Challenges SOC
TREASURE NCT04462276
ForES-SCLC, ≥stable disease after chemo-IO induction; unselected
6.7 vs 13.4 mo
HR 1.55 (95% CI 0.90-2.69), P=.34; TRT arm worse, ns
TL;DRmOS 6.7 vs 13.4mo (HR 1.55, ns) adding consolidative TRT to atezo maintenance; halted early for SAEs 61% vs 18%.
The harm, not the null OS, is the RT read: SAEs 61% vs 18%, fatal AEs 19% vs 3%, driven by post-TRT lymphocyte depletion and low baseline DLCO in the fatal cases. 30Gy/10fx consolidative TRT on atezo maintenance is net harmful in unselected ES-SCLC; any future use needs lung-function gating.
6 details 1 trial watching
Phase 2 open-label RCT (AIO-TRK-0320), 1:1, 20 sites in Germany/Austria. Planned 104 pts; halted early by the SMC after 68 randomized (34/arm) for excess fatal SAEs in the TRT arm. Recruited 2020-2022, last follow-up Sept 2024, post-hoc survival update April 2026.
ES-SCLC with at least stable disease after induction carboplatin-etoposide-atezolizumab. Baseline well balanced between arms and between pts with vs without SAEs. Unselected for lung function.
Consolidative TRT 30 Gy in 10 fractions added to atezolizumab maintenance (arm A) vs atezolizumab maintenance alone (arm B).
Primary: overall survival. Secondary included PFS and safety.
Primary OS not met: the TRT arm was numerically worse with no PFS difference and sharply higher serious and fatal toxicity (see table).
| Endpoint | +TRT (arm A) | Atezo alone (arm B) | Effect |
|---|---|---|---|
| mOS | 6.7 mo (5.1-9.0) | 13.4 mo (10.7-17.5) | HR 1.55 (0.90-2.69), P=.34 |
| mPFS | 2.4 mo (1.3-3.9) | 2.6 mo (1.2-3.9) | HR 0.92 (0.54-1.55), P=.85 |
| SAEs | 61.3% | 18.2% | P<.001 |
| Fatal AEs | 19.4% | 3.0% | P=.04 |
SAEs dominated by infection and respiratory disorders, linked to radiation-induced lymphocyte depletion; fatal-AE pts in arm A had lower baseline DLCO. No other risk factors identified.
CREST (pre-immunotherapy) showed a modest OS benefit from thoracic RT after chemo; TREASURE tested that strategy on an IMpower133-style IO-maintenance backbone and found harm, not benefit.
Open-label; small N (68) and early termination leave OS underpowered with a wide CI. Phase 2; efficacy conclusions provisional, though the safety signal is robust.
Randomised harm signal (SAEs 61% vs 18%, fatal 19% vs 3%) argues against adding consolidative TRT to IO maintenance, contesting emerging RT enthusiasm; OS worse but underpowered by early stop.
In unselected ES-SCLC with at least stable disease after chemo-IO induction, this evidence argues against routinely adding consolidative thoracic RT to atezolizumab maintenance; it does not address the good-lung-function subset the authors flag as possibly selectable.
- Which lung-function-selected ES-SCLC pts might tolerate consolidative TRT on IO maintenance not yet Adebrelimab Combined with Chemotherapy and Thoracic Radiotherapy for First-line Treatment of ES-SCLC Phase 3n=524 · primary completion 2029-06 · phase 3 consolidative TRT on adebrelimab IO maintenance
- Whether lower-dose or delayed TRT lessens lymphocyte depletion and infection risk
📚 Sources · 📄 1 paper
Abstract
SUPREMO
ForpT1-2N1, pT3N0, or pT2N0 grade 3/LVI breast; post-mastectomy + systemic Rx
81.4% vs 81.9% (10-yr OS)
HR 1.04, 95% CI 0.82-1.30, P=0.80; did not meet OS
TL;DR10-yr OS 81.4% vs 81.9% (HR 1.04, P=0.80): chest-wall RT gives no OS benefit in intermediate-risk post-mastectomy breast cancer.
The RT read is local control without survival: CWI halved chest-wall recurrence (9 vs 20, HR 0.45) but the absolute gap stayed under 2 points and never reached OS or DFS. Fields were chest-wall-only (SCF 12%, IMC 1.5%), so this supports omitting CWI in intermediate-risk pN1 on modern systemic therapy, not nodal-RT calls.
