Systemic
STAMPEDE (abiraterone ± enzalutamide, high-risk non-metastatic) NCT00268476
ForHigh-risk M0 prostate: node+ or ≥2 of T3-4/Gleason 8-10/PSA≥40
TL;DRMFS HR 0.53 (6yr 82% vs 69%) and OS HR 0.60 adding 2yr abiraterone to ADT in high-risk M0 prostate (85% also had RT).
The RT read: abiraterone sits on top of definitive ADT+RT (74Gy/37fx to prostate+SV in the 85% who got RT), not RT vs no-RT. It moves systemic intensification for the high-risk M0 pt you're already irradiating; enzalutamide adds nothing over abiraterone (interaction HR 1.02, p=0.91).
8 details 2 trials watching
Pooled meta-analysis of two open-label phase 3 RCTs within the STAMPEDE platform, 113 UK/Swiss sites, N=1974, randomized 1:1. Median follow-up 72 mo (60-84).
High-risk non-metastatic disease: node-positive, or if node-negative ≥2 of T3/T4, Gleason 8-10, PSA ≥40; or high-risk relapse. Median age 68, median PSA 34; 39% node-positive.
Abiraterone 1000mg + prednisolone 5mg daily for 2yr added to 3yr ADT; the second trial's combination arm also received enzalutamide 160mg. Control = ADT alone.
RT planned in 85% (1684/1974): 74Gy/37fx to prostate + seminal vesicles or hypofractionated equivalent. Mandated if node-negative, encouraged if node-positive.
Primary: metastasis-free survival. Secondary: OS, prostate cancer-specific survival, biochemical failure-free survival, PFS, and toxicity.
Adding enzalutamide to abiraterone gave no extra MFS benefit (interaction HR 1.02, p=0.91), with no between-trial heterogeneity.
Open-label design, though MFS/OS are hard endpoints less prone to ascertainment bias. Pooled across two platform trials; no radiotherapy-treated subgroup HR reported in the source excerpt.
Two randomised phase 3 trials pooled; MFS primary hit (HR 0.53) with concordant OS benefit at 72mo, applicable high-risk M0 population. Adding enzalutamide gave no extra benefit.
In high-risk M0 prostate (node+, or ≥2 of T3-4/Gleason 8-10/PSA≥40) going to definitive ADT+RT, this supports adding 2yr abiraterone; it does not extend to lower-risk localized disease, and adding enzalutamide buys nothing.
- Optimal duration of abiraterone (2yr fixed used here)
- Whether benefit holds when radiotherapy is omitted
- Long-term OS and cure fraction beyond 72 months recruiting A Study of Metastases Free Survival With Saruparib vs Placebo Added to a Standard RT/ADT in Men With High-risk Prostate Cancer With a BRCA Mutation Phase 3n=700 · primary completion 2033-03 · MFS endpoint, high-risk localised, 2033 readoutrecruiting Abi/Pred + ADT vs ADT in PSMA-Positive, Conventionally Node-Negative Prostate Cancer Phase 2n=140 · primary completion 2033-04 · abi added to ADT+RT in localised, 2033 readout
📚 Sources · 📄 1 paper
ENZARAD (ANZUP 1303)
ForHigh-risk clinically-localized/locally-advanced prostate, EBRT + 2yr ADT
8yr 74% vs 72%, HR 0.88
95% CI 0.67-1.15, p=0.34; 1° endpoint not met
TL;DRMFS 8yr 74% vs 72%, HR 0.88 (0.67-1.15) p=0.34; enza on an RT+ADT backbone missed 1° endpoint, benefit isolated to cN1/pelvic-RT.
Reported via UroToday →
The intensification benefit tracks the pelvic-RT-planned subgroup (MFS HR 0.47, OS HR 0.53), but that arm was enriched for cN1 (28% vs 0%), so nodal burden, not the RT field itself, likely drives it. Planning whole-pelvis RT for cN1 disease is where adding enzalutamide over 6mo NSAA earns its place; cN0 pts gained nothing.
8 details
Phase 3 open-label RCT, N=802 across 8 countries (2014-2018), median follow-up 8 years. Primary: metastasis-free survival (switched from OS mid-trial for fewer-than-expected deaths). Enzalutamide 160mg × 24mo vs conventional NSAA × 6mo, both on 24mo LHRH agonist + EBRT.
High-risk clinically-localized or locally-advanced prostate, EBRT-suitable. 90% Gleason 8-10, 36% PSA >20, 12% cN1 by conventional imaging. 40% planned pelvic RT, 8% brachytherapy boost.
Prostate to 78Gy, or 46Gy + brachy boost. Pelvic nodal RT 46Gy elective + boost to gross nodes, required for cN1, optional (pre-declared) for cN0. Intensive QA: credentialing, real-time review of first 5 plans per site, 20% sampling thereafter.
Primary MFS not met; PFS positive, OS neutral; benefit isolated to the cN1 and pelvic-RT-planned subgroups (see tables).
| Endpoint | Enza | Control | HR (95% CI), p |
|---|---|---|---|
| MFS (1°) | 74% | 72% | 0.88 (0.67-1.15), p=0.34 |
| PFS | 67% | 62% | 0.78 (0.61-0.99), p=0.044 |
| OS | 83% | 80% | 0.87 (0.63-1.20), p=0.40 |
| Subgroup | MFS HR (95% CI) | OS HR (95% CI) |
|---|---|---|
| cN1 nodal | 0.43 (0.20-0.92) | 0.46 (0.17-1.26) |
| Pelvic RT planned | 0.47 (0.29-0.76) | 0.53 (0.30-0.95) |
| Very high-risk | 0.85 (0.64-1.13) | 0.81 (0.57-1.13) |
| STAMPEDE | ENZARAD | |
|---|---|---|
| cN1 | 39% | 11% |
| Median PSA | 35 ng/ml | 14 ng/ml |
| cT3-4 | 92% | 47% |
| Overall MFS HR | 0.53 | 0.88 |
The cN1 MFS benefit mirrors STAMPEDE abiraterone; the weaker overall effect reflects ENZARAD's more favorable baseline risk (lower cN1 fraction, lower PSA, less cT3-4).
Active NSAA control (not placebo) narrows the measured enzalutamide effect. Subgroup benefits are prespecified but hypothesis-generating, and the pelvic-RT arm is confounded by nodal enrichment. Primary endpoint switched from OS to MFS mid-trial.
Phase 3, prespecified MFS primary, 8yr f/u, active-NSAA control; negative overall reinforces restrained intensification, cN1/pelvic-RT benefit mirrors STAMPEDE. Subgroups prespecified, not practice-defining alone.
In high-risk localized prostate with cN1 disease or planned pelvic-nodal RT, the data support enzalutamide intensification over 6mo NSAA; it does not extend to cN0 pts, who showed no MFS benefit.
