Early signal
10-yr SBRT for Prostate Cancer (Meier Nonrandomized Trial)
ForLow- and intermediate-risk localized prostate, no ADT, Gleason ≤7, PSA ≤20
TL;DR10-yr OS 84%, RFS 90% (94% LR, 86% IR); late G3 GU/GI ≤1.5%, no G4-5; 40Gy/5fx SBRT, no ADT, 21 centers
The unfavorable-IR subgroup is the read: 10-yr RFS 77% vs 92% favorable-IR, so SBRT monotherapy without ADT looks adequate for LR/favorable-IR but leaves unfavorable-IR pts short. 40Gy/5fx transfers directly to practice. Late GU G2+ 14% (vs GI 2.1%) is the toxicity to counsel.
9 details 4 trials watching
Investigator-initiated phase 2 nonrandomized single-arm trial, N=310 evaluable across 21 community, regional and academic centers, treated 2008-2010. Median follow-up 9 yr; 10-yr Kaplan-Meier estimates.
172 low-risk (T1b-T2a, Gleason 6, PSA ≤10) and 138 intermediate-risk (Gleason 7 with PSA ≤10, or Gleason 6 with PSA 10-20), central path review. Median age 68; prostate volume up to 100 cc; ADT not allowed.
40 Gy in 5 fractions (8 Gy×5) on a noncoplanar robotic platform with real-time motion management, dose escalated to ~100 Gy EQD2 (α/β=2).
10-yr OS 84% and overall RFS 90%; risk-group and favorable/unfavorable IR breakdown in the results table. Relapse defined as biochemical failure (nadir+2), clinical failure, or salvage/systemic therapy.
| Subgroup | 10-yr RFS |
|---|---|
| Overall | 90% |
| Low-risk | 94% |
| Intermediate-risk | 86% |
| Favorable IR | 92% |
| Unfavorable IR | 77% |
Late G3 GI/GU 1.4% LR, 1.5% IR; no grade 4-5. G2+ GI 2.1% vs GU 14%, the dominant late burden. Physician-reported CTCAE v3.
PACE-B showed SBRT noninferior to conventional EBRT at 5 yr; this extends single-arm SBRT durability to 10 yr, consistent with the cohort's prior 5-yr low-toxicity report.
Single-arm, no randomized comparator; toxicity is physician-reported (CTCAE v3), not patient-reported, so late GU burden may be understated; RFS folds salvage/systemic therapy into the relapse endpoint.
Single-arm nonrandomized phase 2; no comparator arm (PACE-B provides randomized evidence). Mature 10-yr data reassure but design caps the read below confirmatory.
In low- and favorable-intermediate-risk localized prostate (Gleason ≤7, no ADT indication), this supports ultrahypofractionated SBRT as durable at 10 yr; it does not extend to high-risk or node-positive disease, where ADT and nodal coverage remain in play.
- SBRT monotherapy sufficiency for unfavorable intermediate-risk without ADT n=310 · primary completion 2025-12 · randomized SRT +/- ADT, unfavorable intermediate risk
- 10-yr randomized SBRT vs conventional EBRT outcomes n=503 · primary completion 2028-08 · SBRT vs standard RT: local control + bDFSrecruiting PRO-BOOST-LC: Whole-Gland Boost Strategies Versus SBRT Monotherapy in PSMA-Staged Localized and Locally Advanced Prostate Cancer Phase 2/3n=1200 · primary completion 2033-12 · randomized SBRT monotherapy vs EBRT-backbone boostrecruiting Testing Shorter Duration Radiation Therapy Versus the Usual Radiation Therapy in Patients With High Risk Prostate Cancer Phase 3n=1209 · primary completion 2036-03 · phase 3 SBRT 5fx vs usual 20-45fx EBRT
📚 Sources · 📄 1 paper
ARTO NCT03449719
ForOligomet CRPC, ≤3 mets, no prior systemic mCRPC therapy, on abiraterone
TL;DRmOS NR vs 50mo, HR 0.55 (0.33-0.92, p=0.021) adding SBRT to all mets to abi+ADT in oligomet CRPC (unplanned OS analysis).
Ablative dose is the transferable read: BED ≥100 Gy in 1-5 fractions to ALL oligomet sites, and MDT added no excess grade 3-4 toxicity (the only treatment-related death was in the control arm). Extends the oligomet-MDT OS signal from hormone-sensitive disease into CRPC on an abiraterone backbone, informing whether to irradiate all sites when starting an ARSI.
Also covered Jun 12
9 details 4 trials watching
Phase 2, open-label, randomised 1:1, N=157, 16 Italian academic/community centres; stratified by centre, ECOG PS, and number of metastases. Median follow-up 53 mo (IQR 43-60). This OS read is an unplanned long-term analysis.
Prostate adenocarcinoma with metastatic castrate-resistant disease, ≤3 metastatic sites, and no prior systemic therapy for mCRPC. Control n=82, experimental n=75.
Both arms received ADT plus oral abiraterone acetate 1000 mg daily. The experimental arm added SBRT.
SBRT to all sites of metastatic disease, 1-5 fractions, biologically effective dose ≥100 Gy (ablative).
Primary: 6-month biochemical response (PSA drop ≥50%), previously met and reported. This paper reports an unplanned overall survival analysis at long-term follow-up.
OS median NR (95% CI 55-NR) experimental vs 50 mo (36-NR) control, HR 0.55 (0.33-0.92), p=0.021.
G3-4 infectious complications 5 (control) vs 0 (experimental); cardiovascular disorders 3 vs 3. One treatment-related death (myocardial failure) in the control arm. No excess toxicity from MDT.
Prior oligomet-MDT RCTs (STOMP, ORIOLE) enrolled castration-sensitive disease; ARTO extends the metastasis-directed RT signal into the CRPC setting on an ARSI backbone.
Unplanned OS analysis with post-hoc power recalculation; the trial was powered for 6-month biochemical response, not survival. Open-label, small N (157), phase 2.
Unplanned OS analysis (trial powered for 6-mo biochemical response, not survival); phase 2, N=157, open-label. Positive but hypothesis-generating pending a survival-powered phase 3.
In oligometastatic CRPC (≤3 sites, no prior systemic mCRPC therapy) starting abiraterone, this supports adding metastasis-directed SBRT; the signal does not extend to higher-volume mCRPC or the castration-sensitive oligomet setting.
- Does the OS benefit hold in a phase 3 powered for survival? recruiting Metastasis-directed Therapy in Oligoprogressive Castration-refractory Prostate Cancer Phase 3n=246 · primary completion 2029-01 · phase 3 MDT in oligoprogressive CRPC
- Optimal SBRT dose, fractionation, and site coverage in oligomet CRPC recruiting HIghly MetAstatic Life Prolonging Therapy-Resistant Prostate Cancer: Role of Stereotactic Radiotherapy for Bone and Lymph Node Metastases (HIMARS) Phase NAn=18 · primary completion 2028-05 · phase 1 SBRT max-tolerated-volume escalationrecruiting OligoCare TwiCs (Trials Within Cohorts) Trial Comparing Acute Toxicity in Single-fraction vs Multiple-fraction SBRT for Metastasis-directed Treatment (SPRINT) Phase NAn=302 · primary completion 2029-02 · single- vs multi-fraction SBRT for oligomets
- Which oligomet CRPC pts benefit most from MDT n=18 · primary completion 2023-07 · PSMA PET tests predictive value for MDT
📚 Sources · 📄 1 paper
Abstract
INDIBLADE
ForStage II/III MIBC, cT2-4aN0-2, bladder-preservation candidates
TL;DR2yr bladder-intact EFS 78% (67-90%) with induction ipi+nivo before chemoRT; 2yr OS 96% in cT2-4aN0-2 MIBC.
Cohort spans cT2-4a and clinically node-positive (N1-2), pushing bladder preservation into nodal disease that usually routes to cystectomy. The novel lever is induction ipi+nivo before chemoradiation, not the RT itself; 78% 2yr bladder-intact EFS tests whether induction dual-IO belongs in a trimodality pathway. RT dose and fractionation absent from source, so transferability stays unconfirmed.
7 details 4 trials watching
Single-arm bladder-preservation trial: induction dual checkpoint blockade followed by chemoradiation. N and site count not reported in source. Outcomes reported at 2 years.
Stage II/III MIBC, cT2-4aN0-2. Notably includes clinically node-positive (N1-2) disease, a group usually routed to radical cystectomy.
Induction ipilimumab + nivolumab (dual IO) before chemoradiation. Doses, cycles, and radiosensitizing chemotherapy not stated in source.
Chemoradiation is the definitive local component, but RT dose, fractionation, and target volume are not specified in source, gating whether the result transfers to a given practice.
Headline readout is 2yr bladder-intact event-free survival; overall survival reported alongside.
Single-arm, no comparator vs chemoRT alone or cystectomy; short 2yr follow-up; bladder-intact EFS is a composite surrogate; N and RT details absent from source.
Single-arm, no comparator vs chemoRT alone or cystectomy; 2yr follow-up; bladder-intact EFS a composite surrogate. Hypothesis-generating induction-IO-plus-CRT signal, not yet mature.
In cT2-4aN0-2 MIBC weighing bladder preservation against radical cystectomy, this signals induction ipi+nivo plus chemoradiation is feasible even with node-positive disease, but single-arm 2yr data do not yet displace cystectomy or chemoRT alone off-protocol.
- Does induction ipi+nivo improve bladder-intact EFS vs chemoRT alone? n=50 · primary completion 2024-07 · MMC/cape chemoRT + nivo±ipi, nivo-mono comparator armn=50 · primary completion 2025-09 · induction ipi+nivo → chemoRT, cT2-4aN0-2 bladder-sparing
- Durability of bladder preservation beyond 2 years n=30 · primary completion 2027-06 · long-term bladder-preservation outcomes post-NAT TMT
- Does bladder preservation extend to node-positive (N1-2) MIBC? n=11 · primary completion 2026-02 · chemoRT ± durvalumab, node-positive bladder cancer
📚 Sources · 🐦 1 tweet
‼️ INDIBLADE: stage II/III (cT2-4aN0-2) MIBC -> induction ipilimumab plus nivolumab -> CRT
— NonsparseOncologist (@5_utr) June 17, 2026
2-year bladder-intact event-free survival is 78% (0.67−0.9) 🤩
2-year overall survival was 96% (0.91−1)
Lots of bladders can be potentially spared!https://t.co/LzTe72GYHD
DOREMY NCT02106312
ForLocalized translocation-confirmed myxoid liposarcoma, trunk/extremity
TL;DR5yr local recurrence-free survival 97.4% after de-escalated 36Gy/18fx preop RT in myxoid liposarcoma; wound complications 21%.
The RT read is dose de-escalation: 36Gy/18fx (vs the standard 50Gy/25fx) held 5yr LRFS at 97.4% in translocation-confirmed MLS, with wound complications 21% and G3 late toxicity 3%. Exploiting MLS radiosensitivity trims ~14Gy without a local-control cost, moving the preop-dose decision for this histology specifically.
7 details 4 trials watching
Phase 2 single-group nonrandomized trial, N=90, 9 tertiary sarcoma centers (Europe + US), enrolled 2010-2020. Median follow-up 66.4 mo (IQR 48.8-87.5).
Adults with biopsy-proven, translocation-confirmed localized MLS of trunk or extremity. Mean age 47, 56% male.
36 Gy in once-daily 2-Gy fractions (18 fx) preoperatively, against the standard 50 Gy/25 fx for soft-tissue sarcoma. Delivered per protocol in all 90 pts, then resection.
5yr LRFS 97.4% (95% CI 93.9-100) is the standout; PFS 81.0%, DSS 89.5%, OS 88.5% (full set in table). 3 pts (3%) progressed to metastasis before surgery.
| Endpoint (5yr) | Rate | 95% CI |
|---|---|---|
| Local recurrence-free survival | 97.4% | 93.9-100 |
| Progression-free survival | 81.0% | 72.6-89.4 |
| Disease-specific survival | 89.5% | 82.6-96.4 |
| Overall survival | 88.5% | 81.2-95.8 |
Wound complications in 18 pts (21%), 14 (16%) needing intervention. Late toxicity: G2 in 13 (15%), G3 in only 3 (3%).
Standard preoperative dose for soft-tissue sarcoma is 50 Gy/25 fx. MLS is highly radiosensitive, which motivates cutting ~14 Gy to 36 Gy while preserving local control.
Single-arm, no randomized comparator vs 50 Gy; equivalence inferred, not proven. Rare cancer makes a phase 3 impractical (authors' argument).
Single-arm nonrandomized phase 2; no randomized comparator vs standard 50Gy. Long follow-up, but efficacy equivalence is inferred, not tested. Single-arm design caps the read.
In localized, translocation-confirmed myxoid liposarcoma of the trunk or extremity, this supports reduced-dose 36Gy preop RT as an option; it does not extend to other soft-tissue sarcoma histologies that lack this radiosensitivity.
- Non-inferiority vs standard 50Gy preop RT unproven n=300 · primary completion 2031-01 · prospective MLS registry: 36Gy vs 50Gy preop RT
