Bladder
MIBC bladder-preservation thread: durvalumab added to 55Gy/20fx chemoRT (RAD-IO) plus post-pCR perioperative management.
RAD-IO
ForT2-T4a N0M0 muscle-invasive urothelial bladder cancer
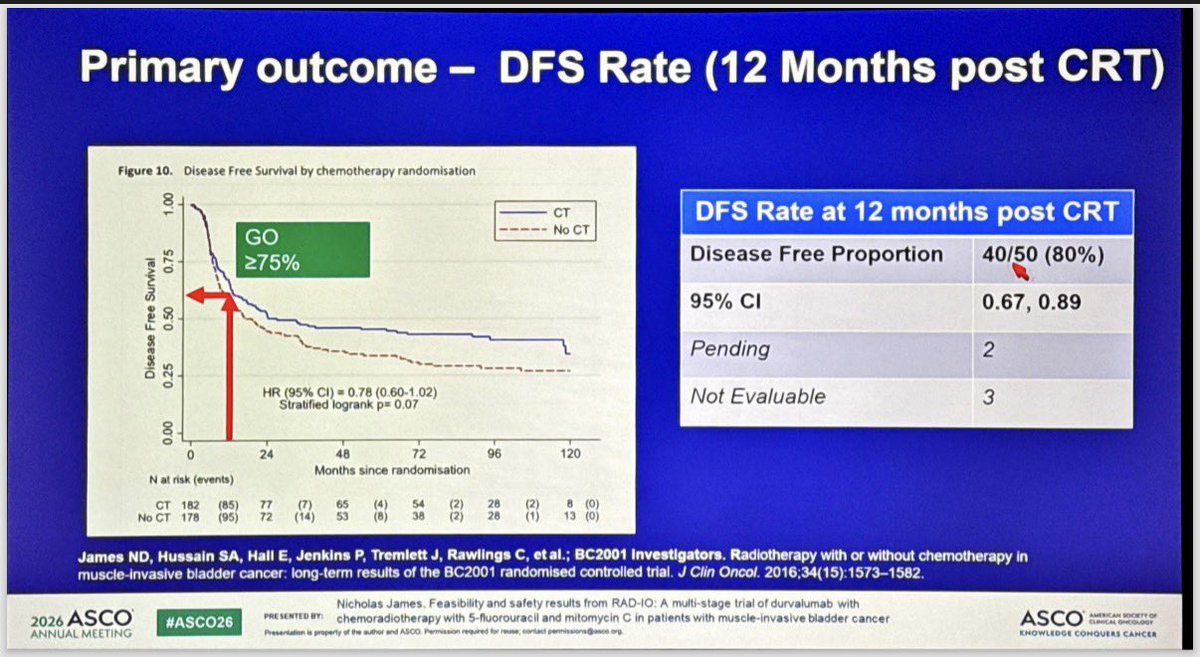
TL;DR12-mo DFS 40/50 (80%, 95% CI 0.67-0.89) cleared the pre-set ≥75% GO bar for durvalumab added to 5FU/MMC chemoRT in MIBC.
RT is standard and transferable: 55Gy/20fx to bladder, plus 46Gy/20fx elective nodal coverage in the node-positive expansion, extending durvalumab-chemoRT preservation to N+ disease. 12-mo DFS 80% (40/50, 95% CI 0.67-0.89) cleared the pre-set ≥75% GO bar vs BC2001. Moves whether to layer IO onto a hypofractionated preservation backbone.
+1 more figure

8 details 4 trials watching
Single-arm, multi-stage feasibility and safety trial testing durvalumab added to 5FU/MMC chemoradiation for bladder preservation. Benchmarked against BC2001 historical CRT data, not a randomised comparator.
T2-T4a N0M0 urothelial muscle-invasive bladder cancer, stratified by prior neoadjuvant chemotherapy (yes vs no). A stage-1 expansion added the first 6 node-positive pts.
Durvalumab 1500 mg given neoadjuvant, synchronous, and adjuvant to 12 months post-chemoRT. Concurrent 5-FU 500 mg/m²/24h ×5 days and mitomycin C 12 mg/m².
55 Gy in 20 fractions to bladder (hypofractionated). Node-positive expansion added 46 Gy/20 fx elective nodal RT.
Primary: 12-month disease-free survival post-chemoRT, read against a GO/NO-GO framework (GO ≥75%, contextual 60-75%, NO-GO <60%).
12-mo DFS 40/50 (80%), 95% CI 0.67-0.89, clearing the ≥75% GO bar. 33/54 (61%) completed planned durvalumab; investigators reported very high bladder-preservation and DFS vs prior trial data.
AEs reported in line with component therapies (chemoRT plus durvalumab). 21/54 (39%) discontinued durvalumab early.
Benchmarked against BC2001 (James, JCO 2016), where adding 5FU/MMC to RT gave DFS HR 0.78 (0.60-1.02), p=0.07. RAD-IO's 80% 12-mo DFS is claimed higher than prior data, but the comparison is non-randomised.
Single-arm with a historical benchmark and no concurrent IO comparator; 12-mo DFS is an early surrogate; small N (~50 evaluable); node-positive experience limited to 6 pts.
Single-arm feasibility stage, no randomised IO comparator; benchmarked against historical BC2001. 12-mo DFS an early surrogate at small N; met pre-set GO bar for further evaluation only.
In T2-T4a N0M0 MIBC opting for bladder preservation, this supports durvalumab layered onto 5FU/MMC chemoRT as worth further evaluation; it does not yet establish that IO improves on chemoRT alone, and node-positive experience rests on only 6 expansion pts.