- Which pelvic-RT subgroups drive the enzalutamide benefit
- Biomarkers to identify who needs treatment intensification
- Does nodal RT sterilization enable enzalutamide's distant-metastasis benefit
📚 Sources · 📄 1 paper
Abstract
REVELUTION
ForIntermediate/high-risk non-metastatic prostate on definitive RT + ADT
68.9 mm³ more plaque with leuprolide vs relugolix
Adjusted for age, statin, baseline plaque; crude 56 vs 25 mm³
TL;DR68.9 mm³ greater total coronary plaque progression with leuprolide vs relugolix at 12mo (adjusted), non-metastatic prostate on RT + ADT.
Reported via UroToday →
The signal is non-calcified plaque: leuprolide added 68.9 mm³ more total plaque than relugolix at 12mo (adjusted), and that gap tracked the non-calcified subtype, with no significant difference in calcified or low-attenuation plaque. For a radonc co-prescribing ADT with definitive RT, it strengthens the mechanistic case for relugolix in cardiovascular-risk pts.
8 details 3 trials watching
Single-institution, open-label, parallel-cohort randomized trial (4 Emory-affiliated centers, Jun 2020-2024). ADT-eligible pts randomized 1:1 relugolix vs leuprolide, stratified by ASCVD 10-yr risk; a lower-risk radiotherapy-alone cohort ran in parallel as a no-ADT control. N=94.
Non-metastatic intermediate/high-risk prostate cancer, all receiving pelvic RT (± pelvic nodes). ADT arms received ≥6 months hormone therapy; the control cohort was lower-risk, RT-alone, with no planned ADT.
Relugolix 360mg load then 120mg daily vs leuprolide 3-month depot. Serial coronary CTA at baseline and 12mo, blinded to arm, quantified by the HeartFlow automated tool.
Primary: 12-month change in total plaque volume. Secondary: non-calcified, calcified, and low-attenuation plaque subtypes.
Adjusted mean total-plaque difference 68.9 mm³ favoring relugolix; crude 12-mo change 56 vs 25 mm³ (leuprolide vs relugolix). Excess driven by non-calcified plaque; calcified and low-attenuation subtypes showed no significant difference.
Offers a coronary-atherosclerosis mechanism for HERO (2020), where relugolix showed lower MACE than leuprolide despite similar testosterone suppression and metabolic effects.
Surrogate imaging endpoint (plaque volume), not clinical MACE; small single-institution N=94, 12-month follow-up. Open-label, with a non-randomized RT-alone control cohort.
Small single-institution randomized trial, surrogate coronary-plaque imaging endpoint (not clinical MACE), 12-mo f/u; mechanistically supports HERO but doesn't independently establish clinical benefit.
In an intermediate or high-risk non-metastatic prostate pt getting definitive RT plus ADT with elevated cardiovascular risk, this supports favoring relugolix over leuprolide on a coronary-plaque basis; it does not extend to ADT-free lower-risk pts or to hard cardiovascular-event rates.
- Do plaque-volume differences translate to fewer clinical cardiovascular events? recruiting Effects of Relugolix vs Leuprolide on Cardiac Function in Patients With Prostate Cancer Phase 2n=70 · primary completion 2027-12 · phase 2 relugolix vs leuprolide cardiac function MRIrecruiting REVELUTION-2: Relugolix+Abiraterone Acetate (AA) Versus Leuprolide+AA Cardiac Trial Phase 3n=72 · primary completion 2029-07 · phase 3 relugolix vs leuprolide cardiac head-to-head
- Durability of plaque effect beyond 12 months recruiting REVELUTION-2: Relugolix+Abiraterone Acetate (AA) Versus Leuprolide+AA Cardiac Trial Phase 3n=72 · primary completion 2029-07 · up to 24-mo combination arm, cardiac readout to 2029
- Generalizability beyond single-institution N=94
📚 Sources · 📄 1 paper
Abstract
MROQC ADT Practice Patterns
ForHigh-risk M0/N0-1 prostate on definitive RT, GG4-5 predominant
TL;DRGuideline-concordant ADT (≥18mo) recommended in 67.0% of high-risk pts on definitive RT; ARPI intensification just 23.2% of STAMPEDE-eligible.
The RT prescriber's read is the adoption gap, not a treatment effect: even in a quality consortium, only 67.0% of high-risk pts on definitive RT are recommended ≥18mo ADT, and just 23.2% of STAMPEDE-eligible get ARPI intensification. Facility-level variability persists on multivariable analysis (P<.0001), so where a man is treated, not only his risk, sets his ADT. Prompts an audit of your own duration and intensification practice.
8 details
Prospective practice-pattern study within the Michigan Radiation Oncology Quality Consortium (MROQC), a statewide RT registry. 553 pts across 26 centers, Jun 2020–Nov 2024. Facility modeled as a random intercept (mixed-effects).
Intact, high-risk M0/N0-1 prostate cancer on definitive RT. GG4-5 75.0%, PSA ≥20 40.0%, cN1 19.9%, cT3/4 13.3%. 27.9% met STAMPEDE M0 intensification criteria.
Primary: intended guideline-concordant ADT (≥18mo). Also assessed: ARPI adoption before vs after STAMPEDE M0 publication, facility-level variability, and multivariable predictors of concordance.
91.3% recommended any ADT, 67.0% guideline-concordant. ARPI intensification among STAMPEDE-eligible rose 0% → 23.2% post-publication. Facility variability persisted on MVA (P<.0001).
| Factor | OR (GC-ADT) | 95% CI |
|---|---|---|
| cN1 | 2.94 | 1.44-5.99 |
| GG4 | 6.23 | 2.85-13.62 |
| GG5 | 9.45 | 4.46-20.06 |
| PSA ≥40 | 3.64 | 1.22-10.87 |
Benchmarks real practice against the 2022 AUA/ASTRO guideline (18-36mo ADT) and STAMPEDE M0 (ARPI for high-burden high-risk). Documents a persistent adoption gap, not a treatment effect.
Captures intended ADT duration and recommendations, not delivered therapy or adherence. Single-state consortium limits generalizability, and there is no efficacy or outcome endpoint.
Descriptive practice-pattern audit (no efficacy endpoint); reinforces AUA/ASTRO ADT guideline and STAMPEDE M0 as benchmark, documenting under-adoption rather than testing a new effect.
In high-risk men (GG4-5, cN1, PSA ≥40, or ≥2 STAMPEDE factors) starting definitive RT, this supports benchmarking ADT to ≥18mo and weighing ARPI intensification when STAMPEDE-eligible; it does not extend to low/intermediate-risk disease or ADT-omission decisions.
- Does intended guideline-concordant ADT translate to delivered treatment and adherence?
- What interventions reduce facility-level variability in ADT recommendations?
- Do Michigan consortium patterns generalize to national practice?
📚 Sources · 📄 1 paper
Abstract
DeLLphi-304
ForRelapsed SCLC with brain mets, >70% prior CNS-directed therapy
TL;DRIntracranial: time-to-CNS-progression HR 0.54 ITT; in brain-mets pts CNS PFS 6.5 vs 4.2mo (HR 0.40), CNS CR 15% vs 5% for tarlatamab.