- Generalizability to non-myxoid soft-tissue sarcoma histologies n=15 · primary completion 2027-05 · hypofrac preop RT in mixed extremity/trunk STSn=150 · primary completion 2028-11 · 14x3Gy hypofrac preop RT across STS histologiesrecruiting Assessment of the Long-term Efficacy of Moderately Hypofractionated Neoadjuvant Radiotherapy Soft Tissue Sarcoma in the Limbs or Trunk Wall Phase 2n=135 · primary completion 2032-06 · mod-hypofrac neoadj RT, all STS grades, LC endpoint
📚 Sources · 📄 1 paper
Abstract
REVELUTION
ForIntermediate/high-risk non-metastatic prostate on definitive RT + ADT
68.9 mm³ more plaque with leuprolide vs relugolix
Adjusted for age, statin, baseline plaque; crude 56 vs 25 mm³
TL;DR68.9 mm³ greater total coronary plaque progression with leuprolide vs relugolix at 12mo (adjusted), non-metastatic prostate on RT + ADT.
Reported via UroToday →
The signal is non-calcified plaque: leuprolide added 68.9 mm³ more total plaque than relugolix at 12mo (adjusted), and that gap tracked the non-calcified subtype, with no significant difference in calcified or low-attenuation plaque. For a radonc co-prescribing ADT with definitive RT, it strengthens the mechanistic case for relugolix in cardiovascular-risk pts.
8 details 3 trials watching
Single-institution, open-label, parallel-cohort randomized trial (4 Emory-affiliated centers, Jun 2020-2024). ADT-eligible pts randomized 1:1 relugolix vs leuprolide, stratified by ASCVD 10-yr risk; a lower-risk radiotherapy-alone cohort ran in parallel as a no-ADT control. N=94.
Non-metastatic intermediate/high-risk prostate cancer, all receiving pelvic RT (± pelvic nodes). ADT arms received ≥6 months hormone therapy; the control cohort was lower-risk, RT-alone, with no planned ADT.
Relugolix 360mg load then 120mg daily vs leuprolide 3-month depot. Serial coronary CTA at baseline and 12mo, blinded to arm, quantified by the HeartFlow automated tool.
Primary: 12-month change in total plaque volume. Secondary: non-calcified, calcified, and low-attenuation plaque subtypes.
Adjusted mean total-plaque difference 68.9 mm³ favoring relugolix; crude 12-mo change 56 vs 25 mm³ (leuprolide vs relugolix). Excess driven by non-calcified plaque; calcified and low-attenuation subtypes showed no significant difference.
Offers a coronary-atherosclerosis mechanism for HERO (2020), where relugolix showed lower MACE than leuprolide despite similar testosterone suppression and metabolic effects.
Surrogate imaging endpoint (plaque volume), not clinical MACE; small single-institution N=94, 12-month follow-up. Open-label, with a non-randomized RT-alone control cohort.
Small single-institution randomized trial, surrogate coronary-plaque imaging endpoint (not clinical MACE), 12-mo f/u; mechanistically supports HERO but doesn't independently establish clinical benefit.
In an intermediate or high-risk non-metastatic prostate pt getting definitive RT plus ADT with elevated cardiovascular risk, this supports favoring relugolix over leuprolide on a coronary-plaque basis; it does not extend to ADT-free lower-risk pts or to hard cardiovascular-event rates.
- Do plaque-volume differences translate to fewer clinical cardiovascular events? recruiting Effects of Relugolix vs Leuprolide on Cardiac Function in Patients With Prostate Cancer Phase 2n=70 · primary completion 2027-12 · phase 2 relugolix vs leuprolide cardiac function MRIrecruiting REVELUTION-2: Relugolix+Abiraterone Acetate (AA) Versus Leuprolide+AA Cardiac Trial Phase 3n=72 · primary completion 2029-07 · phase 3 relugolix vs leuprolide cardiac head-to-head
- Durability of plaque effect beyond 12 months recruiting REVELUTION-2: Relugolix+Abiraterone Acetate (AA) Versus Leuprolide+AA Cardiac Trial Phase 3n=72 · primary completion 2029-07 · up to 24-mo combination arm, cardiac readout to 2029
- Generalizability beyond single-institution N=94
📚 Sources · 📄 1 paper
Abstract
ORIOLE NCT02680587
ForRecurrent HSPC, 1-3 conventional-imaging mets, off ADT ≥6mo
19% vs 61%
P=.005; SABR vs observation
TL;DR6-mo progression 19% vs 61% favoring SABR (P=.005); mPFS NR vs 5.8mo, HR 0.30 (0.11-0.81) in oligomet HSPC.
Surfaced from a review's discussed trials
The RT read is completeness, not SABR alone: among SABR pts, leaving any PSMA-avid lesion untreated collapsed DMFS to 6.0 vs 29.0 mo (HR 0.19, 0.07-0.54). Conventional imaging under-stages, so PSMA-PET staging plus total consolidation, not partial MDT, is the decision this moves. SABR dose/fractionation not reported in source.
9 details 5 trials watching
Phase 2 randomized trial, 2:1 SABR vs observation, N=54 at 3 US radiation centers. Primary: composite progression at 6 mo. Median follow-up 18.8 mo.
Recurrent hormone-sensitive prostate cancer, 1-3 asymptomatic mets ≤5 cm on conventional imaging, prior definitive treatment of the primary. No ADT within 6 mo. Median age 68.
SABR to all conventional-imaging metastases; PSMA-PET obtained but blinded to planning. Dose/fractionation not reported in source. Local control 98.9% at 6 mo.
Because PET was blinded, 16/36 SABR pts had untreated PET-avid lesions; any untreated lesion collapsed DMFS to 6.0 vs 29.0 mo (HR 0.19). Total consolidation, not SABR per se, drove the benefit.
Concordant with STOMP (phase 2 MDT in oligomet PC): both show metastasis-directed therapy delays progression and defers ADT. The pooled ORIOLE+STOMP analysis reinforced the signal.
Phase 2, N=54; composite surrogate primary read at 6 mo, not OS-powered. Open-label observation control. Conventional-imaging staging misses PET-avid disease.
| Endpoint | SABR | Observation | Effect |
|---|---|---|---|
| 6-mo progression (composite) | 7/36 (19%) | 11/18 (61%) | P=.005 |
| 6-mo PSA progression | 4/36 (11%) | 9/18 (50%) | P=.005 |
| Median PFS | Not reached | 5.8 mo | HR 0.30 (0.11-0.81), P=.002 |
| Median biochemical PFS | Not reached | 6.4 mo | HR 0.31 (0.13-0.75), P=.002 |
| Endpoint | No untreated | Any untreated | Effect |
|---|---|---|---|
| 6-mo progression | 1/19 (5%) | 6/16 (38%) | P=.03 |
| Median PFS | Not reached | 11.8 mo | HR 0.26 (0.09-0.76), P=.006 |
| New mets 180d | 3/19 (15.8%) | 10/16 (62.5%) | P=.006 |
| DMFS | 29.0 mo | 6.0 mo | HR 0.19 (0.07-0.54), P<.001 |
Phase 2, N=54; composite progression primary read at only 6mo. Randomised but small, short f/u. Concordant with STOMP MDT signal; awaits phase 3.
In recurrent HSPC with 1-3 conventional-imaging mets and off ADT ≥6mo, this supports metastasis-directed SABR to defer systemic therapy; it does not extend to higher-volume or castration-resistant disease.
- Overall survival benefit of metastasis-directed SABR recruiting Stereotactic Ablative Radiotherapy (SABR) for the Treatment of Patients With Metastatic Cancer, ID-COMET Trial Phase 3n=800 · primary completion 2032-09 · phase 3 SABR vs 3-mo delay, survival endpoint
- Role of PSMA-PET staging before consolidative SABR n=140 · primary completion 2025-05 · PSMA vs fluciclovine PET for RT planningactive Multicenter Randomized Trial of 68Ga-PSMA-11 PET/CT Based SRT After Radical Prostatectomy Phase 3n=193 · primary completion 2027-07 · randomized 68Ga-PSMA PET-guided RT vs standard
- SABR benefit in higher-volume or ADT-dependent disease active Androgen Deprivation Therapy for Oligo-recurrent Prostate Cancer in Addition to radioTherapy Phase 3n=280 · primary completion 2027-10 · phase 3 MDRT ± ADT vs MDRT alone, MPFSrecruiting HIghly MetAstatic Life Prolonging Therapy-Resistant Prostate Cancer: Role of Stereotactic Radiotherapy for Bone and Lymph Node Metastases (HIMARS) Phase NAn=18 · primary completion 2028-05 · SBRT volume-escalation in high-volume mets
📚 Sources · 📄 1 paper
Abstract
RAPCHEM
ForSmall (<5cm) cN1 breast, post-neoadjuvant chemo + surgery, mostly ALND
TL;DR10-yr locoregional recurrence 2.9% (24/838) with radiotherapy de-escalated by nodal response to neoadjuvant chemo; no comparator arm.
Reported via The ASCO Post →
The RT read is the intermediate arm: pts with 1-3 residual nodes got breast RT with regional nodal RT omitted, yet 10-yr LRR held at 3.2%. With low-risk mastectomy pts left with no RT (2.4%), this is the uncontrolled signal behind omitting nodal RT after partial nodal response to NAC, the question B-51 will settle.
7 details 3 trials watching
Prospective, non-randomized multicentre cohort (BOOG 2010-03), 17 Dutch centres, enrolled 2011-2015. Single arm, no with-vs-without RT comparator. 10-year follow-up.
Small (<5 cm) breast cancer with 1-3 clinically involved nodes, treated with neoadjuvant chemotherapy then surgery. Most underwent axillary lymph node dissection. N=848 (838 with follow-up).
RT allocated by post-chemo nodal status. Low (node-negative): breast RT after BCS, RT omitted after mastectomy. Intermediate (1-3 residual nodes): breast/chest wall, regional nodal RT omitted. High (≥4 nodes): breast/chest wall plus nodal RT. Dose/fractionation not reported in source.
Locoregional recurrence (breast, chest wall, or nodal, without distant disease) at 10 years. No formal primary-endpoint statistic reported in source.
Overall 10-yr LRR 2.9% (24/838). Rates stayed low across all three tailored groups, including the de-escalated arms (see table).
| Risk group | RT approach | 10-yr LRR |
|---|---|---|
| Low (node-negative after chemo) | Breast RT after BCS; RT omitted after mastectomy | 2.4% (7/291) |
| Intermediate (few residual nodes) | Breast/chest wall, regional nodes not treated | 3.2% (12/370) |
| High (many residual nodes) | Breast/chest wall + regional nodal RT | 2.8% (5/177) |
Consistent with the de-escalation direction of trials testing nodal RT after NAC, but the randomized answer is **NSABP B-51/RTOG 1304 (NCT01872975)**, testing nodal RT in pts converting to ypN0, expected ~3 years.
Single-arm and uncontrolled: cannot show tailored RT is non-inferior to standard fields. ALND-era staging limits transfer to current SLNB practice. Dose/fractionation and per-group RT compliance not reported in source.
Single-arm, uncontrolled cohort with no with-vs-without RT comparator; cannot show tailored de-escalation is safe. Randomized answer (NSABP B-51) still pending.
In cN1 breast cancer with 1-3 residual nodes after neoadjuvant chemo, this uncontrolled 10-yr data supports reduced-field RT with regional nodes left untreated; it does not extend to pts with ≥4 residual nodes, who still received nodal RT.
- RNI omission after ypN1 vs standard nodal fields, non-inferior? recruiting Internal Mammary Lymph Nodes Irradiation in High-risk Breast Cancer After Neoadjuvant Chemotherapy Phase 3n=722 · primary completion 2032-07 · IMN irradiation vs omission in ypN+ post-NAC
- Post-mastectomy RT omission after nodal conversion to ypN0 active Standard or Comprehensive Radiation Therapy in Treating Patients With Early-Stage Breast Cancer Previously Treated With Chemotherapy and Surgery Phase NAn=1636 · primary completion 2023-09 · comprehensive nodal + chest wall RT vs standard
- Does risk-tailored RT transfer to an SLNB-staged axilla? recruiting Axillary Management in Breast Cancer Patients With Needle Biopsy Proven Nodal Metastases After Neoadjuvant Chemotherapy Phase NAn=1900 · primary completion 2030-02 · omit axillary RT if SLN ypN0 after NACT
📚 Sources · 📄 1 paper
Abstract
COMPPARE
ForDe novo localized prostate cancer, excl very-high-risk and metastatic
TL;DRProton vs IMRT: no difference in bowel urgency (6% vs 5.7%), ≥G2 GI tox, or 3-yr biochemical control in localized prostate.
The RT read is that rectal spacer use, not proton vs photon, moved GI toxicity: 2-yr G2+ fell to ~4.4-4.7% with a spacer vs 7.2-8.7% without (p=0.009), similar across modalities. Protons showed no toxicity or 3-yr biochemical-control edge, arguing against the proton premium for localized disease.