- Does durvalumab add over chemoRT alone in a randomised trial n=11 · primary completion 2026-02 · randomised chemoRT ± durvalumab in node+ MIBC
- Durability of bladder preservation and DFS beyond 12 months active Treating Muscle-invasive Bladder Cancer With A Non-surgical Method Consisting of Anti-PD-1 Therapy and Chemoradiation Phase 2n=71 · primary completion 2025-12 · IO+chemoRT bladder preservation, phase 2recruiting Enfortumab Vedotin in Combination With Pembrolizumab vs. Concurrent Chemoradiotherapy (cCRT) in People With Muscle Invasive Bladder Cancer (EV-309) Phase 3n=390 · primary completion 2030-03 · phase 3 EV+pembro vs cCRT bladder preservation
- Efficacy in node-positive MIBC beyond the 6-patient expansion n=11 · primary completion 2026-02 · durvalumab+chemoRT in node-positive bladder ca
📚 Sources · 🐦 3 tweets
RAD-IO: chemoradiation (5FU+MMC) + Durva in MIBC. #ASCO26 pic.twitter.com/yTyhkdjCox
— Álvaro Pinto (@dralvaropinto) May 30, 2026
#ASCO26 🔬 Abstract 4504 | RAD-IO
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
Durvalumab + chemoradiotherapy in muscle-invasive bladder cancer
Presented by Nicholas D. James, PhD, MBBS, FRCP@OncoAlert@ASCO
Bladder preservation in MIBC remains one of the most important curative-intent questions in GU oncology.
The key… pic.twitter.com/W6JqzTVsJ3
RAD-IO at #ASCO26: durvalumab added to chemoradiation in muscle-invasive bladder cancer cleared its efficacy bar in a bladder-preservation approach. Single-arm, benchmarked against prior CRT data.
— Katy Beckermann (@katy_beckermann) May 30, 2026
Durvalumab given before, during, and 12 months after chemoRT (55Gy/20Fr +… pic.twitter.com/UXxwoZzaMC
Management of MIBC After Pathologic Complete Response
TL;DRReview of perioperative MIBC management after pCR: sandwich IO regimens continue adjuvant regardless of response, cisplatin-chemo alone moves to surveillance.
SWOG 8710ABACUSCHECKMATE-274KEYNOTE-905VOLGANIAGARAVESPERKEYNOTE-B15
8 details 3 trials watching
- 🔍 pCR used as primary endpoint in signal-seeking phase 2 trials
- 🔍 pCR co-primary (not standalone) endpoint in phase 3 registrational trials
- 🔍 High-risk residual disease (≥ypT2 or N+) post-neoadjuvant chemo → adjuvant therapy (CHECKMATE-274)
- 💊 Post-pCR management by regimen
- Sandwich IO (NIAGARA, EVP): continue planned adjuvant regardless of pathologic response
- NIAGARA: resume durvalumab 8 mo post-cystectomy
- Cisplatin-based chemo alone: surveillance after pCR is standard
- 📊 pCR (pT0N0) post-neoadjuvant chemo = strong prognostic marker: SWOG 8710 85% 5-yr OS if pT0
- 📐 Meta-analysis: pooled RR 0.19 for RFS with pCR
- 📊 Perioperative regimens across trials
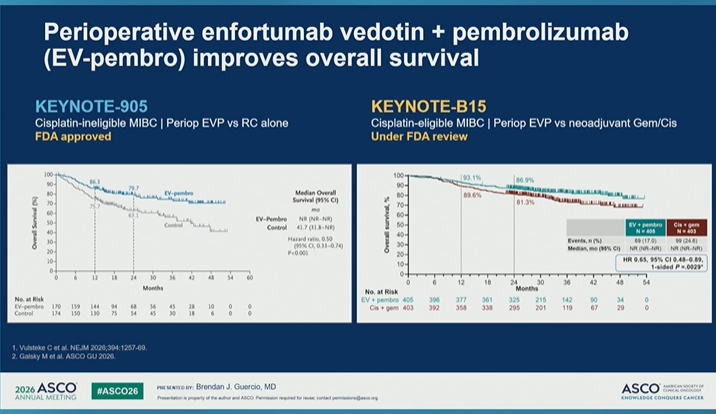
Trial Setting Comparison Result NIAGARA Cis-eligible Gem/Cis + periop durvalumab 24-mo OS 82.2% vs 75.2% VESPER Cis-eligible ddMVAC vs Gem/Cis 5-yr OS 66% vs 57% KEYNOTE-905 Cis-ineligible Periop EVP vs cystectomy alone OS HR 0.50 KEYNOTE-B15 Cis-eligible Periop EVP vs Gem/Cis OS improved (under FDA review)
- ⚠️ Not all pts in perioperative trials completed adjuvant therapy, often due to toxicity
- Relative contribution of pre- vs post-operative therapy components
- Can adjuvant therapy be de-escalated by pCR or biomarker n=761 · primary completion 2025-06 · adjuvant atezo gated by ctDNA+ post-cystectomyrecruiting Surveillance of the Genetic Signature in Circulating Tumor DNA for Guiding Adjuvant Chemotherapy in Urothelial Carcinoma Phase 2n=20 · primary completion 2025-09 · ctDNA-guided adjuvant gem/cis in urothelialn=992 · primary completion 2030-09 · ctDNA-guided adjuvant IO after cystectomy
📚 Sources · 🐦 1 tweet
#ASCO26 GU Oncology Spotlight 🚨
— Dra. María Natalia Gandur Quiroga (@nataliagandur) May 30, 2026
🔬 Management in Bladder Cancer After Pathologic Complete Disease Response
Presented by Brendan J. Guercio, MD@OncoAlert@ASCO
In muscle-invasive bladder cancer, pCR after neoadjuvant therapy is one of the most powerful prognostic signals we… pic.twitter.com/sMd2In7X3p