The RT read is intracranial control without new radiation: brain-mets CNS PFS 6.5 vs 4.2mo (HR 0.40) and CNS CR 15% vs 5%. But >70% had prior CNS-directed therapy, so this is salvage intracranial activity, not a defer-brain-RT signal in RT-naive disease. Informs sequencing systemic ahead of repeat cranial RT.

| Arm | Median CNS PFS | HR (95% CI) |
|---|---|---|
| Tarlatamab (n=254) | NE (13.7-NE) | 0.54 (0.39-0.75) |
| Chemotherapy (n=255) | 7.2 mo (5.6-NE) | n/a |
+2 more figures

| Arm | Median CNS PFS | HR (95% CI) |
|---|---|---|
| Tarlatamab (n=67) | 6.5 mo (4.3-13.7) | 0.40 (0.24-0.66) |
| Chemotherapy (n=56) | 4.2 mo (2.9-5.5) | n/a |
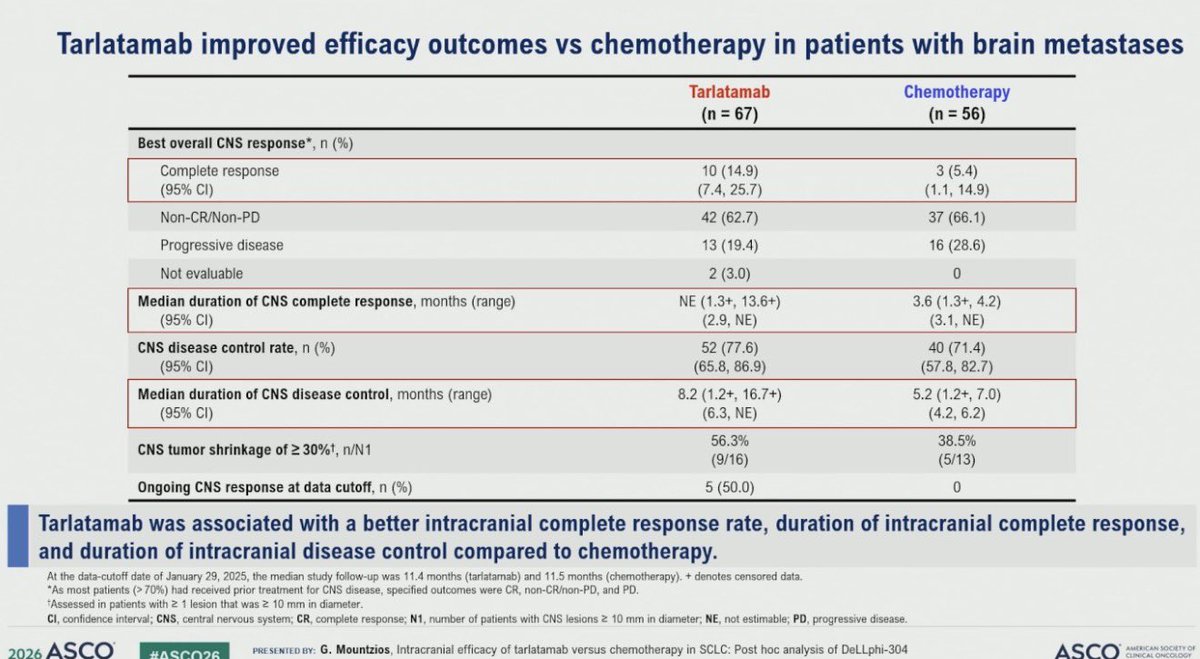
| CNS endpoint | Tarlatamab (n=67) | Chemotherapy (n=56) |
|---|---|---|
| Complete response | 10 (14.9%) | 3 (5.4%) |
| Disease control rate | 52 (77.6%) | 40 (71.4%) |
| Median duration CNS disease control | 8.2 mo | 5.2 mo |
5 details 2 trials watching
Post hoc intracranial analysis of DeLLphi-304, a phase 3 RCT of tarlatamab vs chemotherapy in relapsed SCLC. CNS endpoints were not prespecified primary. Data cutoff Jan 29 2025; median follow-up 11.4 mo (tarlatamab), 11.5 mo (chemo).
Relapsed SCLC. ITT CNS cohort n=254 tarlatamab vs 255 chemo; brain-mets subgroup n=67 vs 56. >70% of brain-mets pts had prior CNS-directed therapy.
Time to CNS progression or death (ITT, RECIST per investigator); brain-mets CNS PFS by mRANO-BM (BICR); best CNS response, CNS disease control rate, and response durations.
ITT time to CNS progression HR 0.54 (0.39-0.75), median NE vs 7.2 mo. Brain-mets CNS PFS and response detail in figures.
First DLL3xCD3 bispecific intracranial signal in SCLC; CNS control historically relied on WBRT/SRS and prophylactic cranial irradiation, not a systemic agent.
Post hoc, unstratified brain-mets HRs, small subgroup N. >70% prior CNS therapy confounds de novo intracranial activity. No new safety data in source.
Post hoc CNS analysis; brain-mets HRs unstratified with small N (67 vs 56), and >70% had prior CNS-directed therapy, confounding de novo intracranial activity.
For relapsed SCLC with previously-treated brain mets, this supports systemic intracranial control as an option before committing to repeat cranial RT; it does not inform RT-naive or symptomatic brain mets, where upfront local therapy still applies.
- Durability of intracranial response beyond current follow-up
- Activity in RT-naive or untreated brain metastases n=35 · primary completion 2029-02 · candidate match
- Sequencing tarlatamab vs cranial radiotherapy in SCLC brain mets n=39 · primary completion 2027-12 · candidate match
📚 Sources · 🐦 1 tweet
Dr. @g_mountzios #ASCO26 presents CNS outcomes with 2L tarlatamab in DeLLphi-304. Improved time to CNS progression overall (HR 0.54). In pts with brain nets, tarlatamab vs chemo CNS CR rate 15% vs 5% with DCR 78% vs 71% and time to CBS progression 6.5m vs 4.2m, HR 0.40 pic.twitter.com/5i8jL1zlKW
— Stephen V Liu, MD (@StephenVLiu) June 1, 2026
PROTEUS
TL;DRMost distant mets PSMA PET-detected (53.0% APA vs 60.7% control); preview NEJM data, MFS benefit's clinical meaning contested.
6 details 1 trial watching
Randomized, apalutamide + ADT vs ADT alone. Results just posted (NEJM online); full ASCO26 presentation pending, so this is a preview read.
Most distant metastases were PSMA PET-detected: 53.0% in the apalutamide group vs 60.7% in the control group. Primary MFS effect size not reported in source.
MFS events were predominantly PET-detected, raising lead-time / detection-bias concerns about the endpoint. The 50-vs-60 BCR/100 figures circulating are an illustrative hypothetical, not PROTEUS primary data.
Curator frames it as 'homerun vs largest negative' pending full data. A companion thought experiment argues PSMA PET vs conventional detection differences could account for much of the apparent metastasis delta.
Preview NEJM data; primary effect size not in source. Most MFS events PSMA PET-detected (53.0% vs 60.7%), raising lead-time/detection bias that undermines the MFS read.