| Endpoint | IMRT | Proton | P |
|---|---|---|---|
| Bowel urgency (EPIC) | 6% | 5.7% | 0.28 |
| Bowel frequency (EPIC) | 4% | 3.5% | 0.43 |
| GI tox ≥G2 (CTCAE) | 5.6% | 5.2% | 0.60 |
| 3-yr FFDP (PSA) | 97.9% | 98.0% | 0.90 |
+1 more figure

| Group | 2-yr G2+ GI toxicity (95% CI) |
|---|---|
| IMRT, no spacer | 7.2% (5.0%, 9.9%) |
| Proton, no spacer | 8.7% (5.0%, 14%) |
| IMRT, spacer | 4.4% (2.8%, 6.4%) |
| Proton, spacer | 4.7% (3.6%, 6.0%) |
6 details 5 trials watching
Prospective comparative effectiveness study (COMPPARE, PCORI-funded), non-randomized proton vs photon cohorts across 51 centers. 2524 accrued July 2018-October 2022. Early results, short follow-up.
De novo localized prostate cancer, excluding very-high-risk and metastatic. Proton cohort n=1500, photon (IMRT) cohort n=1000.
Proton therapy vs IMRT; rectal spacer use captured as a covariate (FDA-approved 2015). Dose/fractionation and target volume not reported in source.
Co-primary patient-reported bowel urgency and frequency (EPIC) and ≥G2 GI toxicity (CTCAE v5), each powered 90%. Exploratory: 3-yr freedom from PSA progression.
No significant proton advantage on any endpoint (all p ≥ 0.28). Observed toxicity fell far below design assumptions (hypothesized IMRT GI tox 29%, actual 5.6%).
Rectal spacer reduced 2-yr cumulative G2+ GI toxicity in both arms (p=0.009); the spacer effect exceeded any proton-vs-IMRT difference.
Directionally consistent with PARTIQoL (randomized proton vs IMRT, localized prostate), which found no bowel-QoL advantage for protons.
Non-randomized cohorts (selection bias, residual confounding); short follow-up leaves late GU/GI toxicity and long-term control unanswered; dose/fractionation not reported.
Prospective but non-randomized cohorts (selection bias); early results, short f/u leave late toxicity and long-term control open. Null aligns with randomized PARTIQoL non-superiority.
In localized prostate cancer (de novo, excluding very-high-risk and metastatic), these early data question routine proton use over IMRT for GI toxicity or 3-yr control; they do not yet speak to late toxicity or long-term outcomes.
- Late GU/GI toxicity beyond 3 years n=454 · primary completion 2025-12 · proton vs IMRT, side-effect head-to-headactive A Prospective Comparative Study of Outcomes With Proton and Photon Radiation in Prostate Cancer Phase NAn=3000 · primary completion 2026-02 · 3000-pt proton vs IMRT QOL + toxicity cohortn=400 · primary completion 2027-03 · proton vs photon, primary late GI toxicity
- Long-term biochemical and metastasis-free control with protons vs IMRT active A Prospective Comparative Study of Outcomes With Proton and Photon Radiation in Prostate Cancer Phase NAn=3000 · primary completion 2026-02 · proton vs IMRT cohorts, disease-control endpointn=303 · primary completion 2026-12 · proton vs IMRT hypofx, improve cancer control
📚 Sources · 🐦 1 tweet
#COMPPARE early results: in localized #ProstateCancer, #proton therapy vs #IMRT showed no sig difference in pt-reported bowel urgency/frequency, ≥G2 GI toxicity, or 3-year biochemical control. Longer follow-up needed for late toxicity/long term outcomes #ASCO2026 pic.twitter.com/yli4l8nEOY
— QianJanieQin (@QianJanieQin) May 31, 2026
MIRACLE-2
For1L unresectable MSS rectal cancer, synchronous liver/lung mets
TL;DR68% ORR, mOS 23.2mo, 18% NED with RT-primed chemo + tislelizumab in MSS unresectable met rectal ca.
The RT-relevant read is technique: HFRT to the primary plus HFRT/SBRT to mets, delivered first to prime immunity, but no dose or fractionation in source, so it doesn't transfer to practice yet. 18% (9/50) converted to NED via resection or watch-and-wait. Near-universal lymphopenia (95.9% all-grade, 36.7% G3/4) undercuts a strategy premised on RT-driven T-cell activation.

| Metric | n (%) | 95% CI |
|---|---|---|
| CR | 1 (2.0%) | |
| PR | 33 (66.0%) | |
| SD | 10 (20.0%) | |
| PD | 6 (12.0%) | |
| ORR | 34 (68.0%) | 53.6-80.0% |
| DCR | 44 (88.0%) | 76.0-95.2% |
| ETS | 38 (76.0%) | 62.4-86.8% |
9 details 2 trials watching
Prospective single-arm phase I, N=50, Fudan University Shanghai Cancer Center. Data cutoff Dec 31 2025; median follow-up 19.9 mo (95% CI 16.4-23.4).
MSS rectal cancer, primary ≤10cm from anal verge, synchronous unresectable mets. 76% male, median age 57; 52% liver, 8% lung, 40% both; RAS/BRAF-mut 56%.
RT delivered first as an immune primer: HFRT to the primary, HFRT or SBRT to metastases. Dose, fractionation, and target volumes not reported in source.
Post-RT, biomarker-gated: FOLFOX-bevacizumab-tislelizumab (RAS/BRAF-mut) or FOLFIRI-cetuximab-tislelizumab (WT); tislelizumab 200mg Q2W. Resection/metastasectomy if converted, watch-and-wait if primary cCR.
Primary: ETS rate (≥20% target shrinkage at 8wk). Secondary: DCR, DOR, OS, PFS, safety.
ETS 76.0%, ORR 68.0%, DCR 88.0%; 18% (9/50) reached NED. Median OS 23.2mo, PFS 9.3mo, DOR 8.0mo (endpoints in table).
| Endpoint | Median | 95% CI | 1-yr rate |
|---|---|---|---|
| OS | 23.2 mo | 15.1-31.3 | 93.3% |
| PFS | 9.3 mo | 7.1-11.5 | 33.4% |
| DOR (n=34) | 8.0 mo | 5.2-10.8 | 20% |
Single-arm phase I, N=50, no comparator to isolate RT's contribution. Surrogate primary (ETS at 8wk), short median DOR (8mo), and near-universal lymphopenia (95.9%).
Single-arm phase I, N=50; surrogate primary (ETS at 8wk); no comparator to isolate RT's contribution to the immune-priming effect.
- RT's added benefit over chemo plus PD1 alone in MSS mCRC
- Optimal RT dose and fractionation for immune priming in MSS mCRC recruiting Regorafenib Alone or in Combination With Hypofractionated/Low-dose Radiotherapy Plus Toripalimab for Metastatic Colorectal Cancer Phase 2n=108 · primary completion 2025-04 · randomized hypofrac+LDRT + toripalimab, MSS mCRCrecruiting Standard Systemic Therapy Combined With High/Low-dose Radiotherapy Plus Toripalimab for Metastatic Colorectal Cancer Phase 2n=96 · primary completion 2026-12 · high + low-dose RT + toripalimab in MSS mCRC
- Predictive biomarker for MSS response to trimodal therapy
📚 Sources · 🐦 1 tweet
MIRACLE-2: RT to primary/mets -> chemo + tislelizumab in MSS unresectable met rectal ca (N=50): 68% ORR & median OS 23 mo.
— Dr. Nina Niu Sanford (@NiuSanford) May 31, 2026
Early, single-arm data, but ~1 in 5 pts reached NED.
Suggests RT + systemic + PD1 blockade could overcome immune resistance in MSS mCRC. #ASCO26 @OncoAlert pic.twitter.com/sjnUW8x7f3
RAD-IO
ForT2-T4a N0M0 muscle-invasive urothelial bladder cancer
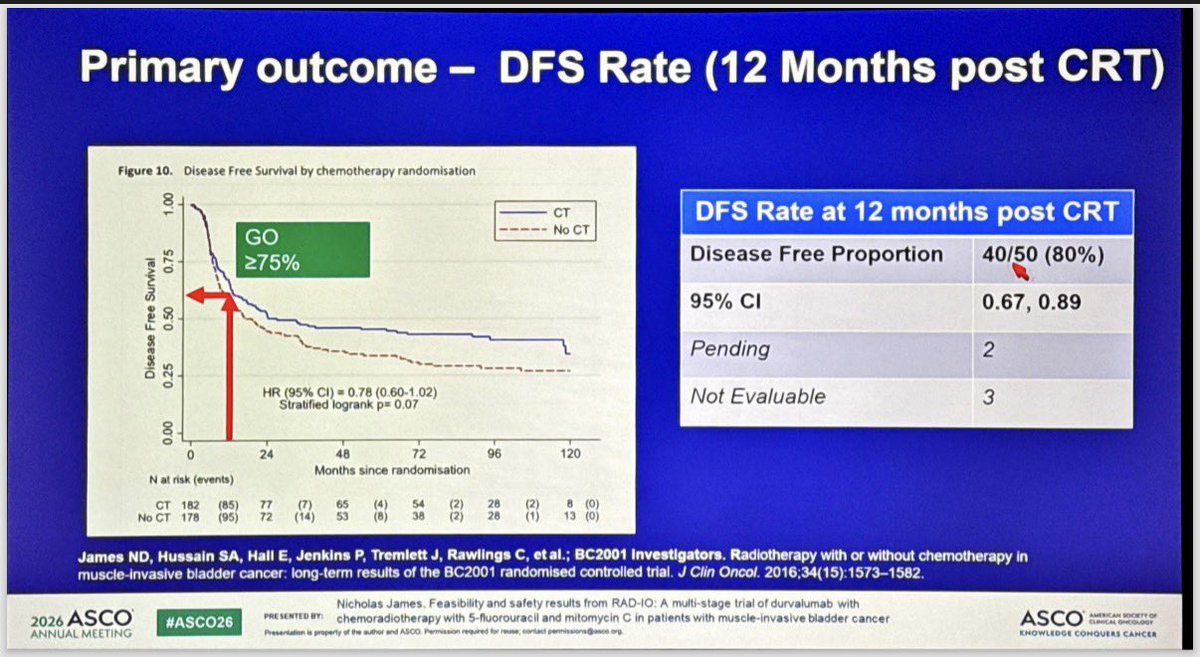
TL;DR12-mo DFS 40/50 (80%, 95% CI 0.67-0.89) cleared the pre-set ≥75% GO bar for durvalumab added to 5FU/MMC chemoRT in MIBC.
RT is standard and transferable: 55Gy/20fx to bladder, plus 46Gy/20fx elective nodal coverage in the node-positive expansion, extending durvalumab-chemoRT preservation to N+ disease. 12-mo DFS 80% (40/50, 95% CI 0.67-0.89) cleared the pre-set ≥75% GO bar vs BC2001. Moves whether to layer IO onto a hypofractionated preservation backbone.
+1 more figure

8 details 4 trials watching
Single-arm, multi-stage feasibility and safety trial testing durvalumab added to 5FU/MMC chemoradiation for bladder preservation. Benchmarked against BC2001 historical CRT data, not a randomised comparator.
T2-T4a N0M0 urothelial muscle-invasive bladder cancer, stratified by prior neoadjuvant chemotherapy (yes vs no). A stage-1 expansion added the first 6 node-positive pts.
Durvalumab 1500 mg given neoadjuvant, synchronous, and adjuvant to 12 months post-chemoRT. Concurrent 5-FU 500 mg/m²/24h ×5 days and mitomycin C 12 mg/m².
55 Gy in 20 fractions to bladder (hypofractionated). Node-positive expansion added 46 Gy/20 fx elective nodal RT.
Primary: 12-month disease-free survival post-chemoRT, read against a GO/NO-GO framework (GO ≥75%, contextual 60-75%, NO-GO <60%).
12-mo DFS 40/50 (80%), 95% CI 0.67-0.89, clearing the ≥75% GO bar. 33/54 (61%) completed planned durvalumab; investigators reported very high bladder-preservation and DFS vs prior trial data.
AEs reported in line with component therapies (chemoRT plus durvalumab). 21/54 (39%) discontinued durvalumab early.
Benchmarked against BC2001 (James, JCO 2016), where adding 5FU/MMC to RT gave DFS HR 0.78 (0.60-1.02), p=0.07. RAD-IO's 80% 12-mo DFS is claimed higher than prior data, but the comparison is non-randomised.
Single-arm with a historical benchmark and no concurrent IO comparator; 12-mo DFS is an early surrogate; small N (~50 evaluable); node-positive experience limited to 6 pts.
Single-arm feasibility stage, no randomised IO comparator; benchmarked against historical BC2001. 12-mo DFS an early surrogate at small N; met pre-set GO bar for further evaluation only.
In T2-T4a N0M0 MIBC opting for bladder preservation, this supports durvalumab layered onto 5FU/MMC chemoRT as worth further evaluation; it does not yet establish that IO improves on chemoRT alone, and node-positive experience rests on only 6 expansion pts.
- Does durvalumab add over chemoRT alone in a randomised trial n=11 · primary completion 2026-02 · randomised chemoRT ± durvalumab in node+ MIBC
- Durability of bladder preservation and DFS beyond 12 months active Treating Muscle-invasive Bladder Cancer With A Non-surgical Method Consisting of Anti-PD-1 Therapy and Chemoradiation Phase 2n=71 · primary completion 2025-12 · IO+chemoRT bladder preservation, phase 2recruiting Enfortumab Vedotin in Combination With Pembrolizumab vs. Concurrent Chemoradiotherapy (cCRT) in People With Muscle Invasive Bladder Cancer (EV-309) Phase 3n=390 · primary completion 2030-03 · phase 3 EV+pembro vs cCRT bladder preservation
- Efficacy in node-positive MIBC beyond the 6-patient expansion n=11 · primary completion 2026-02 · durvalumab+chemoRT in node-positive bladder ca
📚 Sources · 🐦 3 tweets
RAD-IO: chemoradiation (5FU+MMC) + Durva in MIBC. #ASCO26 pic.twitter.com/yTyhkdjCox
— Álvaro Pinto (@dralvaropinto) May 30, 2026
#ASCO26 🔬 Abstract 4504 | RAD-IO
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
Durvalumab + chemoradiotherapy in muscle-invasive bladder cancer
Presented by Nicholas D. James, PhD, MBBS, FRCP@OncoAlert@ASCO
Bladder preservation in MIBC remains one of the most important curative-intent questions in GU oncology.
The key… pic.twitter.com/W6JqzTVsJ3
RAD-IO at #ASCO26: durvalumab added to chemoradiation in muscle-invasive bladder cancer cleared its efficacy bar in a bladder-preservation approach. Single-arm, benchmarked against prior CRT data.
— Katy Beckermann (@katy_beckermann) May 30, 2026
Durvalumab given before, during, and 12 months after chemoRT (55Gy/20Fr +… pic.twitter.com/UXxwoZzaMC
A-DREAM
FormHSPC deep responder (PSA<0.2) after 18-24mo ADT + ≥12mo ARPI
TL;DR41% remained treatment-free with eugonadal testosterone recovery at 18mo after interrupting ADT+ARPI in deep-responding mHSPC (1° EP met, one-sided p=0.0249).
In metastatic HSPC deep responders (PSA<0.2 after ≥18mo ADT and ≥12mo ARPI, predominantly low-volume), this supports discussing a monitored ADT+ARPI holiday with scheduled PSA/imaging; it does not extend to incomplete responders or high-volume disease.

