Therapy in Treating Patients With Early-Stage Breast Cancer Previously Treated With Chemotherapy and Surgery Phase NAn=1636 · primary completion 2023-09 · randomised comprehensive nodal vs standard RT fieldsrecruiting RecurIndex Guided Avoidance of Regional Nodal Irradiation for Node Positive Breast Cancer Phase NAn=540 · primary completion 2029-08 · RecurIndex-gated RNI in clinically low-risk N1
- Do proton or DIBH techniques eliminate the non-BCM excess? recruiting Robustness Evaluation of Deep Inspiration Breath-Hold (DIBH) Plans in Internal Mammary Irradiationn=25 · primary completion 2026-12 · DIBH dose coverage + OAR params in IM irradiationn=220 · primary completion 2027-01 · proton locoregional RT, 10-15y cardiac mortality + SMNn=750 · primary completion 2027-12 · IMPT vs IMRT/VMAT, cardiac + lung toxicity endpoints
📚 Sources · 🐦 2 tweets
📌 Internal Mammary and Medial Supraclavicular irradiation in stage I-III breast cancer: 20 years results of the randomised EORTC trial 22922/10925, including in pNo patients
— Elisabetta Bonzano MD, PhD (@to_be_elizabeth) May 17, 2026
Special Joint Presentation Led by Prof. Philip Poortmans and Orit Kaidar-Person ✨ at #ESTRO26 @ESTRO_RT… pic.twitter.com/KIoJtdhEzp
20-year outcomes of @EORTC internal mammary #radiotherapy trial.
— Shankar Siva (@_ShankarSiva) May 17, 2026
➡️internal mammary improved control
➡️ survival counterbalanced by late adverse events #radiotherapy #bcsm
Great to see the long term data at #ESTRO26, and discussing Charlotte Cole suggests with modern RT, long… pic.twitter.com/yPtlfrLcri
IMPORT HIGH
ForInvasive early breast pT1-3 pN0-pN3a M0 post-BCS requiring tumour bed boost
3.5% vs 3.7% vs 5.5% at 10yr
95% CI 2.4-5.0 / 2.6-5.3 / 4.1-7.3
TL;DR10yr IBTR 3.5% vs 3.7% vs 5.5% across 40+16Gy, 48Gy SIB, 53Gy SIB; further escalation adds nothing.
The transferable parameter is 48Gy/15F in 3 weeks with the boost built in, no separate 8-fraction phase, holding IBTR at 3.7% at 10yr with moderate/marked distortion under 18%. The 53Gy arm settles the escalation question: 5.5% IBTR, worse not better, so the decision this moves is boost delivery (SIB vs sequential), not boost dose.

| Arm | 10-yr IBTR (95% CI) | Absolute OS diff vs 40Gy/15F |
|---|---|---|
| 40Gy/15F + 16Gy/8F | 3.5% (2.4, 5.0) | reference |
| 48Gy/15F (3.2Gy/F) | 3.7% (2.6, 5.3) | -0.5 (-3.0, 2.8) |
| 53Gy/15F (3.5Gy/F) | 5.5% (4.1, 7.3) | 1.5 (-1.4, 5.1) |
+2 more figures

| Arm | N | 5-yr IBTR (95% CI) |
|---|---|---|
| 40Gy/15F + 16Gy/8F | 871 | 1.9% (1.2, 3.1) |
| 48Gy/15F (3.2Gy/F) | 874 | 2.0% (1.2, 3.2) |
| 53Gy/15F (3.5Gy/F) | 872 | 3.2% (2.2, 4.7) |

9 details 4 trials watching
Phase 3 randomised 1:1:1, N=2617 across 76 UK hospitals, accrued 2009-2015. Annual clinical follow-up to 10 years; PROs and photographs collected only to 5 years.
Women ≥18 years after breast conserving surgery for invasive early breast cancer, pT1-3, pN0-pN3a, M0, all requiring tumour bed boost RT. Described by the investigators as a higher-than-average risk group.