- Does the MFS benefit hold on OS or conventional-imaging endpoints? n=1503 · primary completion 2026-06 · apalutamide MFS by conventional imaging (BICR)
- How much of the MFS delta reflects PSMA PET lead-time bias?
📚 Sources · 🐦 3 tweets
#ASCO26
— Daniel E Spratt (@DrSpratticus) May 31, 2026
The PROTEUS trial results are now online...buckle up as we wait to see the full presentation. This is going to be a trial that is likely highly controversial until the full results are published.
Some may call this a homerun, others may call this the largest negative…
Thought experiment:
— Sean McBride (@seanmmcbride) May 31, 2026
Let's take a very simple hypothetical trial involving 100 patients in the APA arm and 100 patients in the ADT alone arm. Pulling from PROTEUS EFS data, assume that, by 5 years, 60 patients in the ADT arm have had a BCR compared to 50 in the ADT+APA arm.… pic.twitter.com/WJaiDlJnQs
#ASCO26
— Daniel E Spratt (@DrSpratticus) May 31, 2026
Talk about real-time updates. NEJM paper now online and my predictions and inferences appear true.
Majority of MFS events were by PET not conventional imaging. "Most distant metastases were identified by PSMA PET (53.0% of those in the apalutamide group and 60.7% in the… https://t.co/Yz4myY0flq
RASolute 302
ForPreviously treated metastatic pancreatic cancer (RAS-mut or WT)
HR 0.40
95% CI 0.30-0.53, P<0.001; mOS 13.2 vs 6.7 mo (overall pop)
TL;DRmOS 13.2 vs 6.7mo, HR 0.40 (0.30-0.53), P<0.001 for daraxonrasib vs investigator's-choice chemo in previously treated metastatic pancreatic cancer.
In previously treated metastatic pancreatic cancer with a RAS mutation, daraxonrasib's OS benefit supports it as a systemic option over chemotherapy; the signal does not extend to treatment-naive or localized disease.

| Population · Arm | Median OS | HR (death) | 12-mo OS |
|---|---|---|---|
| G12 · Daraxonrasib | 13.2 mo (10.0-NR) | 0.40 (0.30-0.54) | 53.3% |
| G12 · Chemo | 6.6 mo (5.4-8.2) | — | 8.7% |
| Overall · Daraxonrasib | 13.2 mo (10.0-NR) | 0.40 (0.30-0.53) | 53.2% |
| Overall · Chemo | 6.7 mo (5.8-8.0) | — | 17.3% |
7 details 1 trial watching
Phase 3 RCT, daraxonrasib vs investigator's-choice chemotherapy in previously treated metastatic pancreatic cancer. Two prespecified populations: RAS G12-mutant and overall (G12/G13/Q61 or no RAS mutation identified).
Previously treated metastatic pancreatic cancer. RAS G12 arm n=228 vs 231; overall n=248 vs 252. Overall population also includes tumors with no identified RAS mutation.
Daraxonrasib, an oral RAS(ON) multi-selective inhibitor targeting active GTP-bound RAS, vs investigator's choice cytotoxic chemotherapy.
Primary OS met: median 13.2 vs 6.7 mo, HR 0.40 (0.30-0.53), P<0.001 (overall); HR 0.40 (0.30-0.54) in RAS G12. 12-mo OS 53% vs 17% (overall). Deaths 32% vs 55-56%.
Chemo control (6.6-6.7 mo) matches the historic 2L metastatic PDAC benchmark; no prior targeted agent has shown an OS signal of this magnitude in this setting.
Data limited to a single ASCO LBA OS figure; full safety and PFS not yet reported. Open-label; daraxonrasib median OS upper CI not reached (10.0-NR), so tail durability is immature.
Randomized phase 3, OS primary hit HR 0.40 in 2L metastatic PDAC where no targeted SOC exists; hard endpoint, unprecedented magnitude. Full LBA data pending.
- Sequencing and combination with 1L chemotherapy recruiting Study of Daraxonrasib and Daraxonrasib + GnP as First-line Treatment in Patients With Metastatic Pancreatic Adenocarcinoma Phase 3n=900 · primary completion 2028-06 · 1L daraxonrasib + gem/nab-paclitaxel combination
- Efficacy across RAS-WT vs RAS-mutant subsets
- Full safety and toxicity profile
📚 Sources · 🐦 1 tweet
#ASCO26
— Nicholas Hornstein (@GIMedOnc) May 31, 2026
This one is special.
This is the hottest paper of 2026 and potentially in the history of pancreatic cancer.
Let’s dive in.
RASolute 302: Daraxonrasib vs investigator’s choice chemotherapy in previously treated metastatic pancreatic cancer
Abstract LBA5 (soon!)… pic.twitter.com/Lq7PEjOWAo
A-DREAM
FormHSPC deep responder (PSA<0.2) after 18-24mo ADT + ≥12mo ARPI
TL;DR41% remained treatment-free with eugonadal testosterone recovery at 18mo after interrupting ADT+ARPI in deep-responding mHSPC (1° EP met, one-sided p=0.0249).
In metastatic HSPC deep responders (PSA<0.2 after ≥18mo ADT and ≥12mo ARPI, predominantly low-volume), this supports discussing a monitored ADT+ARPI holiday with scheduled PSA/imaging; it does not extend to incomplete responders or high-volume disease.

+2 more figures


8 details 4 trials watching
Phase 2 single-arm Alliance trial. N=78 eligible metastatic HSPC deep responders interrupt ADT+ARPI. Enrolled 07/2022-03/2024; median follow-up 26.9mo.
Entry required PSA<0.2 (stable/falling) after 18-24mo ADT and ≥12mo ARPI. Median age 70 (49-90); 64.9% low-volume, 35.1% high-volume (CHAARTED); 51.3% had prior local radiation, 29.5% metastasis-directed radiation.
Primary: treatment-free with eugonadal testosterone (≥150 ng/dL) at 18 months. Exploratory: rPFS, TTNT, OS, cost.
Primary met: 32/78 (41.0%) treatment-free and eugonadal at 18mo (80% CI 33.1-48.9%, one-sided p=0.0249). 57.7% were treatment-free at 18mo and 66.7% recovered testosterone; median time to eugonadal T 9.0mo.
Disease control held through interruption: rPFS 15/78 events, OS 4/78 events, both medians not reached. The 41% primary is capped by slow testosterone recovery, not progression, so the endpoint understates short-term oncologic safety in this older cohort.
Single-arm with no randomised comparator against continued therapy, so the survival cost of interruption is unquantified. Median follow-up 26.9mo is short for mHSPC; durability of treatment-free intervals is unproven.
Single-arm phase 2, N=78, no randomised comparator vs continued therapy; primary endpoint met but interruption safety needs longer follow-up and randomisation.