Also covered Jul 9
8 details 5 trials watching
Phase 3 open-label RCT, 1:1, N=1607 ITT (808 CWI vs 799 no CWI) across 173 UK, European, and international sites. Median follow-up 9.6y, with 295 OS events (150 vs 145).
Intermediate-risk early breast: pT1N1, pT2N1, pT3N0, or pT2N0 with grade 3 and/or LVI. All had mastectomy, an axillary procedure, and adjuvant systemic therapy.
CWI 40-50 Gy to the chest wall. Supraclavicular fossa irradiated in only 97/808 CWI pts and IMC in 12/808 — this was chest-wall-only treatment, not comprehensive regional nodal RT.
Contemporary systemic backbone: 85% chemotherapy, 79% endocrine therapy, 19% trastuzumab.
OS, DFS, and DMFS were all null; the only endpoint favoring CWI was chest-wall recurrence (see table).
| Endpoint | CWI | No CWI | Effect |
|---|---|---|---|
| Overall survival | 81.4% | 81.9% | HR 1.04 (0.82-1.30), P=0.80 |
| Disease-free survival | 76.2% | 75.5% | HR 0.97 (0.79-1.18) |
| Distant MFS | 78.2% | 79.2% | HR 1.06 (0.86-1.31) |
| Chest-wall recurrence | 9 (1.1%) | 20 (2.5%) | HR 0.45 (0.20-0.99) |
EBCTCG PMRT meta-analysis (Lancet 2014) showed reduced recurrence and breast-cancer mortality in node-positive disease; SUPREMO finds no OS benefit in the intermediate-risk 1-3 node group treated in a modern systemic era.
Open-label; SCF/IMC coverage was sparse and non-standardized, so it does not test comprehensive regional nodal RT. Enrolment 2006-2013 predates some contemporary systemic regimens.
Adequately powered phase 3, prespecified OS endpoint, 10-yr f/u; null result diverges from EBCTCG-based routine PMRT for intermediate-risk 1-3 node disease.
In intermediate-risk post-mastectomy breast (pT1-2N1, pT3N0, or pT2N0 grade 3/LVI) on contemporary systemic therapy, this supports omitting chest-wall RT for survival; it does not extend to ≥4 positive nodes or to the comprehensive regional-nodal RT question.
- Does CWI omission hold in HER2+ and triple-negative intermediate-risk subgroups n=1106 · primary completion 2026-12 · phase 3 PMRT omission in pN1, 7y DFS non-inferiority
- Role of comprehensive regional nodal RT vs chest-wall-only in this population recruiting Evaluating Omitting of Internal Mammary Irradiation Among Early Stage Intermediate Risk (N1) Breast Cancer Phase NAn=214 · primary completion 2025-10 · omits IMN RT in N1 intermediate-riskactive Postmastecomy Internal Mammary Nodal Irradiation for High-risk Breast Cancer Patients Phase 3n=2400 · primary completion 2025-11 · phase 3 postmastectomy IMN RT vs none, DFSrecruiting The T-REX Trial: Tailored Regional External Beam Radiotherapy in Clinically Node-negative Breast Cancer Patients With 1-2 Sentinel Node Macrometastases. Phase NAn=1350 · primary completion 2028-12 · omits regional RT in 1-2 node macrometsrecruiting RecurIndex Guided Avoidance of Regional Nodal Irradiation for Node Positive Breast Cancer Phase NAn=540 · primary completion 2029-08 · RecurIndex-guided RNI vs none in N1
- Local control durability beyond 10 years
📚 Sources · 📄 1 paper
Abstract
NRG/RTOG 1112 NCT01730937
ForLocally advanced HCC, macrovascular invasion (74%), 1L systemic candidates
15.8 vs 12.3 mo
HR 0.77 (90% CI 0.59-1.01), 1-sided P=.06, ns; adjusted HR 0.72, P=.04
TL;DRAdding SBRT to sorafenib: mOS 15.8 vs 12.3mo (HR 0.77, 1-sided P=.06, ns primary); mPFS 9.2 vs 5.5mo, HR 0.55, P<.001.
The RT read is PFS, not the ns OS primary: mPFS 9.2 vs 5.5mo (HR 0.55, P<.001), a locoregional-control signal in a cohort 74% macrovascular-invasion, where liver-directed RT is hardest. Personalized 27.5-50Gy/5fx, no excess G3+ toxicity. Open decision: does SBRT still add over a modern IO backbone (sorafenib obsolete)?