Control was 40Gy/15F whole breast plus sequential 16Gy/8F boost. Both experimental arms used a simultaneous integrated boost in 15 fractions over 3 weeks, 48Gy (3.2Gy/F) or 53Gy (3.5Gy/F) to the tumour bed, with a modest dose reduction to whole breast distant from the tumour.
Primary: ipsilateral breast tumour relapse (IBTR), reported here at 10 years. Secondary reporting covers overall survival and clinician-assessed late normal tissue effects.
Moderate/marked AEs at 10 years were low across all randomised groups: breast distortion/shrinkage <18%, induration <10%, telangiectasia <2%, breast oedema <2%. No arm-specific late toxicity split is given in the source.
At 5 years (Coles, Lancet 2023) IBTR was 1.9% / 2.0% / 3.2%, and 48Gy was declared non-inferior in absolute terms. The 10-year data preserve that ordering, and both 40+16Gy and 48Gy stay below the 5% control estimate assumed in the original sample size calculation.
Source reports absolute rates only, no between-arm HRs or non-inferiority p-values at 10 years. PRO and photographic cosmesis stopped at 5 years, so 10-year toxicity is clinician-scored. Conference presentation, not yet a full peer-reviewed 10-year report.
The practical yield is logistic as much as oncologic: SIB collapses boost into the same 15 fractions, cutting visits without paying an IBTR or late-toxicity penalty. Further escalation to 53Gy does not help, which closes the dose-escalation arm of this question in a boost-indicated population.
Randomised 3-arm phase 3, prespecified 10-yr follow-up of a published primary; reaffirms 48Gy/15F SIB rather than changing it. No new comparator.
In pT1-3 pN0-pN3a post-BCS pts you would otherwise book for 40Gy/15F plus a sequential 16Gy boost, this supports a 15-fraction 48Gy SIB as an equivalent-control option; it does not speak to boost omission in low-risk pts, who were not the population studied.
- Does SIB benefit extend to post-mastectomy or nodal RT settings?
- Which boost-indicated subgroups could safely omit boost entirely? n=295 · primary completion 2029-11 · RT omission in low-risk DCIS, age >=50
- Five-fraction SIB as the next de-escalation step? recruiting Ultra-hypofractioNated Adjuvant Radiotherapy ± sImultaneous Integrated Boost for Low-risk Breast Cancer Patients Phase 2n=65 · primary completion 2025-10 · phase 2 ultrahypofx WBI +/- SIB, feasibilityn=50 · primary completion 2029-02 · ultra-short WBI with SIB, cosmesis + PROM endpointsrecruiting 5 fr Ultrahypofractionated WBI and SIB for Breast Cancer With Unfavorable Characteristics Phase NAn=458 · primary completion 2029-06 · randomised 26/30Gy 5fr SIB vs 40.05/48Gy 15fr SIB
📚 Sources · 🐦 1 tweet
Day THREE of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 17, 2026
Ten-year results of the IMPORT HIGH trial (ISRCTN47437448): Dose escalated simultaneous integrated boost radiotherapy in early breast cancer Presented by Charlotte Coles 🇬🇧 #RadOnc ☢️
Ten-year IMPORT HIGH trial data show that a… pic.twitter.com/7RqVy2SrQm
HypoG-01
ForBreast cancer receiving adjuvant RT + tumour-bed boost per HypoG-01 eligibility
TL;DR118 first events at 4.8y median f/u; LRR infrequent and mostly in-volume, patterns comparable between 40Gy/15fx and 50Gy/25fx.
The contouring read matters more than the fractionation read here: 20/30 recurrence sites fell in-volume and 19/30 nodal recurrences sat in L1-L2, so ESTRO CTV definitions covered where disease actually came back. That supports keeping current axillary level coverage rather than expanding target volumes when moving to 40 Gy/15 fx.