+2 more figures


8 details 4 trials watching
Phase 2 single-arm Alliance trial. N=78 eligible metastatic HSPC deep responders interrupt ADT+ARPI. Enrolled 07/2022-03/2024; median follow-up 26.9mo.
Entry required PSA<0.2 (stable/falling) after 18-24mo ADT and ≥12mo ARPI. Median age 70 (49-90); 64.9% low-volume, 35.1% high-volume (CHAARTED); 51.3% had prior local radiation, 29.5% metastasis-directed radiation.
Primary: treatment-free with eugonadal testosterone (≥150 ng/dL) at 18 months. Exploratory: rPFS, TTNT, OS, cost.
Primary met: 32/78 (41.0%) treatment-free and eugonadal at 18mo (80% CI 33.1-48.9%, one-sided p=0.0249). 57.7% were treatment-free at 18mo and 66.7% recovered testosterone; median time to eugonadal T 9.0mo.
Disease control held through interruption: rPFS 15/78 events, OS 4/78 events, both medians not reached. The 41% primary is capped by slow testosterone recovery, not progression, so the endpoint understates short-term oncologic safety in this older cohort.
Single-arm with no randomised comparator against continued therapy, so the survival cost of interruption is unquantified. Median follow-up 26.9mo is short for mHSPC; durability of treatment-free intervals is unproven.
Single-arm phase 2, N=78, no randomised comparator vs continued therapy; primary endpoint met but interruption safety needs longer follow-up and randomisation.
- Survival cost of interruption vs continued ADT+ARPI active A Study of an Intermittent ADT Approach With Apalutamide Monotherapy in Participants With mCSPC Phase 3n=420 · primary completion 2026-10 · intermittent post-response, rPFS non-inferiorityn=1600 · primary completion 2035-05 · phase 3 intermittent vs continuous, OS endpoint
- Durability of treatment-free interval beyond 27 months
- Which deep responders can safely interrupt active A Study of an Intermittent ADT Approach With Apalutamide Monotherapy in Participants With mCSPC Phase 3n=420 · primary completion 2026-10 · restricted to PSA <0.2 deep respondersrecruiting Optimal PSA Triggered Individual Management of Androgen Sensitive Prostate Cancer Phase 2n=160 · primary completion 2030-10 · intermittent ARPI in optimal PSA responders
📚 Sources · 🐦 1 tweet
Can treatment be safely stopped in selected patients with mHSPC?
— MJosé Juan (@mjuanfi81) May 30, 2026
Phase II A-DREAM trial, 41% of responders remained treatment-free with testosterone recovery 18m after stopping ADT/ARPI. At a median FU of 21 months, 35% of patients required treatment re-initiation.@OncoAlert pic.twitter.com/iW2VDBWWhN
CHRYSALIS-2
ForTreatment-naïve atypical EGFR-mutant advanced NSCLC
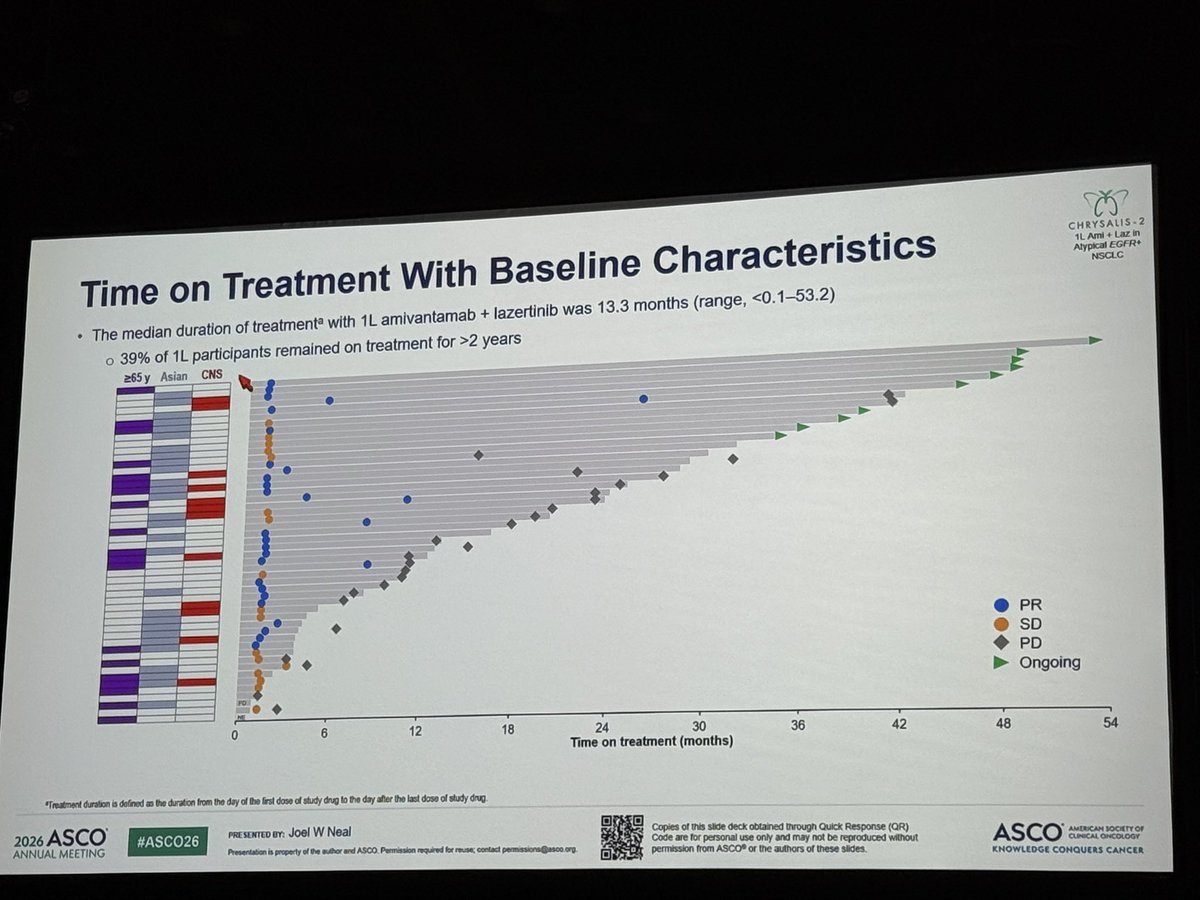
TL;DRmOS 41.0 mo (95% CI 27.7-NE) with 1L amivantamab + lazertinib in treatment-naïve atypical EGFR-mutant NSCLC; single-arm, n=49.
In treatment-naïve atypical EGFR-mutant advanced NSCLC, a population with few standard targeted options, this single-arm 41-mo median OS supports amivantamab+lazertinib as a candidate 1L regimen; it does not extend to common EGFR (exon19del/L858R) disease, where randomised data already guide practice.

+1 more figure
8 details
Single-arm cohort, n=49, no randomised comparator. Median follow-up 31.3 mo.
Treatment-naïve (1L) atypical EGFR-mutated advanced NSCLC. Responses durable regardless of demographics, baseline mutations, and disease characteristics.
IV amivantamab + lazertinib. Median treatment duration 13.3 mo (range <0.1-53.2); 39% on treatment >2 years.
Median OS 41.0 mo (95% CI 27.7-NE), ~3.5 years. No clear association between EGFR variant subtype and OS.
With longer follow-up, safety consistent with prior reports; no new safety signals.
Extends the durable 1L amivantamab+lazertinib OS signal from common EGFR (exon19del/L858R) to atypical variants.
Single-arm, n=49, no randomised comparator. Atypical EGFR is a heterogeneous class; per-variant efficacy not detailed in source.
Single-arm cohort (n=49), no randomised comparator in atypical EGFR NSCLC; durable but single-arm design caps the read at early-signal despite 31-mo follow-up.
- Efficacy by specific atypical EGFR variant
- Randomised comparison vs other 1L options in atypical EGFR
📚 Sources · 🐦 1 tweet
Amivantamab + lazertinib achieved a median OS of 41.0 months in treatment-naïve atypical EGFR-mutant NSCLC, with no clear association between EGFR variant subtype and outcome. A compelling option. Meanwhile, amivantamab continues evaluation across multiple tumor types. #ASCO26 pic.twitter.com/aWn3Ja60Ji
— Chul Kim (@chulkimMD) May 29, 2026
ESAONA
ForTreatment-naive EGFR-mutant NSCLC with brain metastases
TL;DRiORR 95.5% vs 79.6% (p=0.0004) and icPFS HR 0.46 favoring asandeutertinib over osimertinib in 1L EGFR-mut NSCLC brain mets.
The RT-relevant read is upfront local therapy: iORR 95.5% vs 79.6% and intracranial PFS not reached (HR 0.46) strengthen deferring upfront SRS/WBRT in favor of TKI in EGFR-mut brain mets. No head-to-head vs radiosurgery, so it moves sequencing, not RT omission at progression.
7 details 5 trials watching
Randomised phase 2, N=224 (111 asandeutertinib vs 113 osimertinib), 1L EGFR-mutant NSCLC with brain metastases. All efficacy endpoints BICR-assessed. Blinding not specified in source.
Treatment-naive (1L) EGFR-mutant NSCLC with brain metastases. Mutation subtype, symptomatic status, and prior brain RT not reported in source.
Asandeutertinib (next-generation EGFR TKI) vs osimertinib. Dose and schedule not reported in source.
Intracranial endpoints (response, icPFS) drove the result and cleared significance more decisively than the borderline overall PFS benefit. Full arm comparison in the table above.
| Endpoint | Asandeutertinib | Osimertinib | HR (p) |
|---|---|---|---|
| iORR | 95.5% (89.8-98.5) | 79.6% (71.0-86.6) | p=0.0004 |
| Intracranial PFS | NR | 17.5 mo (15.18-NA) | HR 0.46, p=0.0020 |
| Overall PFS | NR | 17.2 mo (15.18-19.55) | HR 0.64, p=0.0473 |
Any TRAEs 99.1% vs 95.6%; serious TRAEs numerically higher with asandeutertinib (10.8% vs 7.1%). Fatal and discontinuation rates not reported in source.
Osimertinib is the established CNS-active 1L EGFR TKI (FLAURA). Asandeutertinib raises the intracranial bar in phase 2, but no OS or phase 3 head-to-head yet.
Phase 2 with immature time-to-event data (medians not reached); overall PFS benefit borderline (p=0.0473); no OS; blinding not specified.
Strong intracranial activity revives whether a CNS-active TKI can defer upfront brain-directed RT/SRS in EGFR-mutant NSCLC. Phase 3 confirmation vs osimertinib, plus OS and durability, is needed before displacing the standard.
Randomised phase 2; strong intracranial ORR but time-to-event immature (medians NR), overall PFS borderline (p=0.0473), no OS. Needs phase 3 before displacing osimertinib.
In treatment-naive EGFR-mutant NSCLC with brain metastases, this supports a TKI-first, SRS-deferred read; it does not extend to EGFR-wildtype disease or brain mets progressing on a prior EGFR TKI.
- Overall survival vs osimertinib recruiting TY-9591 in the Patients With EGFR Mutations in Advanced NSCLC With Brain Metastases Phase 2n=420 · primary completion 2025-06 · 1L TY-9591 vs osimertinib, EGFR brain metsn=380 · primary completion 2029-03 · phase 3 furmonertinib vs osimertinib in brain mets
- Durability of intracranial response with longer follow-up
- Head-to-head efficacy vs upfront radiosurgery n=162 · primary completion 2024-12 · osimertinib +/- early SRS, asymptomatic BMactive Study of Osimertinib + SRS vs Osimertinib Alone for Brain Metastases in EGFR Positive Patients With NSCLC Phase 2n=40 · primary completion 2025-04 · randomized osimertinib +/- upfront SRS, 1Lrecruiting Observation or Upfront Cranial RT in Oncogene Mutated NSCLC With Asymptomatic BM: A Phase III RCT Phase 3n=190 · primary completion 2025-12 · phase 3 upfront cranial RT vs obs on TKI
📚 Sources · 🐦 1 tweet
#ASCO26 🧠🌍
— Dr Rishabh Jain (@DrRishabhOnco) May 30, 2026
Could a next-generation EGFR TKI outperform osimertinib in patients with brain metastases?
The phase II ESAONA trial suggests the answer may be yes.
🧪 LBA2007 | ESAONA
1L EGFR-mutated NSCLC with brain metastases
👥 n=224
⚔️ Asandeutertinib vs Osimertinib
Key… https://t.co/mEOKGNKgf7 pic.twitter.com/pUQuH6i2cV
OptiTROP-Lung05 NCT06448312
For1L IIIB/IIIC-IV PD-L1≥1% NSCLC, EGFR/ALK wild-type
HR 0.35
95% CI 0.26-0.47, p<0.0001; median NR vs 5.7 mo
TL;DRmPFS NR vs 5.7 mo, HR 0.35, adding Sac-TMT (TROP2 ADC) to pembrolizumab in 1L PD-L1+ NSCLC.