- Survival cost of interruption vs continued ADT+ARPI active A Study of an Intermittent ADT Approach With Apalutamide Monotherapy in Participants With mCSPC Phase 3n=420 · primary completion 2026-10 · intermittent post-response, rPFS non-inferiorityn=1600 · primary completion 2035-05 · phase 3 intermittent vs continuous, OS endpoint
- Durability of treatment-free interval beyond 27 months
- Which deep responders can safely interrupt active A Study of an Intermittent ADT Approach With Apalutamide Monotherapy in Participants With mCSPC Phase 3n=420 · primary completion 2026-10 · restricted to PSA <0.2 deep respondersrecruiting Optimal PSA Triggered Individual Management of Androgen Sensitive Prostate Cancer Phase 2n=160 · primary completion 2030-10 · intermittent ARPI in optimal PSA responders
📚 Sources · 🐦 1 tweet
Can treatment be safely stopped in selected patients with mHSPC?
— MJosé Juan (@mjuanfi81) May 30, 2026
Phase II A-DREAM trial, 41% of responders remained treatment-free with testosterone recovery 18m after stopping ADT/ARPI. At a median FU of 21 months, 35% of patients required treatment re-initiation.@OncoAlert pic.twitter.com/iW2VDBWWhN
ARACOG (AFT-47)
ForAdvanced prostate cancer (mHSPC/mCRPC/nmCRPC) starting an ARSI
TL;DRMCCD -36.1 (enza) vs -15.8 (daro), P=0.009 at 24 wk: enzalutamide worse for cognition; randomized open-label phase 2, N=111 advanced prostate.
In advanced prostate cancer pts where cognitive tolerability drives ARSI selection, this randomized head-to-head supports darolutamide over enzalutamide for cognitive sparing; it does not address efficacy or compare against apalutamide or abiraterone.

| Arm (N) | Max-changed domain | Median % change | P |
|---|---|---|---|
| Darolutamide (48) | PALFAM (visual mem/exec) | -15.8 | 0.009 |
| Enzalutamide (47) | SWM (working mem/exec) | -36.1 | n/a |
+1 more figure

7 details 2 trials watching
Randomized open-label phase 2, N=111, darolutamide vs enzalutamide, stratified by age (<65, 65-80, >80). US academic centers only; enrolled 8/2021 to 3/2025, crossover permitted.
Advanced prostate cancer across mHSPC, mCRPC, and nmCRPC. Required acceptable enzalutamide co-pay; predominantly White, with most non-White pts randomized to enzalutamide.
Darolutamide provided by the study vs enzalutamide through standard of care, an asymmetry that could bias crossover and adherence.
Primary: between-arm % change from baseline to 24 wk in Maximally Changed Cognitive Domain (MCCD), from 5 remotely delivered CANTAB tests. Crossovers scored at crossover in their randomized arm.
MCCD median change -36.1 (enza, N=47) vs -15.8 (daro, N=48), P=0.009: greater cognitive decline on enzalutamide.
First randomized head-to-head of cognition for these two ARSIs; direction fits darolutamide's minimal blood-brain-barrier penetration vs enzalutamide's CNS exposure.
Open-label with a functional endpoint; enzalutamide via standard of care may have altered crossover. CANTAB is a research tool, not a clinical diagnostic; small N and race-by-arm imbalance limit inference.
Randomized head-to-head met its prespecified cognitive endpoint; aligns with darolutamide's known low CNS penetration. Phase 2, open-label, small N keep it below practice-changing.
- Does the cognitive advantage translate to functional outcomes or efficacy? n=102 · primary completion 2026-04 · tracks functional status + cognition on ARPIs
- Darolutamide vs apalutamide or abiraterone on cognition? n=102 · primary completion 2026-04 · cognitive outcomes across daro/apa/abi ARPIs
- Durability of the cognitive difference beyond 24 weeks
📚 Sources · 🐦 2 tweets
ARACOG (AFT-47) met its primary endpoint: enzalutamide caused significantly greater cognitive decline than darolutamide at 24 weeks in advanced prostate cancer.
— Katy Beckermann (@katy_beckermann) May 30, 2026
Randomized open-label phase 2, 111 pts (mHSPC, mCRPC, nmCRPC), DAR vs ENZ.
Cognition was measured with CANTAB, a… pic.twitter.com/kj4vfGRVyp
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 Abstract 5005 | ARACOG / AFT-47
Cognitive effects of darolutamide vs enzalutamide
Presented by Alicia K. Morgans, MD, MPH, FASCO@CaPsurvivorship @OncoAlert@ASCO
In prostate cancer, we often discuss AR pathway inhibitors through the lens… pic.twitter.com/vpZr1w6kc6
ENZAMET + Decipher (Part 2)
FormHSPC on ADT + enzalutamide, Decipher genomic classifier available
TL;DRDecipher >0.85 predicts docetaxel OS benefit on an ADT+enza backbone (HR 0.75 vs 1.94, interaction p=0.04); ≤0.85 can skip docetaxel.
In mHSPC starting ADT + enzalutamide, a Decipher score >0.85 is where the docetaxel OS benefit concentrates while ≤0.85 sees little added benefit; the read informs docetaxel selection, not any radiotherapy decision.

| Treatment arm | Decipher >0.85 vs ≤0.85 OS HR | p |
|---|---|---|
| ADT + ENZA | 3.02 (1.50-5.76) | — |
| ADT + ENZA + Doce | 1.08 (0.60-1.71) | 0.73 |
+1 more figure

| Decipher stratum | Unweighted HR (doce vs none) | IPTW-weighted HR |
|---|---|---|
| ≤0.85 | 2.78 (1.49-5.21) | 1.94 (0.95-3.96) |
| >0.85 | 1.13 (0.71-1.79) | 0.75 (0.43-1.33) |
7 details
Preplanned biomarker analysis of the phase 3 ENZAMET RCT. Decipher genomic classifier (DPMC, cutpoint >0.85) applied to the ADT + enzalutamide backbone cohort, N=320.
Metastatic hormone-sensitive prostate cancer on an ADT + enzalutamide backbone with an available Decipher score. A low-volume subset was analysed separately.
ADT + enzalutamide ± early docetaxel. Docetaxel was given at investigator discretion (a stratification factor), so the docetaxel comparison is not randomised.
Two-part signal: Decipher >0.85 is prognostic for worse OS on ADT+enza, and by IPTW interaction (p=0.04) predicts OS benefit from added docetaxel; ≤0.85 derives little benefit. Effect sizes in the figures.
Consistent with docetaxel OS benefit in CHARTED and STAMPEDE for high-volume/high-risk mHSPC; positions Decipher as a molecular refinement of that selection. Presented as Level 1B evidence.
Docetaxel not randomised (IPTW-weighted, residual imbalance after scoring); the high-Decipher benefit's CI crosses 1 and rests on a subgroup interaction. Hypothesis-generating, not yet practice-defining.
Post-hoc biomarker-by-docetaxel interaction; docetaxel not randomised (IPTW-weighted, residual imbalance acknowledged). High-Decipher benefit CI crosses 1, rests on interaction p=0.04, strengthened only after weighting.