| Event type | n |
|---|---|
| Isolated LRR | 19 |
| Concomitant LRR | 1 |
| Isolated distant recurrence | 61 |
| Second malignancy | 37 |
| Total first events | 118 |
+1 more figure

9 details
Pre-planned secondary analysis (ITT) of the HypoG-01 phase III randomised trial. N=1,260, median follow-up 4.8 years.
Randomisation was 40 Gy/15 fractions over 3 weeks vs 50 Gy/25 fractions over 5 weeks, each with a tumour-bed boost. Target volumes followed ESTRO contouring guidelines.
First oncological event: locoregional recurrence (LRR), distant recurrence (DR), or second malignancy. LRR classified against the CTV as in-volume, marginal (outside CTV, ≥50% prescribed dose), or out-of-volume (<50%), with planned dose at the recurrence site re-estimated on the initial RT-plan CT.
118 first events. LRR was the lowest-frequency event type; distant recurrence (n=61) and second malignancy (n=37) dominated. 20/30 recurrence sites were in-volume (67%) and 19/30 nodal sites were mainly levels I and II.
Arm-level event counts are not reported in the source, so the "no obvious difference" claim between arms cannot be checked. With roughly 20 LRR events total, the analysis is descriptive and underpowered to exclude a modest fractionation effect on failure pattern.
The actionable signal is target-volume adequacy rather than fractionation: recurrences clustered inside the treated volume and in axillary levels I-II, which argues the ESTRO CTV is catching the right anatomy rather than that coverage needs widening. Out-of-volume failures would have been the argument for larger fields; they were the minority.
Pre-planned secondary analysis of a randomised phase III; supports moderate hypofractionation and ESTRO contouring. Event count (19 iLRR) too small for a powered arm comparison.
In breast pts eligible for adjuvant RT with a tumour-bed boost, this supports 40 Gy/15 fx with standard ESTRO-guided CTVs without widening nodal volumes; it does not address ultra-hypofractionation or pts whose recurrence risk sits outside the trial's eligibility.
- Do failure patterns hold with ultra-hypofractionation (5-fraction) schedules?
- Does boost technique alter in-volume vs marginal recurrence distribution?
📚 Sources · 🐦 1 tweet
Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 16, 2026
Patterns of locoregional and distant recurrence and dosimetric analysis in the HypoG-01 phase III trial Presented by Louis Munschi 🇫🇷 #RadOnc ☢️
In the HypoG-01 phase III trial (1260 patients, median follow-up 4.8 years), 118… pic.twitter.com/ogARInu0fB
DBCG HYPO
ForNode-negative early breast cancer or DCIS after breast-conserving surgery
24.7% vs 19.5% at 10 yr
HR 0.76 (95% CI 0.62-0.92), p=0.005 favouring 40 Gy/15 fx
TL;DR10-yr grade 2-3 breast induration 19.5% with 40Gy/15fx vs 24.7% with 50Gy/25fx, HR 0.76, p=0.005; no recurrence or survival cost.
The induration difference is not just non-inferiority, it favours 40 Gy/15 fx (24.7% vs 19.5%, HR 0.76, p=0.005), so the shorter course is the lower-fibrosis option, not merely the more convenient one. Applies to node-negative and DCIS whole-breast fields; boost and nodal coverage are not addressed in source.

| Endpoint | 50 Gy/25 fx | 40 Gy/15 fx | Effect size |
|---|---|---|---|
| 10-yr grade 2-3 induration | 24.7% | 19.5% | HR 0.76 (95% CI 0.62-0.92), p=0.005 |
| 10-yr overall survival | 92.1% | 93.0% | HR 0.81 (95% CI 0.63-1.04), p=0.10 |
+1 more figure

9 details 5 trials watching
Phase III randomised non-inferiority trial, 1:1, run across Denmark, Norway and Germany with accrual 2009-2014. Median follow-up 12.8 years; these are the prespecified 10-year analyses.