| Arm | PFS events n (%) | Median PFS | HR (95% CI) |
|---|---|---|---|
| Sac-TMT+Pembro | 66 (31.7%) | NR (13.6-NE) | 0.35 (0.26-0.47) |
| Pembro | 128 (62.4%) | 5.7 mo (4.3-7.0) | — |
+2 more figures

| PD-L1 TPS | mPFS combo | mPFS pembro | HR (95% CI) |
|---|---|---|---|
| ≥50% | NR | 9.5 mo | 0.47 (0.29-0.77) |
| 1-49% | NR | 4.3 mo | 0.28 (0.19-0.41) |

| Arm | OS events n (%) | Median OS | HR (95% CI) |
|---|---|---|---|
| Sac-TMT+Pembro | 33 (15.9%) | NR | 0.55 (0.36-0.85) |
| Pembro | 54 (26.3%) | NR | — |
8 details 2 trials watching
Phase 3, open-label, multicenter RCT (NCT06448312); 1:1, N=413. Primary PFS by BICR crossed its interim efficacy boundary at 194 events; median follow-up 10.5 mo.
1L stage IIIB/IIIC or IV NSCLC, PD-L1 TPS ≥1% (22C3), EGFR/ALK wild-type, ECOG 0-1. Stratified by histology, PD-L1 (1-49 vs ≥50), ECOG.
Sac-TMT (TROP2 ADC) 4 mg/kg Q2W + pembrolizumab 400 mg Q6W vs pembrolizumab alone; pembro capped at 18 cycles.
ORR 70.2% vs 42.0%. PFS gain held across PD-L1 strata, strongest in TPS 1-49% where pembro monotherapy is weakest. OS immature, formal testing pending.
Current 1L PD-L1+ NSCLC standard is pembrolizumab ± chemotherapy. This tests a chemo-free ADC+IO doublet; no head-to-head vs chemo-IO.
Open-label; OS immature at 10.5-mo follow-up and formally untested; PFS reported at an interim efficacy boundary. No safety data in source.
PFS crossed an interim efficacy boundary; key-secondary OS descriptive/immature at 10.5-mo f/u; open-label. Strong but not yet mature enough to move 1L SOC.
- Will the OS benefit mature and hold? n=30 · primary completion 2026-06 · candidate match
- How does the chemo-free ADC+IO doublet compare to chemo+IO? n=30 · primary completion 2026-06 · candidate match
- Safety of adding a TROP2 ADC to pembrolizumab
📚 Sources · 🐦 2 tweets
🔁REVIEW #ASCO26 #LCSM Oral
— Hidehito HORINOUCHI (@HHorinouchi) May 30, 2026
🔥OptiTROP-Lung05: 1L Sac-TMT + Pembro vs Pembro in PD-L1+ NSCLC
✅mPFS NR vs 5.7m (HR 0.35)
✅ORR 70.2% vs 42.0%
✅OS HR 0.55 (95%CI 0.36-0.85, immature)
🎙️Dr. Caicun Zhou
🔗 https://t.co/DcbK1dGrhO@OncoAlert @Larvol @ASCO @IASLC https://t.co/512k6dZviW pic.twitter.com/Vdo86N50h9
Right patient. Right treatment. Right timing.
— Yakup Ergün (@dr_yakupergun) May 30, 2026
The result: curves like these👇#ASCO26 https://t.co/72KByLKz90
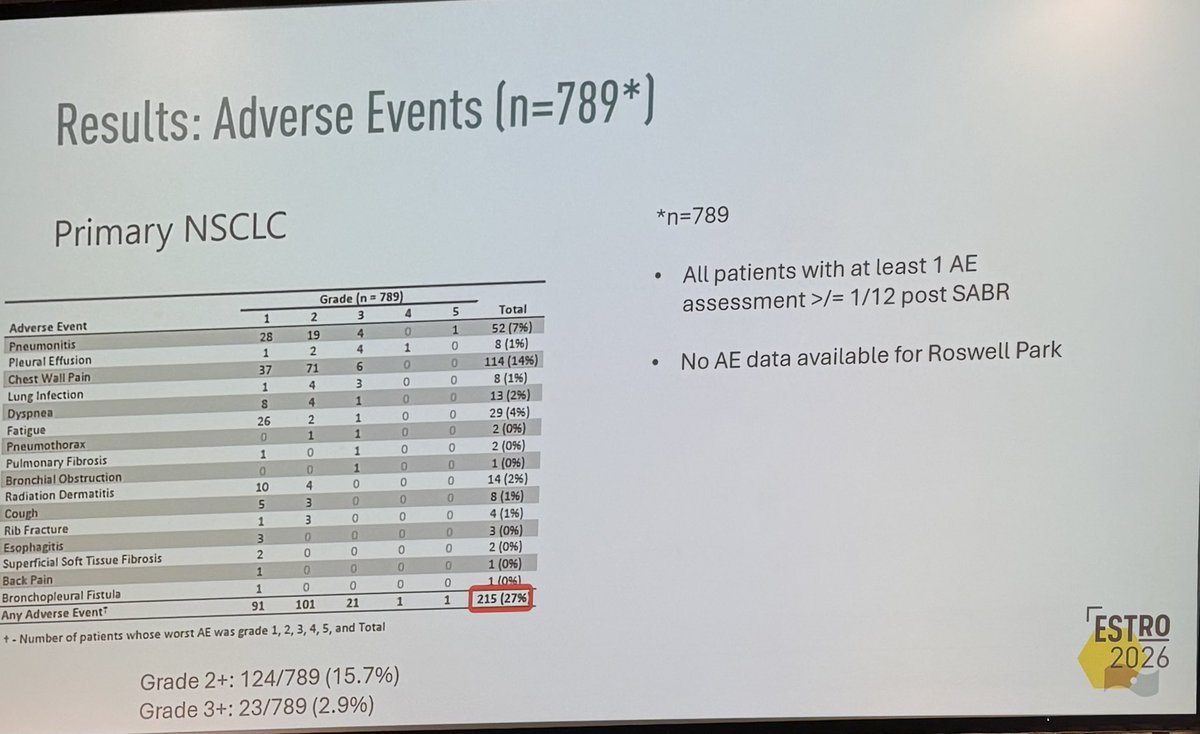
Single-fraction SABR for primary NSCLC and lung oligomets (pooled, n=1687)
ForPrimary NSCLC or pulmonary oligometastases, SABR candidates
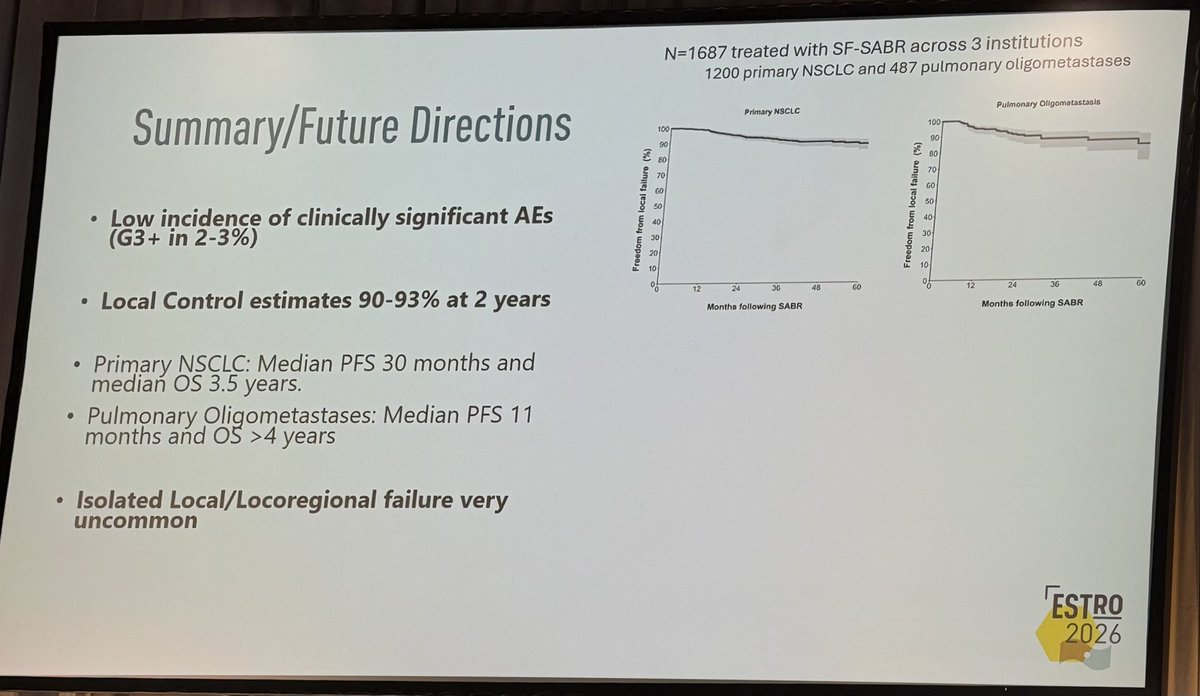
TL;DR2-yr local control 90-93% and G3+ AEs 2-3% across 1687 pts (1200 primary NSCLC, 487 oligomets) treated with single-fraction SABR.
The transfer gate is the fraction size the source omits: outcomes are labeled single-fraction but no Gy dose is given, so you cannot map this 2y LC of 90-93% onto a specific regimen before offering one visit instead of a multi-fraction course. Toxicity (G3+ 2-3%) comes from 2 of 3 sites only. Moves the single- vs multi-fraction choice for lung SABR.
+2 more figures
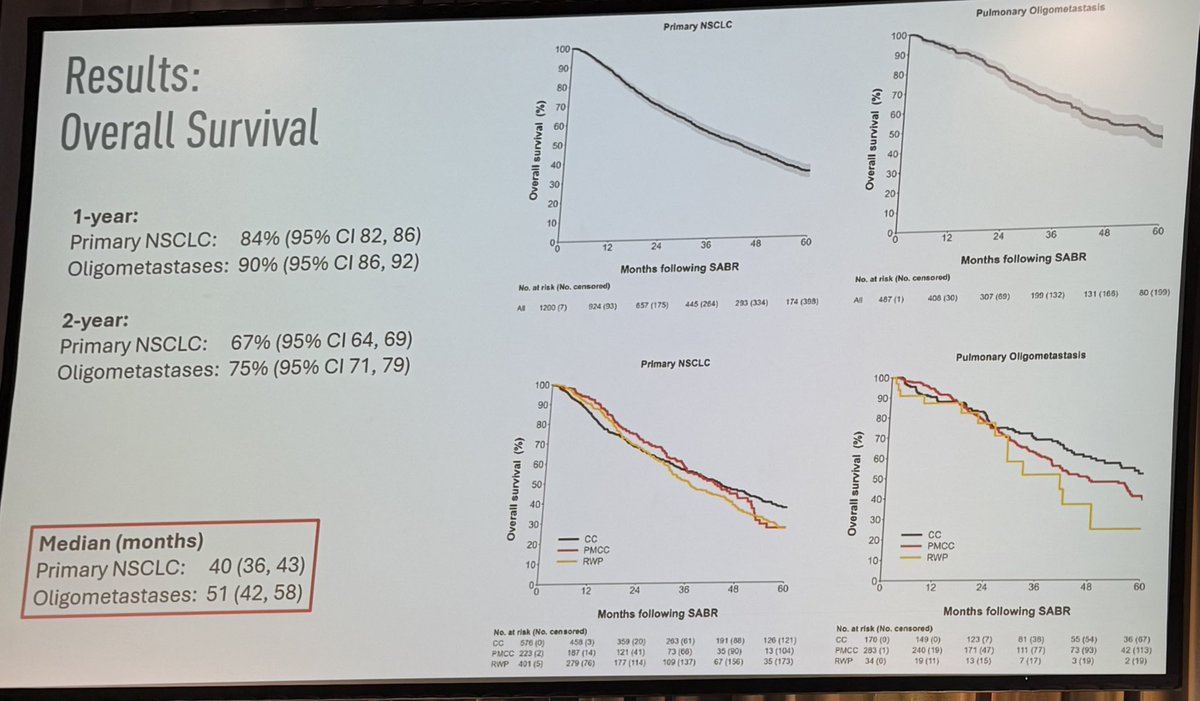
| Endpoint | Primary NSCLC | Oligomets |
|---|---|---|
| 1-yr OS | 84% (82-86) | 90% (86-92) |
| 2-yr OS | 67% (64-69) | 75% (71-79) |
| Median OS | 40 mo (36-43) | 51 mo (42-58) |
7 details 1 trial watching
Pooled retrospective analysis of 3 institutions (Peter MacCallum, Cleveland Clinic, Roswell Park). N=1687 (1200 primary NSCLC, 487 pulmonary oligometastases). No randomisation, no comparator arm; survival curves out to 60 months.
Primary NSCLC (n=1200) and pulmonary oligometastases (n=487) treated with single-fraction SABR. Stage, tumour location, and specific eligibility criteria not reported in source.
Single-fraction SABR across all pts. The Gy dose is not reported in source (single fraction only), so the specific regimen behind these outcomes is unknown, gating whether the result transfers to a given practice.
No prespecified primary endpoint stated. Reported: local control, overall survival, PFS, and adverse events.
2y local control 90-93%; isolated local/locoregional failure very uncommon. Median PFS 30 mo (NSCLC) vs 11 mo (oligomets). OS by cohort shown in the figure.
G3+ AEs 2-3% (23/789, 2.9% in the assessed NSCLC subset); G2+ 124/789 (15.7%), any AE 215/789 (27%). AE data from 2 of 3 sites only (no Roswell Park).
Consistent with SAFRON II (TROG 13.01) and RTOG 0915 supporting single-fraction lung SABR, but those were randomised; this pooled cohort carries no comparator.
Retrospective, no randomised/matched comparator. Single-fraction Gy dose unstated. AE denominator excludes one of three sites (n=789 of 1687).
Pooled retrospective single-arm cohort, no randomised or matched comparator vs multi-fraction SABR; single-fraction Gy dose unstated. Consistent with SAFRON II / RTOG 0915.
In pts with primary NSCLC or a pulmonary oligometastasis being considered for SABR, this supports single-fraction delivery as a lower-visit option with high local control; it does not establish it over a multi-fraction schedule, which this cohort did not compare against.
- Single-fraction vs multi-fraction SABR in a randomised comparison active A Pilot Study of Single Fraction Stereotactic Body Radiation Therapy (SBRT) in Central Non-Small Cell Lung Cancer Phase NAn=30 · primary completion 2028-03 · single-fx vs multi-fx SBRT in central NSCLC