- Prospective validation of Decipher-guided docetaxel selection in mHSPC
- Whether DPMC ≤0.85 pts can safely omit docetaxel
- Decipher predictive value across other intensification agents (ARSI, PARP)
📚 Sources · 🐦 1 tweet
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 ENZAMET + Decipher | Part 2
Can genomics guide docetaxel intensification in mHSPC?
Outstanding presentation by @ChrisSweeney1.@OncoAlert@ASCO
After Part 1, the key question was:
➡️ Can a genomic classifier identify which patients with… pic.twitter.com/nJYMxuXelV
TALAPRO-3
ForHRR-deficient metastatic prostate cancer
HR 0.48
95% CI 0.36-0.65, P<0.001; 3yr rPFS 77% vs 56% (ITT)
TL;DR3yr rPFS 77% vs 56%, HR 0.48 (0.36-0.65), adding talazoparib to enzalutamide/ADT in HRR-deficient metastatic prostate cancer.
In HRR-deficient metastatic prostate cancer, this supports intensifying enzalutamide/ADT with talazoparib, benefit steepest in the BRCA subgroup; it does not extend to HRR-intact disease.

| Population | HR (95% CI) | Median rPFS, mo |
|---|---|---|
| ITT | 0.48 (0.36-0.65) | NC vs 45.8 |
| BRCA | 0.37 (0.22-0.61) | NC vs 35.1 |
| Non-BRCA | 0.57 (0.39-0.82) | NC vs NC |
6 details 2 trials watching
Randomized, placebo-controlled trial: talazoparib+enzalutamide vs placebo+enzalutamide, 300 vs 299 pts. Published NEJM May 30, 2026.
HRR-deficient metastatic prostate cancer, enzalutamide/ADT backbone both arms. Prespecified BRCA (104/103) and non-BRCA HRR (196/196) strata.
Talazoparib (PARP inhibitor) added to enzalutamide plus ADT; control substituted placebo for talazoparib on the same ARSI backbone.
Primary: imaging-based (radiographic) PFS. OS and other secondaries not reported in source.
ITT 3yr rPFS 77% vs 56%, P<0.001; per-population HRs and medians in the figure. Benefit concentrated in the BRCA subgroup.
Extends PARP+ARSI combinations (TALAPRO-2, PROpel, MAGNITUDE) that established the class in HRR-altered mCRPC toward the enzalutamide/ADT-backbone metastatic setting.
Primary endpoint is rPFS, a surrogate; OS not reported in source. Non-BRCA benefit is modest, so the HRR-wide result leans on BRCA. Talazoparib medians not reached, so follow-up is immature.
Randomized phase 3, rPFS primary hit (HR 0.48); but rPFS is a surrogate and OS not reported. Aligns with PARP+ARSI direction (TALAPRO-2, PROpel, MAGNITUDE).
- Overall survival benefit, given rPFS is the surrogate primary endpoint n=1054 · primary completion 2022-10 · mature phase 3, same combo vs enza, mCRPC
- Whether non-BRCA HRR alterations derive benefit comparable to BRCA recruiting A Study of Talazoparib With or Without Enzalutamide in People With Prostate Cancer Who Have Previously Received Abiraterone Acetate Phase 2n=126 · primary completion 2029-03 · talazoparib in broad HRR-mutant mCRPC
📚 Sources · 🐦 1 tweet
JUST In: TALAPRO-3 published in @NEJM
— Toni Choueiri, MD (@DrChoueiri) May 30, 2026
Adding #talazoparib to enzalutamide/ADT
=>3-year rPFS: 77% vs 56% in HRR-deficient metastatic prostate cancer !
Looking forward to full presentation by @neerajaiims who keeps changing SOC, one trial at a time. @ASCO #ASCO26 @OncoAlert pic.twitter.com/nXiPk4DIXg
CHRYSALIS-2
ForTreatment-naïve atypical EGFR-mutant advanced NSCLC
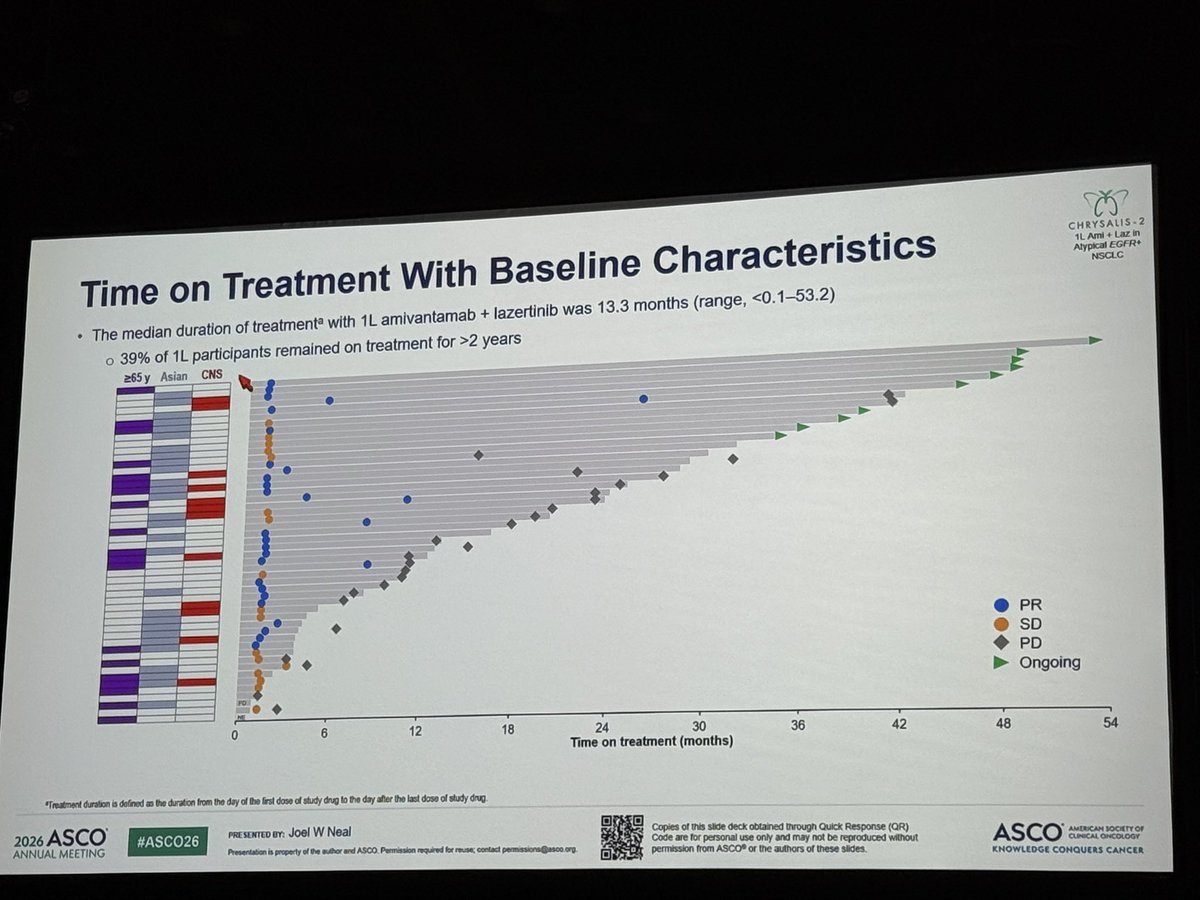
TL;DRmOS 41.0 mo (95% CI 27.7-NE) with 1L amivantamab + lazertinib in treatment-naïve atypical EGFR-mutant NSCLC; single-arm, n=49.