1,882 women with node-negative breast cancer or DCIS. Allocation was 949 to 50 Gy and 933 to 40 Gy after exclusions; 936 and 917 women respectively carried forward in the flow diagram.
Whole-breast RT only: 50 Gy in 25 fractions vs 40 Gy in 15 fractions. No boost, nodal target volume, or technique detail (IMRT vs 3D, prone vs supine) is reported in the source.
Primary: grade ≥2 breast induration at 3 years, scored at two consecutive visits or at final follow-up. Morbidity assessed at years 0, 1, 2, 3, 4, 5 and 10; recurrence and survival were prespecified 10-year secondary analyses.
Induration is the toxicity endpoint here and it favours the hypofractionated arm. No other late-effect domain (cardiac, pneumonitis, cosmesis scoring, second malignancy) is reported in the source.
Consistent with START-B and the UK long-term hypofractionation experience, but adds prospectively scored induration out to 10 years in a trial that also enrolled DCIS.
Locoregional recurrence, distant failure and breast cancer mortality are reported only as not significantly different, with no event counts, HRs, or non-inferiority margin in the source. Induration scoring is clinician-assessed and not blinded to fractionation.
Prespecified 10-yr analysis of a randomised phase III with 12.8-yr median f/u; reinforces moderate hypofractionation already standard worldwide.
In node-negative invasive breast cancer or DCIS after lumpectomy, this supports 40 Gy/15 fx over 50 Gy/25 fx on long-term induration as well as convenience; it does not speak to node-positive pts needing regional nodal irradiation.
- Does the induration advantage hold with a tumour bed boost? active Hypofractionation With Simultaneous Integrated Boost vs. Standard Fractionation in Early Breast Cancer Phase NAn=2324 · primary completion 2019-01 · hypofx + SIB vs standard fractionation, n=2324n=132 · primary completion 2026-03 · 40 Gy/15 fx + SIB boost, 4y fibrosis 1° endpoint
- How does 40 Gy/15 fx compare with 26 Gy/5 fx at 10 years? n=2100 · primary completion 2029-03 · 1 wk vs 3 wk adjuvant RT, non-inferiority, n=2100recruiting 5 fr Ultrahypofractionated WBI and SIB for Breast Cancer With Unfavorable Characteristics Phase NAn=458 · primary completion 2029-06 · randomised 26 Gy/5 fx vs 40.05 Gy/15 fx, both SIBrecruiting Ultra-Hypofractionated vs Moderate Hypofractionated Radiotherapy for Regional Lymph Nodes in High Risk Breast Cancer Phase NAn=1950 · primary completion 2034-03 · 26 Gy/5 fx vs 40 Gy/15 fx nodal RT, f/u to 2034
📚 Sources · 🐦 1 tweet
Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 17, 2026
10-year Follow-Up of the DBCG HYPO Trial: Breast Induration, Recurrence and Survival After Hypofractionated Whole Breast Irradiation Presented by Hanna Forsberg 🇩🇰 @BOffersen #RadOnc ☢️ #BreastCancer
The DBCG HYPO trial reports… pic.twitter.com/4qf9R3HZwT
Tumour bed boost after BCS + WBRT
ForPost-BCS invasive breast cancer treated with WBRT, Dutch cohort 2012-2016
TL;DR10-yr IBTR 1.2% no-boost vs 1.2% boost in 0-2 risk factors; boost omission viable in modern systemic era.
The boost arm carries HIGHER crude IBTR at every stratum (10-yr 3.3% vs 2.7% at ≥3 RF), which is confounding by indication, not harm, and it means these data cannot estimate boost efficacy at all. What they do support is a floor: with 0-2 risk factors, 10-yr IBTR is 1.2% either way, so the omission decision rests on that absolute rate.