- Optimal single-fraction dose across primary NSCLC and pulmonary oligometastases
📚 Sources · 🐦 1 tweet
👏🏽👏🏽👏🏽@neildwallaceie at #ESTRO26 - 1687 patients receiving single fraction SABR for #lungcancer and pulmonary oligomets, @PeterMacRadOnc / @ClevelandClinic / @RoswellPark. Fantastic local control, and low adverse rates. Should we be using “one stop” SABR more often #radonc ? pic.twitter.com/w2IlGKRU5o
— Shankar Siva (@_ShankarSiva) May 18, 2026
HEAT Trial NCT01794403
ForLocalized low- to intermediate-risk prostate cancer, IPSS <12
7% vs 7.4% (AHRT vs EHRT)
Non-inferior, P=0.007 at 4.25y; NI margin 12%
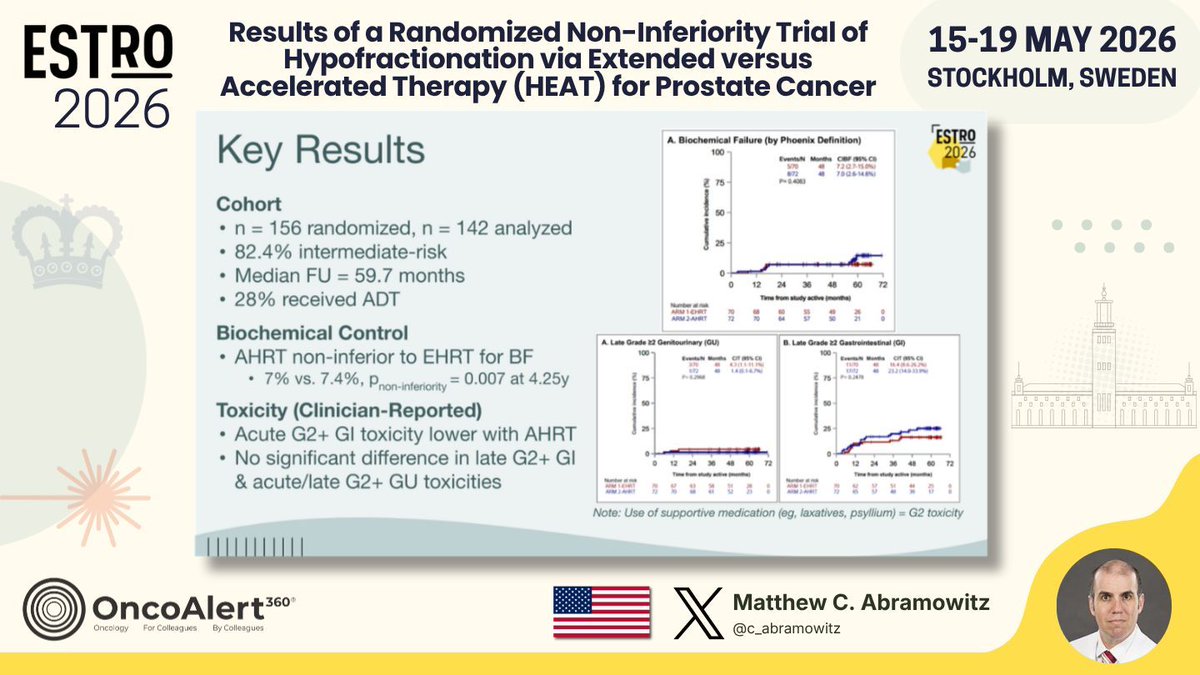
TL;DRAHRT 5fx non-inferior to EHRT 26fx for biochemical failure, 7% vs 7.4% (P_NI=0.007) at 4.25y; less acute GI toxicity.
The head-to-head prior SBRT trials skipped: 5fx AHRT (36.25 Gy, SIB 40 Gy) vs 26fx EHRT, both IMRT with ADT allowed, isolating fractionation from technique and hormones. Acute G2+ GI toxicity favored the 5fx arm at equal biochemical control, moving the ultrahypofractionation choice for low- to intermediate-risk pts.
| Arm | Biochemical failure (4.25y) | P (NI) |
|---|---|---|
| AHRT | 7% | 0.007 |
| EHRT | 7.4% | ref |
+1 more figure
8 details 4 trials watching
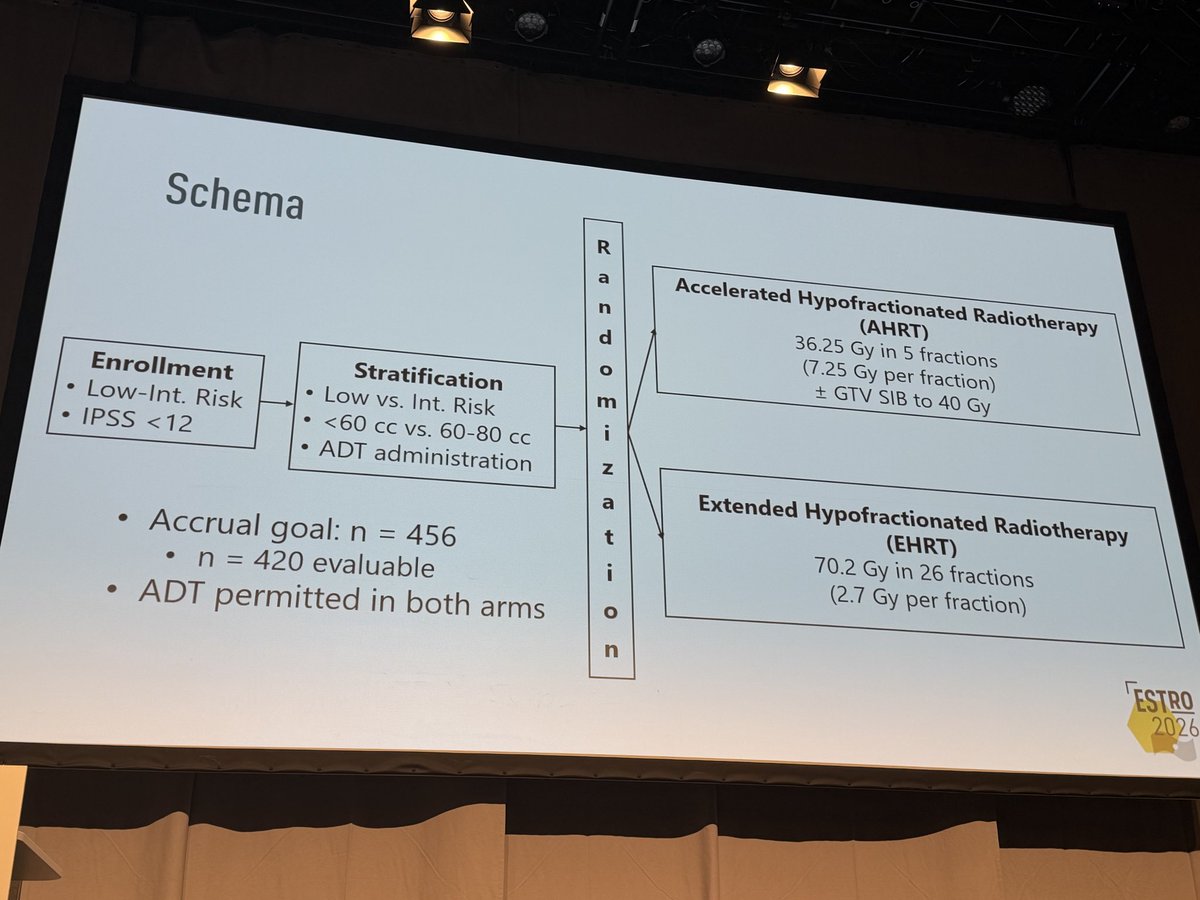
Phase 3 international non-inferiority RCT, 1:1, biochemical failure (Phoenix) primary, NI margin 12%. Interim analysis at 142 analyzed of 456 planned; median follow-up 59.7 mo.
Localized low- to intermediate-risk prostate cancer, IPSS <12. 82.4% intermediate-risk; stratified by risk, gland volume (<60 vs 60-80cc), and ADT. 28% received ADT (≤6 mo, both arms).
AHRT 36.25 Gy/5 fx (7.25 Gy/fx) + GTV SIB to 40 Gy vs EHRT 70.2 Gy/26 fx (2.7 Gy/fx), IMRT in all patients.
AHRT non-inferior to EHRT for biochemical failure: 7% vs 7.4%, P non-inferiority=0.007 at 4.25y.
| Arm | Dose / fractionation | Boost / technique |
|---|---|---|
| AHRT | 36.25 Gy / 5 fx (7.25 Gy/fx) | GTV SIB to 40 Gy |
| EHRT | 70.2 Gy / 26 fx (2.7 Gy/fx) | IMRT all pts |
Acute G2+ GI toxicity lower with AHRT. No significant difference in late G2+ GI or acute/late G2+ GU toxicity. Supportive-med use (laxatives, psyllium) counted as G2.
First RCT comparing AHRT vs EHRT 1:1 with modern IMRT and ADT. Prior ultrahypofractionation trials (HYPO-RT-PC, PACE-B, NRG-GU005) used heterogeneous or no-ADT controls.
Interim analysis at roughly one-third of planned accrual; full pre-specified primary pending. Small analyzed N (142); biochemical, not clinical, endpoint.
Interim analysis at 142 of 456 planned pts; non-inferiority met but full pre-specified primary analysis pending. Underpowered vs accrual goal.
In localized low- to intermediate-risk prostate with IPSS <12, this supports 5fx AHRT as non-inferior to 26fx EHRT with less acute GI toxicity; it does not extend to high-risk disease or glands >80cc, which the trial excluded.
- Durability of biochemical control at full accrual and longer follow-up recruiting Androgen Suppression Combined With Nodal Irradiation and Dose Escalated Prostate Treatment Phase 3n=710 · primary completion 2032-10 · phase 3 SBRT vs EBRT + brachytherapy boostrecruiting PRO-BOOST-LC: Whole-Gland Boost Strategies Versus SBRT Monotherapy in PSMA-Staged Localized and Locally Advanced Prostate Cancer Phase 2/3n=1200 · primary completion 2033-12 · SBRT monotherapy vs whole-gland boost
- Does 5fx AHRT benefit extend to high-risk or larger-gland prostate? recruiting Testing Shorter Duration Radiation Therapy Versus the Usual Radiation Therapy in Patients With High Risk Prostate Cancer Phase 3n=1209 · primary completion 2036-03 · phase 3 5fx SBRT vs usual RT, high-risk
- Long-term late GU/GI toxicity with 5fx AHRT n=42 · primary completion 2028-01 · 5fx SABR, urethra/rectum-sparing, GU/GI AE
📚 Sources · 🐦 2 tweets
Day FOUR of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 18, 2026
Results of a Randomized Non-Inferiority Trial of Hypofractionation via Extended versus Accelerated Therapy (HEAT) for Prostate Cancer Presented by Matthew C. Abramowitz🇺🇸 #RadOnc ☢️ #ProstateCancer
HEAT is an international phase… pic.twitter.com/IkSTgQHwXK
The HEAT trial is another randomized demonstration of the safety & efficacy of SBRT compared to hypofractionted RT in #prostatecancer at #ESTRO26 pic.twitter.com/c9sNb3KOqo
— Pierre Blanchard, MD (@PBlanchardMD) May 18, 2026
INRT-AIR & DARTBOARD pooled analysis
ForOropharynx/larynx/hypopharynx HNSCC, stage I-IVB, excl T1-2N0 larynx
TL;DR5-yr solitary elective nodal recurrence 0% with ENI omission across 117 pts; 5-yr OS 87%, PFS 74%.
The failure pattern is what matters: solitary elective nodal recurrence was 0% at 5 yrs while 3-yr local recurrence ran 9.5% and distant 11%, so the residual risk sits in the primary and systemically, not in the uncovered elective levels. Node selection was AI-assisted off PET/CT plus neck CT, which gates whether the volume reproduces outside these trials.

| Endpoint | Timepoint | Value |
|---|---|---|
| Solitary elective nodal recurrence | 5-year | 0% |
| Local recurrence | 3-year | 9.5% |
| Regional recurrence | 3-year | 4.3% |
| Distant metastasis | 3-year | 11% |
| Overall survival | 5-year | 87% |
| Progression-free survival | 5-year | 74% |
| Composite MDADI (mean) | 12 months | 84.9 |
+1 more figure