In treatment-naïve atypical EGFR-mutant advanced NSCLC, a population with few standard targeted options, this single-arm 41-mo median OS supports amivantamab+lazertinib as a candidate 1L regimen; it does not extend to common EGFR (exon19del/L858R) disease, where randomised data already guide practice.

+1 more figure
8 details
Single-arm cohort, n=49, no randomised comparator. Median follow-up 31.3 mo.
Treatment-naïve (1L) atypical EGFR-mutated advanced NSCLC. Responses durable regardless of demographics, baseline mutations, and disease characteristics.
IV amivantamab + lazertinib. Median treatment duration 13.3 mo (range <0.1-53.2); 39% on treatment >2 years.
Median OS 41.0 mo (95% CI 27.7-NE), ~3.5 years. No clear association between EGFR variant subtype and OS.
With longer follow-up, safety consistent with prior reports; no new safety signals.
Extends the durable 1L amivantamab+lazertinib OS signal from common EGFR (exon19del/L858R) to atypical variants.
Single-arm, n=49, no randomised comparator. Atypical EGFR is a heterogeneous class; per-variant efficacy not detailed in source.
Single-arm cohort (n=49), no randomised comparator in atypical EGFR NSCLC; durable but single-arm design caps the read at early-signal despite 31-mo follow-up.
- Efficacy by specific atypical EGFR variant
- Randomised comparison vs other 1L options in atypical EGFR
📚 Sources · 🐦 1 tweet
Amivantamab + lazertinib achieved a median OS of 41.0 months in treatment-naïve atypical EGFR-mutant NSCLC, with no clear association between EGFR variant subtype and outcome. A compelling option. Meanwhile, amivantamab continues evaluation across multiple tumor types. #ASCO26 pic.twitter.com/aWn3Ja60Ji
— Chul Kim (@chulkimMD) May 29, 2026
ESAONA
ForTreatment-naive EGFR-mutant NSCLC with brain metastases
TL;DRiORR 95.5% vs 79.6% (p=0.0004) and icPFS HR 0.46 favoring asandeutertinib over osimertinib in 1L EGFR-mut NSCLC brain mets.
The RT-relevant read is upfront local therapy: iORR 95.5% vs 79.6% and intracranial PFS not reached (HR 0.46) strengthen deferring upfront SRS/WBRT in favor of TKI in EGFR-mut brain mets. No head-to-head vs radiosurgery, so it moves sequencing, not RT omission at progression.
7 details 5 trials watching
Randomised phase 2, N=224 (111 asandeutertinib vs 113 osimertinib), 1L EGFR-mutant NSCLC with brain metastases. All efficacy endpoints BICR-assessed. Blinding not specified in source.
Treatment-naive (1L) EGFR-mutant NSCLC with brain metastases. Mutation subtype, symptomatic status, and prior brain RT not reported in source.
Asandeutertinib (next-generation EGFR TKI) vs osimertinib. Dose and schedule not reported in source.
Intracranial endpoints (response, icPFS) drove the result and cleared significance more decisively than the borderline overall PFS benefit. Full arm comparison in the table above.
| Endpoint | Asandeutertinib | Osimertinib | HR (p) |
|---|---|---|---|
| iORR | 95.5% (89.8-98.5) | 79.6% (71.0-86.6) | p=0.0004 |
| Intracranial PFS | NR | 17.5 mo (15.18-NA) | HR 0.46, p=0.0020 |
| Overall PFS | NR | 17.2 mo (15.18-19.55) | HR 0.64, p=0.0473 |
Any TRAEs 99.1% vs 95.6%; serious TRAEs numerically higher with asandeutertinib (10.8% vs 7.1%). Fatal and discontinuation rates not reported in source.
Osimertinib is the established CNS-active 1L EGFR TKI (FLAURA). Asandeutertinib raises the intracranial bar in phase 2, but no OS or phase 3 head-to-head yet.
Phase 2 with immature time-to-event data (medians not reached); overall PFS benefit borderline (p=0.0473); no OS; blinding not specified.
Strong intracranial activity revives whether a CNS-active TKI can defer upfront brain-directed RT/SRS in EGFR-mutant NSCLC. Phase 3 confirmation vs osimertinib, plus OS and durability, is needed before displacing the standard.
Randomised phase 2; strong intracranial ORR but time-to-event immature (medians NR), overall PFS borderline (p=0.0473), no OS. Needs phase 3 before displacing osimertinib.
In treatment-naive EGFR-mutant NSCLC with brain metastases, this supports a TKI-first, SRS-deferred read; it does not extend to EGFR-wildtype disease or brain mets progressing on a prior EGFR TKI.
- Overall survival vs osimertinib recruiting TY-9591 in the Patients With EGFR Mutations in Advanced NSCLC With Brain Metastases Phase 2n=420 · primary completion 2025-06 · 1L TY-9591 vs osimertinib, EGFR brain metsn=380 · primary completion 2029-03 · phase 3 furmonertinib vs osimertinib in brain mets
- Durability of intracranial response with longer follow-up
- Head-to-head efficacy vs upfront radiosurgery n=162 · primary completion 2024-12 · osimertinib +/- early SRS, asymptomatic BMactive Study of Osimertinib + SRS vs Osimertinib Alone for Brain Metastases in EGFR Positive Patients With NSCLC Phase 2n=40 · primary completion 2025-04 · randomized osimertinib +/- upfront SRS, 1Lrecruiting Observation or Upfront Cranial RT in Oncogene Mutated NSCLC With Asymptomatic BM: A Phase III RCT Phase 3n=190 · primary completion 2025-12 · phase 3 upfront cranial RT vs obs on TKI
📚 Sources · 🐦 1 tweet
#ASCO26 🧠🌍
— Dr Rishabh Jain (@DrRishabhOnco) May 30, 2026
Could a next-generation EGFR TKI outperform osimertinib in patients with brain metastases?
The phase II ESAONA trial suggests the answer may be yes.
🧪 LBA2007 | ESAONA
1L EGFR-mutated NSCLC with brain metastases
👥 n=224
⚔️ Asandeutertinib vs Osimertinib
Key… https://t.co/mEOKGNKgf7 pic.twitter.com/pUQuH6i2cV
OptiTROP-Lung05 NCT06448312
For1L IIIB/IIIC-IV PD-L1≥1% NSCLC, EGFR/ALK wild-type
HR 0.35
95% CI 0.26-0.47, p<0.0001; median NR vs 5.7 mo
TL;DRmPFS NR vs 5.7 mo, HR 0.35, adding Sac-TMT (TROP2 ADC) to pembrolizumab in 1L PD-L1+ NSCLC.