| Risk factors | N no boost | N boost | 5-yr no boost | 5-yr boost | 10-yr no boost | 10-yr boost |
|---|---|---|---|---|---|---|
| 0-2 | 15,085 | 13,845 | 0.6% | 0.7% | 1.2% | 1.2% |
| ≥ 3 | 149 | 733 | 1.3% | 2.9% | 2.7% | 3.3% |
| Uncertain | 592 | 944 | 0.8% | 3.3% | 1.4% | 3.6% |
+2 more figures


9 details
Dutch population-based cohort (DBRT / Netherlands Cancer Registry linkage) of breast-conserving treatment, 2012-2016. Non-randomised: boost use reflects clinician risk assessment, not allocation.
Breast conserving treatment with or without an RT boost. Strata by number of risk factors: 0-2 (15,085 no boost / 13,845 boost), ≥3 (149 / 733), uncertain (592 / 944).
Whole-breast RT with or without tumour bed boost. No dose, fractionation, boost technique, or target-volume detail reported in source.
Primary: ipsilateral breast tumour recurrence (IBTR), histologically confirmed via a pathology-report text/code algorithm. Cumulative incidence reported at 5 and 10 years by risk-factor count.
Low IBTR across every subgroup. Only the ≥3 risk-factor boost group crossed an Assisi threshold at 10 years (3.3%, vs the <3% bar).
EORTC 22881-10882 anchored the ~50% relative IBTR reduction from boost. Absolute IBTR here is an order of magnitude below that trial's era, which is the authors' argument that a relative halving now buys little absolute benefit.
Confounding by indication is the dominant issue: higher-risk pts got the boost, so crude boost-arm rates run higher. The ≥3 RF no-boost cell is 149 pts. 10-yr estimates on a 2012-2016 cohort are projected, and IBTR ascertainment was algorithmic.
Registry cohort with non-random boost allocation; confounding by indication and a 149-pt no-boost ≥3 RF stratum undercut the omission claim.
In post-BCS pts with 0-2 of the listed risk factors receiving WBRT, this supports discussing boost omission on absolute-risk grounds; it does not inform pts with ≥3 risk factors, where the ≥3 RF no-boost stratum is only 149 pts.
- Which ≥3 risk-factor subgroups actually gain from a boost
- Does boost omission hold with longer observed follow-up
- Boost value in pts with residual disease after neoadjuvant therapy
📚 Sources · 🐦 1 tweet
Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 16, 2026
Is a boost to the tumour bed still indicated after breast-conserving surgery and whole-breast radiotherapy in the era of modern systemic therapy? Presented by Femke Froklage 🇳🇱 #RadOnc ☢️
We aimed to identify a subgroup of breast… pic.twitter.com/RqK5r9XPqW
RCC SBRT local control
TL;DR100% local control at 5 years for primary RCC treated with SBRT, per a conference tweet with no denominator.
The RT-relevant gap is technique: no dose, fractionation, or tumor-size cap is in the source, and those are what determine whether a primary-RCC SBRT local-control figure transfers to a reader's practice. Without them this does not move the SBRT vs partial nephrectomy or ablation decision.
6 details
Not reported in source. The tweet gives no phase, sample size, sites, or accrual period; the underlying series cannot be identified from the text provided.
No dose, fractionation, or technique reported in source. Primary-RCC SBRT regimens vary widely across published series, so the local-control claim cannot be attributed to a specific regimen.
100% local control at 5 years is the only figure in the source. No denominator, no confidence interval, and no local-control definition accompany it.
Single social-media claim without a linked abstract, figure, or registration. Local control alone omits the renal-function and cancer-specific-survival endpoints that gate modality choice in primary RCC.
Single tweet with a bare local-control percentage; no N, design, dose, or follow-up definition to classify against. Underlying series not identifiable from source.
- Which series does this 100% 5-yr local control come from
- SBRT vs partial nephrectomy or thermal ablation in operable primary RCC
- Renal function preservation after primary-RCC SBRT
📚 Sources · 🐦 1 tweet
These results are so impressive!! 💯 local control at 5 years for RCC treated with SBRT@DrRanaMcKay @AdityaBagrodia @DrTylerStewart @DrYukselUrun @OncoAlert https://t.co/fUB3airM5g
— Tyler Seibert MD PhD (@TylerSbrt) May 17, 2026
OligoCare
ForOligometastatic solid tumors treated with SABR; prostate/NSCLC/CRC/breast…
TL;DRReal-world SABR local in-field progression 5.0% at 1yr, 11.4% at 3yrs across 2447 pts / 3533 lesions; CRC worst.