10 details 5 trials watching
Patient-level pooled analysis of two prospective trials of involved nodal RT, INRT-AIR and DARTBOARD. N=117, median follow-up 3.4 years. No randomised ENI comparator arm.
HNSCC of oropharynx, larynx, and hypopharynx, stage I-IVB, excluding T1-2N0 larynx. Completed PET/CT and neck CT required for entry.
INRT omits elective nodal irradiation, treating involved nodes only, with an artificial-intelligence model assisting identification of suspicious lymph nodes. Dose, fractionation, and margin not reported in source.
5-yr solitary elective nodal recurrence 0%. 3-yr cumulative incidence: local 9.5%, regional 4.3%, distant 11%. 5-yr OS 87%, PFS 74%.
Mean composite MDADI 84.9 at 12 months, with no significant decline after treatment. No late G3+ toxicity, xerostomia, or feeding-tube rates reported in source.
Pooled single-arm data with no ENI control, so the 0% solitary elective recurrence carries no randomised contrast. Median follow-up 3.4 yrs underpins 5-yr estimates, and the AI nodal-selection step is not externally reproduced.
The dosimetric case for INRT rests on OAR sparing, but the only patient-reported outcome here is swallowing (MDADI 84.9), with no xerostomia or dysphagia comparison against ENI. Authors state randomized evidence is required before non-trial implementation.
Pooled single-arm prospective cohorts, N=117, no randomised ENI comparator; presenters explicitly require randomised evidence before non-trial use.
In PET/CT-staged oropharynx, larynx, or hypopharynx HNSCC (excluding T1-2N0 larynx) being planned for definitive chemoRT, this supports enrolling on an INRT trial rather than omitting elective nodal coverage off-protocol, and it does not speak to node-positive necks staged without PET/CT.
- Does INRT reduce late toxicity vs ENI in a randomized comparison? recruiting Dose De-escalation and Sentinel LN Mapping Driven Radiotherapy of Contralateral Neck in Ipsilateral Node Positive HNSCC Phase NAn=147 · primary completion 2027-01 · tests contralateral elective volume + dose reductionrecruiting Personalized Elective Neck Irradiation Guided by Sentinel Lymph Node Biopsy in Larynx and Pharynx Cancer. The PRIMO Study. Phase 3n=242 · primary completion 2029-12 · phase 3 SLNB-guided vs standard ENI, 242 pts
- Is the AI nodal-selection step reproducible outside these two trials? not yet SPECT-CT Guided ELEctive Contralateral Neck Treatment in Lateralized Oropharyngeal Cancer Phase NAn=128 · primary completion 2030-04 · SPECT-CT lymphatic mapping to select elective volume
- Does INRT hold for HPV-negative and oral cavity primaries? recruiting Personalized Neck Radiation Therapy Directed by Sentinel Lymph Node Biopsy for the Treatment of Oral Cavity Squamous Cell Carcinoma, PRECEDENT Trial Phase 2n=50 · primary completion 2030-07 · SLNB-directed neck RT in oral cavity SCC, cT1-4arecruiting Comparing Sentinel Lymph Node (SLN) Biopsy With Standard Neck Dissection for Patients With Early-Stage Oral Cavity Cancer Phase 2/3n=686 · primary completion 2031-04 · SLNB vs elective neck dissection, early oral cavity
📚 Sources · 🐦 1 tweet
Day FOUR of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 18, 2026
Omission of elective nodal irradiation in HNSCC: long-term results and patient-level pooled analysis from 2 prospective trials (INRT-AIR & DARTBOARD)
Presenter Sympascho Young 🇺🇸
A patient-level pooled analysis of 117 patients… pic.twitter.com/KaaT70nSNH
FASTRACK II NCT02613819
ForPrimary RCC ≤10 cm, medically inoperable or declined surgery, N0-N1
100% at 36, 60, and 84 mo
RECIST, intention-to-treat population; median f/u 62 mo
TL;DR100% freedom from local progression at 36, 60, and 84 months after single-fraction 26 Gy or 42 Gy/3fx SABR in inoperable primary RCC.
The size-adapted prescription is what transfers: 26 Gy × 1 for ≤4 cm, 42 Gy/3fx at 48 h intervals above that, in a cohort that was 65% T1b or higher (median 46 mm), not a small-tumour-enriched series. Two colonic obstructions place bowel as the constraint for central lesions.
10 details
Non-randomised phase 2, eight hospitals in Australia and the Netherlands (TROG 15.03, with ANZUP). Accrual July 28 2016 to Feb 27 2020: 71 enrolled, one withdrew consent before treatment, 70 treated. This report is the pre-planned final long-term follow-up, median 62 months (IQR 60-72).
Histologically confirmed primary RCC in pts who were medically inoperable, high risk, or declined surgery; ECOG ≤2; tumour ≤10 cm; N0-N1. Median age 77 (70-82), 70% male. Median tumour size 46 mm (37-55): T1a 34%, T1b 56%, T2a 9%, T3a 1%, with one N1 pt.
Size-adapted prescription: 26 Gy in a single fraction for tumours ≤4 cm, and 42 Gy in 3 fractions delivered 48 h apart for tumours >4 cm. No systemic therapy component.
Primary: freedom from local progression by RECIST, assessed in the intention-to-treat population, with safety co-assessed in ITT.
100% local control at 36, 60, and 84 months, with no local recurrences and no cancer-related deaths reported over median 62-month follow-up.
Seven pts (10%) had at least one treatment-related grade 3 event within 9 months: pain (abdominal/flank/tumour) 4 (6%), nausea and vomiting 3 (4%), colonic obstruction 2 (3%), diarrhoea 1 (1%). No grade 4 events, no treatment-related deaths, and no new long-term safety signals.
Single-arm and non-randomised: no head-to-head against partial nephrectomy, cryoablation, or radiofrequency ablation, which is the live comparison in the surgery-declining subset. N=70 with one N1 pt leaves nodal disease essentially untested. Industry co-funding (Varian) alongside Cancer Australia.
The value here is durability rather than magnitude: a flat 100% at 84 months in a cohort with median 46 mm tumours argues the ablative dose is adequate for lesions well beyond the small-renal-mass range where thermal ablation is usually deployed. The bowel events, not renal function, define the practical constraint for central tumours on the 3-fraction schedule.
Single-arm phase 2; no randomised comparator vs nephrectomy or thermal ablation. Long f/u and 100% local control do not lift a non-randomised design.
For a medically inoperable or surgery-declining pt with a T1b-T2a primary RCC ≤10 cm, this supports SABR as a definitive local option with durable 84-month local control; it does not address the surgically fit pt in whom partial nephrectomy remains untested against SABR.
- SABR vs partial nephrectomy in surgically fit pts
- SABR vs thermal ablation for T1b tumours
- Long-term renal function after single-fraction 26 Gy
📚 Sources · 📄 1 paper
Abstract
PRIME NCT03561961
ForHigh-risk, very high-risk and/or node-positive non-metastatic prostate, 2y ADT
Not yet mature
Interim: no signal of inferiority for SBRT arm; 4-5y data awaited
TL;DRInterim data: 36.25 Gy/5 fx SBRT with whole-pelvis RT and 2y ADT shows no inferiority signal vs 68 Gy/25 fx; BFFS immature.
The transferable point is the pelvic dose: 25 Gy / 5 fx elective nodal with SIB permitted to involved nodes, grade 3+ under 1%, which is the constraint question that has kept 5-fraction prescribing confined to node-negative prostate-only. HYPO-RT-PC never tested nodes or ADT, so this extends the ultrahypofractionation toxicity envelope, not its efficacy.

| Toxicity (Grade ≥2) | SBRT (5 fx) | Moderate Hypo (25 fx) | p |
|---|---|---|---|
| Acute GU | ~5.4% | ~4.0% | 0.59 |
| Acute GI | ~2.2% | ~3.7% | 0.20 |
| Late GU | ~10-12% | ~9-11% | NS |
| Late GI | ~5-7% | ~4-6% | NS |
| Grade 3+ GU/GI | <1% | <1% | n/a |
+1 more figure

| HYPO-RT-PC | PRIME | |
|---|---|---|
| Experimental arm | 42.7 Gy / 7 fx | 36.25 Gy / 5 fx |
| Control arm | 78 Gy / 39 fx | ~68 Gy / 25 fx |
| Accrual | 2010 - 2015 | 2018 - 2023 |
| Primary endpoint result | 10y FFS 72% vs 65%, HR 0.84 (0.69-1.03) | Not yet mature |
10 details 5 trials watching
Phase III, open-label, randomized non-inferiority trial, Tata Memorial Centre and collaborating Indian centers. Accrual 2018-2023, completed at N~434, randomized 1:1 stratified by risk group and nodal status. Median follow-up is interim, 1-2 years.
High-risk, very high-risk and/or node-positive non-metastatic prostate cancer; ECOG 0-2; life expectancy 10 years. PSMA PET/CT staging permitted, which matters for how the node-positive stratum was defined relative to older conventionally-staged trials.
Arm A 36.25 Gy in 5 fractions (7.25 Gy/fx), every other day; Arm B ~68 Gy in 25 fractions (2.7 Gy/fx) over ~5 weeks. Both arms received prostate plus whole-pelvis elective nodal RT at 25 Gy / 5 fx (or equivalent), with SIB to positive nodes allowed in the SBRT arm. Delivered in the modern IMRT/VMAT with daily IGRT era.
Long-course ADT, ~2 years, in both arms. ADT is not a randomized variable here, so the trial isolates fractionation, not the systemic question.
Primary: biochemical failure-free survival (Phoenix, nadir + 2 ng/mL). Secondary: acute and late toxicity (RTOG/CTCAE v4.0/5.0), OS, MFS, clinical failure-free survival, QoL (QLQ-C30, QLQ-PR25, IPSS), cost-effectiveness.
Interim only. Source reports no signal of inferiority for the SBRT arm on BFFS and no difference in MFS or OS in early follow-up; no HR, CI, or non-inferiority margin is reported in source. OS data explicitly immature.
No significant difference in grade ≥2 toxicity between arms: acute GU ~5.4% vs ~4.0% (p=0.59), acute GI ~2.2% vs ~3.7% (p=0.20); late grade ≥2 GU ~10-12% vs ~9-11% and GI ~5-7% vs ~4-6%, both NS. Grade 3+ under 1% in both arms, acute and late. Urinary and bowel QoL domains stable and comparable.
HYPO-RT-PC established ultrahypofractionation non-inferiority (10y FFS 72% vs 65%, adjusted HR 0.84, 95% CI 0.69-1.03) but in node-negative disease, prostate plus proximal seminal vesicles only, no pelvic RT, no ADT, mostly 3D-CRT. PRIME is testing a different question: 5 fractions with elective nodal coverage on top of 2y ADT.
Interim analysis at 1-2 years against a BFFS primary read under 2 years of ADT, where testosterone suppression flattens both curves and early concordance is close to uninformative. Toxicity is reported as approximate ranges rather than point estimates with CIs. Open-label, though toxicity grading and PSA endpoints are only modestly susceptible to that.
Interim analysis at 1-2y of a BFFS primary that needs 4-5y maturity; safety-only read. Interim data cannot promote past early-signal regardless of clean design.
In high-risk or node-positive non-metastatic prostate going to whole-pelvis RT with long-course ADT, this supports 5-fraction SBRT as tolerable but not yet as an efficacy-equivalent substitute; it says nothing about omitting ADT or treating without pelvic coverage.
- Mature 4-5y BFFS and non-inferiority margin recruiting Androgen Suppression Combined With Nodal Irradiation and Dose Escalated Prostate Treatment Phase 3n=710 · primary completion 2032-10 · ph3 nodal RT + prostate SBRT vs EBRT/brachy boost
- Late GU toxicity beyond 2y with nodal SIB active Hypofractionated Whole-Pelvis Radiotherapy (WPRT) vs Conventionally-Fractionated WPRT in Prostate Cancer Phase 2n=58 · primary completion 2024-03 · 5fx vs 25fx whole-pelvis RT, QoL primaryrecruiting Phase III Adaptive Adaptive Stereostactic Body Radiotherapy (SBRT) With Dose Escalation for High-Risk Prostate Cancer Phase NAn=390 · primary completion 2033-04 · adaptive SBRT with WPRT plus DIL boost, 5y outcomes
- Whether pelvic nodal RT itself adds benefit in this population n=224 · primary completion 2017-08 · whole-pelvis vs prostate-only RT, high risk, 5y EPrecruiting A Trial of 5 Fraction Prostate SBRT Versus 5 Fraction Prostate and Pelvic Nodal SBRT Phase 3n=1128 · primary completion 2028-06 · randomises 5fx prostate vs prostate+pelvic nodal SBRT
📚 Sources · 🐦 1 tweet
PRIME trial
— Rohit Malde (@roxboxfix) May 18, 2026
Can we safely deliver ultra-short SBRT including pelvic nodal irradiation in biologically aggressive disease treated with ADT?
With Pelvic RT
Moderate hypofractionation:
~68 Gy/25#/5w
Vs
Extreme hypofractionation/SBRT:
36.25 Gy / 5 # /1-2w
Compare HYPO RT PC pic.twitter.com/7NABknLsD5
PACE-NODES
ForHigh-risk localised prostate (T3a-T4, Gleason 8-10, or PSA>20), planned 12-36mo…
28% vs 21%
PPN-SBRT vs P-SBRT; no difference at 12wk, symptoms resolved quickly
TL;DRGrade ≥2 GI toxicity 28% vs 21% with added pelvic nodal SBRT over 12wk; GU unchanged, symptoms resolved by 12wk.
The deliverability number is the buried read: 11% of PPN-SBRT pts never received the allocated treatment vs 4% prostate-only, mostly unmet constraints. Nodal dose was 25Gy/5f alongside 36.25Gy/5f prostate on alternate days. That gates whether 5f elective nodal coverage is exportable outside high-volume centres, before any efficacy signal arrives.