| Arm | PFS events n (%) | Median PFS | HR (95% CI) |
|---|---|---|---|
| Sac-TMT+Pembro | 66 (31.7%) | NR (13.6-NE) | 0.35 (0.26-0.47) |
| Pembro | 128 (62.4%) | 5.7 mo (4.3-7.0) | — |
+2 more figures

| PD-L1 TPS | mPFS combo | mPFS pembro | HR (95% CI) |
|---|---|---|---|
| ≥50% | NR | 9.5 mo | 0.47 (0.29-0.77) |
| 1-49% | NR | 4.3 mo | 0.28 (0.19-0.41) |

| Arm | OS events n (%) | Median OS | HR (95% CI) |
|---|---|---|---|
| Sac-TMT+Pembro | 33 (15.9%) | NR | 0.55 (0.36-0.85) |
| Pembro | 54 (26.3%) | NR | — |
8 details 2 trials watching
Phase 3, open-label, multicenter RCT (NCT06448312); 1:1, N=413. Primary PFS by BICR crossed its interim efficacy boundary at 194 events; median follow-up 10.5 mo.
1L stage IIIB/IIIC or IV NSCLC, PD-L1 TPS ≥1% (22C3), EGFR/ALK wild-type, ECOG 0-1. Stratified by histology, PD-L1 (1-49 vs ≥50), ECOG.
Sac-TMT (TROP2 ADC) 4 mg/kg Q2W + pembrolizumab 400 mg Q6W vs pembrolizumab alone; pembro capped at 18 cycles.
ORR 70.2% vs 42.0%. PFS gain held across PD-L1 strata, strongest in TPS 1-49% where pembro monotherapy is weakest. OS immature, formal testing pending.
Current 1L PD-L1+ NSCLC standard is pembrolizumab ± chemotherapy. This tests a chemo-free ADC+IO doublet; no head-to-head vs chemo-IO.
Open-label; OS immature at 10.5-mo follow-up and formally untested; PFS reported at an interim efficacy boundary. No safety data in source.
PFS crossed an interim efficacy boundary; key-secondary OS descriptive/immature at 10.5-mo f/u; open-label. Strong but not yet mature enough to move 1L SOC.
- Will the OS benefit mature and hold? n=30 · primary completion 2026-06 · candidate match
- How does the chemo-free ADC+IO doublet compare to chemo+IO? n=30 · primary completion 2026-06 · candidate match
- Safety of adding a TROP2 ADC to pembrolizumab
📚 Sources · 🐦 2 tweets
🔁REVIEW #ASCO26 #LCSM Oral
— Hidehito HORINOUCHI (@HHorinouchi) May 30, 2026
🔥OptiTROP-Lung05: 1L Sac-TMT + Pembro vs Pembro in PD-L1+ NSCLC
✅mPFS NR vs 5.7m (HR 0.35)
✅ORR 70.2% vs 42.0%
✅OS HR 0.55 (95%CI 0.36-0.85, immature)
🎙️Dr. Caicun Zhou
🔗 https://t.co/DcbK1dGrhO@OncoAlert @Larvol @ASCO @IASLC https://t.co/512k6dZviW pic.twitter.com/Vdo86N50h9
Right patient. Right treatment. Right timing.
— Yakup Ergün (@dr_yakupergun) May 30, 2026
The result: curves like these👇#ASCO26 https://t.co/72KByLKz90
NRG/RTOG 9804 + E5194 Combined Analysis
ForGood-risk DCIS (low/int grade, ≤2.5cm, ≥3mm margins), lumpectomy without RT
TL;DR15-yr IBR 11.4% vs 19.0% with vs without tamoxifen in RT-omitted good-risk DCIS; MVA HR 0.54, invasive-IBR HR 0.43.
Tamoxifen's benefit here concentrates on invasive IBR (HR 0.43, p=0.0042), not DCIS-IBR (p=0.089), offsetting the recurrences that carry survival weight. But 15-yr IBR stays 11.4% even with tamoxifen, and no arm tests RT, so this informs the omit-RT-plus-endocrine path, not RT vs tamoxifen.
7 details 4 trials watching
Ancillary exploratory analysis pooling the non-RT arm of NRG/RTOG 9804 with the good-risk cohort of ECOG-ACRIN E5194. N=878 (317 + 561), median follow-up 14.85 yr.
Good-risk DCIS: low or intermediate grade, ≤2.5 cm, margins ≥3 mm, lumpectomy without RT. Median age 59. Tamoxifen users skewed toward negative re-excision and pathologic size ≤5 mm.
Tamoxifen optional and non-randomized, used by 43.1% overall (65.6% in 9804, 30.3% in E5194).
No RT in either cohort by design; this characterizes the RT-omitted good-risk population, not an RT comparison.
IBR overall, invasive IBR, DCIS-IBR, contralateral breast event, OS. Fine-Gray competing-risk models, univariate plus multivariable.
NSABP B-24 randomized tamoxifen after lumpectomy plus RT and cut breast events; this extends the tamoxifen signal to the RT-omitted good-risk setting, though non-randomized.
Tamoxifen not randomized; users differed on prognostic factors (re-excision, size), so residual confounding is likely. Exploratory combined dataset, not a prespecified endpoint.
| Endpoint | HR (95% CI) | p |
|---|---|---|
| Any IBR | 0.54 (0.35-0.83) | 0.0045 |
| Invasive IBR | 0.43 (0.24-0.77) | 0.0042 |
| Group | 15-yr IBR (95% CI) |
|---|---|
| Tamoxifen | 11.4% (7.9-15.5) |
| No tamoxifen | 19.0% (15.3-22.9) |
Non-randomized optional tamoxifen compared within a post-hoc combined dataset; users differed on prognostic factors. Consistent with randomized NSABP B-24 signal but confounded here.
For good-risk DCIS where RT is already being omitted, this supports endocrine therapy to reduce invasive IBR; it does not test whether tamoxifen substitutes for RT.
- Whether endocrine therapy can substitute for RT in good-risk DCIS not yet Assessment of Biosignature Classification of DCIS for RadioTherapy Benefit Post Lumpectomy (ABCD RT) Phase 3n=5270 · primary completion 2039-07 · phase 3 RT omission in biosignature-low DCIS
- Aromatase inhibitor vs tamoxifen in RT-omitted good-risk DCIS recruiting DCIS: RECAST Trial Ductal Carcinoma In Situ: Re-Evaluating Conditions for Active Surveillance Suitability as Treatment Phase 2n=400 · primary completion 2028-11 · DCIS trial with tamoxifen vs AI arms
- Which good-risk DCIS pts can omit both RT and endocrine therapy active Comparing an Operation to Monitoring, With or Without Endocrine Therapy (COMET) Trial For Low Risk DCIS Phase NAn=997 · primary completion 2024-06 · active monitoring vs surgery, low-risk DCISn=2500 · primary completion 2034-02 · active surveillance vs standard, low-risk DCIS