The histology split is the actionable read: CRC 3yr in-field failure 19.6% vs prostate 8.1%, despite CRC receiving the highest median dose per fraction. That argues for dose escalation or a combination strategy in CRC mets specifically, and it puts minimum PTV dose (not prescription dose) on the plan-review checklist.

| Primary | n | 1 year | 3 years |
|---|---|---|---|
| Colorectal | 518 | 9.3% | 19.6% |
| Breast | 378 | 4.1% | 11.3% |
| NSCLC | 530 | 6.0% | 9.8% |
| Prostate | 1021 | 2.7% | 8.1% |
+2 more figures


10 details
EORTC OligoCare prospective real-world registry of SABR for oligometastatic disease, 57 institutions, accrual July 2019 to July 2025. Interim analysis; median follow-up 31 months (minimum 6).
2447 eligible pts with 3533 lesions. Median age 69 (28-94), 69% male. Primary tumors: prostate 1021 (42%), NSCLC 530 (22%), colorectal 518 (21%), breast 378 (15%).
SABR to metastatic sites; lesion locations were lung 807 (23%), non-vertebral bone 869 (25%), non-regional lymph node 558 (16%), spine 515, liver 306 (9%), brain 231 (7%), other 247 (7%). Minimum PTV dose correlated with outcome and is named the most critical technical factor; prescription dose and fractionation not reported in source.
Local in-field progression reported as cumulative incidence. No primary endpoint stated in the source; no survival or systemic-progression endpoints given here.
Local in-field progression 5.0% at 1 year and 11.4% (99% CI 10.0-12.9%) at 3 years, i.e. 88.6% local control at 3 years, 237 events among 2447 pts.
Colorectal primaries failed most (19.6% at 3 years) despite the highest median dose per fraction, which the authors read as relative radioresistance rather than underdosing and a case for dose escalation or combination approaches. De novo oligometastatic disease outperformed repeat OMD, attributed to higher delivered dose.
Registry design with no comparator arm and heterogeneous dose/fractionation across 57 centres; indication and selection bias are unaddressed in source. Safety and toxicity outcomes are not reported in the source content.
Large prospective multi-site registry with explicit histology-stratified analyses, but non-randomised and no comparator; supports rather than tests current oligomet SABR practice.
In a CRC oligomet being planned for SABR, this registry supports treating minimum PTV dose as the coverage constraint to scrutinize and sets a realistic ~1 in 5 three-year in-field failure expectation; it does not extend to unirradiated or non-oligometastatic disease.
- Optimal dose escalation strategy for colorectal oligometastases
- Minimum PTV dose threshold for durable local control
- Whether repeat OMD failure reflects dose or biology
📚 Sources · 🐦 1 tweet
📣 #ESTRO26 - @UmbertoRicardo e2irradiate @EORTC prospective OLIGOCARE registry of SABR for oligomets. ~2500 patients, ~3500 mets.
— Shankar Siva (@_ShankarSiva) May 17, 2026
➡️ local failure 5% at 1 year and 11% at 3 years
➡️ Colorectal cancer has higher risk of progression
➡️ minimum PTV dose correlated with outcome… pic.twitter.com/cx4zERqHhK
EXTEND
ForOligometastatic solid tumors, mixed histology, on standard-of-care systemic…
TL;DRPrimary aggregated analysis across all tumor-histology baskets now published in JCO; no effect sizes reported in source tweet.
The aggregated all-basket read is the gate for whether MDT generalizes beyond the single histologies that carry their own randomized data, so it moves the offer-MDT-or-not decision in mixed-histology oligomet. No effect sizes, RT dose, fractionation, or target volume appear in the source text.