| Endpoint | PPN-SBRT | P-SBRT |
|---|---|---|
| CTCAE grade ≥2 GI to 12wk | 28% | 21% |
| Did not receive allocation | 11% | 4% |
+2 more figures

7 details 5 trials watching
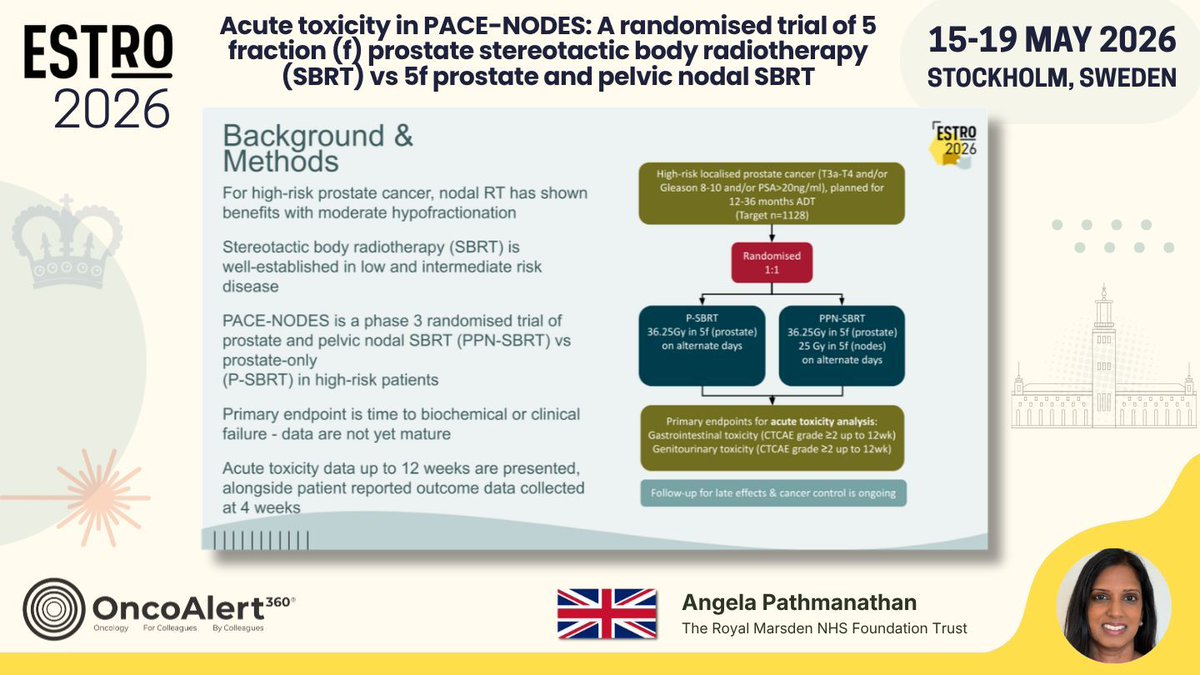
Phase 3 randomised, 1:1, multicentre. 1166 pts randomised against a target of 1128. This report is the prespecified acute toxicity analysis; the trial's primary endpoint, time to biochemical or clinical failure, is not yet mature.
High-risk localised prostate cancer: T3a-T4 and/or Gleason 8-10 and/or PSA >20 ng/ml. All planned for 12-36 months ADT.
Both arms 36.25Gy in 5f to prostate on alternate days. PPN-SBRT adds 25Gy in 5f to pelvic nodes. 11% of PPN-SBRT vs 4% of P-SBRT did not receive allocation, mostly because dose constraints were not met.
Co-primary for this analysis: CTCAE grade ≥2 GI and GU toxicity to 12 weeks. Patient-reported EPIC-26 domain scores collected at 4 weeks.
Grade ≥2 GI symptoms were more frequent with PPN-SBRT (28% vs 21%) across the 12-week window, with no difference at 12 weeks. No difference in acute GU toxicity by clinician or patient report. EPIC-26 bowel domain at 4 weeks mirrored the clinician-scored GI gap.
Acute window only, capped at 12 weeks; late GI/GU effects and cancer control are still accruing. Toxicity scoring is unblinded, which matters most for clinician-graded GI events. Effect sizes for the GI difference (CI, p) were not reported in source.
Randomised, but this is an acute-toxicity readout only; the primary biochemical/clinical failure endpoint is explicitly immature. Safety supports feasibility, not adoption.
In high-risk localised prostate on long-course ADT, this supports 5f nodal SBRT as tolerable in the acute window; it does not yet inform whether to cover nodes, since the biochemical/clinical failure endpoint is immature.
- Late GI/GU toxicity beyond 12 weeks n=68 · primary completion 2025-10 · 5y cumulative GI/GU toxicity after prostate SBRTn=500 · primary completion 2027-12 · 1° EP is late GI toxicity after prostate SBRT
- Biochemical and clinical failure benefit from nodal coverage recruiting A Trial of 5 Fraction Prostate SBRT Versus 5 Fraction Prostate and Pelvic Nodal SBRT Phase 3n=1128 · primary completion 2028-06 · phase 3 prostate vs prostate+pelvic nodal SBRT, n=1128recruiting Phase II Trial of PSA Response-based Androgen Deprivation Therapy and Nodal Coverage for Prostate Cancer Early Salvage Radiotherapy (RANGER) Phase 2n=68 · primary completion 2030-11 · PSA-adapted sequential pelvic nodal RT in salvage fossarecruiting PRO-BOOST-N: Prostate-First Versus Combined Prostate and Nodal Dose Escalation in PSMA PET-Staged Node-Positive Prostate Cancer Phase 2/3n=1600 · primary completion 2033-12 · randomises nodal dose escalation in cN1M0 PSMA-staged
- Whether unmet nodal dose constraints limit delivery outside trial centres
📚 Sources · 🐦 1 tweet
Day THREE of #ESTRO26 Coverage by OncoAlert 🚨
— OncoAlert (@OncoAlert) May 17, 2026
Acute toxicity in PACE-NODES: A randomised trial of 5 fraction (f) prostate stereotactic body radiotherapy (SBRT) vs 5f prostate and pelvic nodal SBRT
Presented by Angela Pathmanathan 🇬🇧 #RadOnc ☢️ #ProstateCancer
PACE-NODES is a… pic.twitter.com/z9bAOiKSIy
OLIGOMA NCT04495309
ForOligometastatic breast, ≤5 lesions, any line, mostly ER+/HER2- first line
35.8 vs 20.4 mo, HR 0.48
95% CI 0.25-0.91, p=0.021
TL;DRmPFS 35.8 vs 20.4mo, HR 0.48 (0.25-0.91), p=0.021 for MDT to all lesions in oligometastatic breast, QoL non-inferior.
The RT read is who was actually irradiated: 2/3 of lesions were bone and >80% of pts had 1-3 mets, so this is largely bone-directed ablative RT in first-line ER+ disease, not a visceral-oligomet population. Dose and fractionation are not reported in source, which gates transfer to practice. QoL non-inferiority at 12wk (-2.1, margin -10) removes the main argument against adding local therapy to a working systemic backbone.

+3 more figures

| Arm | QLQ-C30 mean at 12wk (95% CI) | Between-group change (ANCOVA) |
|---|---|---|
| Experimental | 72.2 (67.2-77.2) | -2.1 (-9.2-5.1) |
| Control | 74.3 (69.3-79.3) | n/a |


9 details 5 trials watching
Randomised trial (ARO-2021-09, NCT04495309) of systemic therapy alone vs systemic therapy plus local ablative radiotherapy to all metastatic lesions. Randomisation stratified by type of systemic therapy and treatment line. N=87 (43 experimental, 44 control).
Metastatic breast cancer, any treatment line, maximum 5 metastatic lesions, with the systemic regimen determined by multidisciplinary tumour board. Pts requiring palliative RT to all metastases were not eligible, though palliative RT to symptomatic sites was allowed. Median age 58 / 59; ECOG 0 in 76.7% of the experimental arm.
The intervention is local ablative radiotherapy to all metastatic lesions on top of the systemic backbone. Dose, fractionation, modality, and target-volume definition are not reported in the source slides, and 2/3 of treated lesions were bone metastases.
Co-primary: progression-free survival and quality of life (EORTC QLQ-C30) at 12 weeks post-randomisation. Secondary: overall survival, toxicity, compliance, QLQ-C30 and QLQ-BR23, and patient satisfaction with cancer care (EORTC PATSAT C33).
Both co-primaries read out in favour of adding MDT: PFS separated at HR 0.48 and the QoL summary score met non-inferiority against a -10 point margin. See the figure captions for the arm-level values.
Recruitment stopped early at <20% of the initial and <40% of the amended target, leaving N=87 and a wide HR CI (0.25-0.91). Open-label design with a patient-reported co-primary. No OS data reported in source, and the toxicity secondary endpoint is likewise absent from the presented slides.
The presenter frames this as the first RCT showing a PFS benefit from MDT in oligometastatic breast cancer, extending the STOMP / SABR-COMET line of evidence into a histology where systemic control is comparatively good. Eight further randomised trials are accruing, so the magnitude here should be read as provisional.
Randomised but stopped early at <20% of initial accrual target; N=87 with wide HR CI (0.25-0.91). Underpowered for a durable PFS estimate.
In ER+/HER2- breast cancer with 1-3 mostly bony metastases on first-line systemic therapy, this supports discussing ablative RT to all lesions as a PFS-directed addition; it does not extend to >5 lesions, heavily visceral disease, or pts needing palliative RT to every site.
- Does the PFS benefit translate to overall survival n=340 · primary completion 2026-11 · JCOG phase 3 MDT vs systemic alone, 340 pts
- Which oligometastatic breast subgroups benefit most active Standard Treatment +/- SBRT in Solid Tumors Patients With Between 1 and 5 Bone-only Metastases Phase NAn=168 · primary completion 2025-07 · SBRT vs none in 1-5 bone-only mets, breast inclrecruiting BreCLIM-2 - A RCT Investigating Local Treatment for Breast Cancer Liver Metastases Phase 3n=200 · primary completion 2029-12 · RCT of local tx in 1-4 breast liver metsnot yet Adding Surgery and Radiation to the Usual Treatment for HER2-Positive Breast Cancer That Had Already Spread at Diagnosis Phase 3n=562 · primary completion 2032-05 · HER2+ de novo stage IV, 1-5 mets, SBRT added
- Optimal RT dose and fractionation for bone-dominant oligomet breast recruiting OligoCare TwiCs (Trials Within Cohorts) Trial Comparing Acute Toxicity in Single-fraction vs Multiple-fraction SBRT for Metastasis-directed Treatment (SPRINT) Phase NAn=302 · primary completion 2029-02 · single-fraction vs multifraction SBRT, breast incl
📚 Sources · 🐦 3 tweets
📌 Metastases-directed treatment in Patients with Oligometastatic Breast Cancer: Results from the OLIGOMA-trial (ARO-2021-09, NCT04495309) @DavidKrugMD 👏🏻 #ESTRO26 @ESTRO_RT @OncoAlert #OncoAlertAF pic.twitter.com/YDMef0fXRm
— Elisabetta Bonzano MD, PhD (@to_be_elizabeth) May 17, 2026
❗️ The OLIGOMA trial results just dropped at #ESTRO26 and they are massive. A 15-month improvement in median PFS for OMD breast cancer (HR = 0.48). This adds to the growing mountain of evidence that MDT (Metastasis-Directed Therapy) works. Lets’s go 🧵 1/n pic.twitter.com/5uiEVSYtdH
— NonsparseOncologist (@5_utr) May 17, 2026
Here are some details!
— Jeff Ryckman (@jryckman3) May 17, 2026
On OLIGOMA, nearly 3/4 were first line endocrine or chemotherapy. #ESTRO26 #OncTwitter@CJTsaiMDPhD pic.twitter.com/r3kJzNNsyK
EXTEND
ForOligometastatic solid tumors, mixed histology, on standard-of-care systemic…
TL;DRPrimary aggregated analysis across all tumor-histology baskets now published in JCO; no effect sizes reported in source tweet.
The aggregated all-basket read is the gate for whether MDT generalizes beyond the single histologies that carry their own randomized data, so it moves the offer-MDT-or-not decision in mixed-histology oligomet. No effect sizes, RT dose, fractionation, or target volume appear in the source text.
Also covered May 18
7 details
Phase II randomized trial of metastasis-directed therapy added to standard of care vs standard of care alone in oligometastatic solid tumors. This report is the primary analysis of all tumor-histology baskets pooled.
No effect sizes are reported in the source, which is a tweet plus a JCO title-page image. Primary endpoint, medians, HRs, and follow-up all require the full text.
Pooling across histology baskets can obscure heterogeneity between them. MDT technique, dose, fractionation, and target volume are not stated in source, so transferability to a specific RT practice cannot be judged here.
Phase II randomized basket design caps the read at hypothesis-generating; source gives no primary endpoint, effect size, or follow-up to classify further.
- Which histology baskets drive the pooled estimate
- Whether ctDNA selects pts who benefit from MDT
- Confirmatory phase 3 in mixed-histology oligomet
📚 Sources · 🐦 1 tweet
1/ Tremendous thanks to the patients, coauthors and all who made the EXTEND trial possible. The primary aggregated analysis is now available online @JCO_ASCO with ctDNA correlatives presented synchronously at @ESTRO_RT #ESTRO26 pic.twitter.com/Zoy8DGRWbW
— Alexander Sherry (@AlexSherryMD) May 17, 2026