Also covered May 18
7 details
Phase II randomized trial of metastasis-directed therapy added to standard of care vs standard of care alone in oligometastatic solid tumors. This report is the primary analysis of all tumor-histology baskets pooled.
No effect sizes are reported in the source, which is a tweet plus a JCO title-page image. Primary endpoint, medians, HRs, and follow-up all require the full text.
Pooling across histology baskets can obscure heterogeneity between them. MDT technique, dose, fractionation, and target volume are not stated in source, so transferability to a specific RT practice cannot be judged here.
Phase II randomized basket design caps the read at hypothesis-generating; source gives no primary endpoint, effect size, or follow-up to classify further.
- Which histology baskets drive the pooled estimate
- Whether ctDNA selects pts who benefit from MDT
- Confirmatory phase 3 in mixed-histology oligomet
📚 Sources · 🐦 1 tweet
1/ Tremendous thanks to the patients, coauthors and all who made the EXTEND trial possible. The primary aggregated analysis is now available online @JCO_ASCO with ctDNA correlatives presented synchronously at @ESTRO_RT #ESTRO26 pic.twitter.com/Zoy8DGRWbW
— Alexander Sherry (@AlexSherryMD) May 17, 2026
DIREKHT
ForResected HNSCC, post-operative RT candidates
TL;DRContralateral neck sparing and 56 Gy primary CTV de-escalation in selected post-op HNSCC; no effect sizes reported in source tweets.
The RT-relevant lever is target volume plus dose, not systemic therapy: contralateral neck sparing in a selected subgroup and a 56 Gy primary CTV. Both would move the elective-volume and dose-de-escalation decision in post-op HNSCC, but the source gives no control or toxicity numbers to weigh them against.
6 details 5 trials watching
Two de-escalation levers: contralateral neck sparing in a specified subgroup, and primary CTV dose reduced to 56 Gy. Fractionation, high-risk CTV dose, and elective nodal dose are not reported in source.
Post-operative HNSCC. The contralateral-sparing subset is described only as a "specified group"; the criteria are not in source.
Source is a single third-party commentary tweet. No design, N, endpoints, or effect sizes reported; the linked detail was not captured.
Source is a commentary tweet with no design, N, endpoints, or effect sizes. Nothing reported that supports classifying the result.
- Which subgroup safely tolerates contralateral neck sparing n=396 · primary completion 2027-12 · randomised omission of nodal RT in pN0-N1 oral cavity
- Locoregional control with 56 Gy vs standard post-op dose recruiting The Efficacy and Safety of De-escalated Postoperative Radiotherapy in Locally Advanced HNSCC With pCR/MPR Phase NAn=23 · primary completion 2027-04 · PORT 50 Gy vs standard 60 Gy after pCR/MPRrecruiting Transoral Surgical Resection Followed by De-escalated Adjuvant IMRT in Resectable p16+ Locally Advanced Oropharynx Cancer Phase 2n=150 · primary completion 2028-12 · risk-stratified de-escalated adjuvant IMRT post-TORS
- Late toxicity and swallowing outcomes after volume plus dose de-escalation n=33 · primary completion 2026-01 · reduced-dose RT post-TORS, long-term toxicity focusrecruiting Preservation of Swallowing in Respected Oral Cavity Squamous Cell Carcinoma: Examining Radiation Volume Effects (PRESERVE): A Randomized Trial Phase 2n=90 · primary completion 2026-09 · QoL primary: omit pN0 neck RT vs full volume
📚 Sources · 🐦 1 tweet
There are tremendous opportunities to improve post-operative radiotherapy in HNSCC. The DIREKHT trial is an excellent example of such work, in which they spared the contralateral neck in a specified group of patients and/or reduced the primary CTV dose to 56 Gy.
— David Sher (@DavidSherMD) May 16, 2026
The details… https://t.co/7W84LYIofR