8 details 3 trials watching
Phase 3 open-label RCT, 1:1, 193 randomized (177 eligible), stratified by performance status, liver function, degree of metastases, and macrovascular invasion. Accrual stopped early after first-line systemic SOC shifted.
Locally advanced HCC unsuitable for or refractory to standard locoregional therapy, fit for first-line systemic. 84.7% male, median age 66; macrovascular invasion in 74%.
Personalized SBRT, 27.5 to 50 Gy in 5 fractions, dose adapted to liver function, delivered before sorafenib.
Primary: overall survival. Secondary: progression-free survival, adverse events, quality of life.
Primary OS trend favored SBRT but missed the prespecified 1-sided threshold (P=.06); stratification-adjusted OS and the secondary PFS were both significant. See the endpoint table.
| Endpoint | SBRT+sorafenib | Sorafenib | Effect (HR/P) |
|---|---|---|---|
| mOS | 15.8 mo | 12.3 mo | HR 0.77 (90% CI 0.59-1.01), 1-sided P=.06 |
| mPFS | 9.2 mo | 5.5 mo | HR 0.55 (0.40-0.75), P<.001 |
| G3+ TRAE | 47% (39/83) | 42% (37/88) | P=.52 |
G3+ treatment-related AEs similar (47% vs 42%, P=.52). Treatment-related deaths: 2 with sorafenib (liver failure, death NOS), 1 with SBRT+sorafenib (lung infection). No excess RT-attributable toxicity.
Predates modern first-line combinations (atezolizumab-bevacizumab, durvalumab-tremelimumab); the sorafenib-alone comparator is now obsolete, leaving open whether SBRT adds over an IO backbone.
Open-label; accrual stopped early (underpowered); primary OS not significant unadjusted; comparator superseded; QoL assessed in small subsets (n=17-20).
Randomised phase 3 argues for adding SBRT to systemic in MVI-heavy HCC, but primary OS not significant (1-sided P=.06), stopped early, sorafenib comparator obsolete.
In locally advanced HCC with macrovascular invasion refractory to or unsuitable for standard locoregional therapy, this supports adding SBRT to first-line systemic as contested evidence; it does not establish benefit over a modern IO-based first-line backbone.
- Does SBRT add over modern IO-based first-line systemic therapy? recruiting Testing Immunotherapy With or Without Stereotactic Body Radiation Therapy in Patients With Advanced Liver Cancer, HELIO-RT Trial Phase 3n=226 · primary completion 2029-03 · phase 3 IO+SBRT vs IO alone
- Optimal SBRT dose and fractionation with impaired liver function recruiting A Pilot Study of Liver Protection Using Prednisone for Patients Receiving Stereotactic Body Radiation Therapy for Hepatocellular Carcinoma Phase 2n=20 · primary completion 2026-08 · prednisone liver-protection during SBRTn=18 · primary completion 2026-12 · phase 1 repeated-dose SBRT dose escalation
📚 Sources · 📄 1 paper
Abstract
BART
ForHigh-risk (T3-4/N+/R+) MIBC, post-cystectomy + chemo, no immunotherapy
HR 0.43
95% CI 0.20-0.96, p=0.04; 2y LRFFS 87.1% vs 76.0% (ITT)
TL;DR2y locoregional FFS 87.1% vs 76.0% (HR 0.43, p=0.04) with adjuvant pelvic RT post-cystectomy; OS not significant (HR 0.78, p=0.31).
Reported via UroToday →
The LRFFS benefit concentrates in the pN+ and T3+ subgroups (2y HR 0.22 and 0.25), and per-protocol it widens to HR 0.27 (93.2% vs 75.0%) once the 14 who never received RT are analysed as observation. Standard 50.4Gy/28fx to bed plus pelvic nodes transfers directly, so this moves the adjuvant-pelvic-RT decision for node-positive or margin-positive disease.
9 details 2 trials watching
Phase 3 multicentre RCT, 1:1, N=153 (RT 77 / obs 76), enrolled 2016-2024, stratified by nodal stage (N0/N+) and chemotherapy. Median follow-up 47 mo. Underpowered: accrual fell short of the sample-size goal.
High-risk (T3-4, N1-3, or R+) non-metastatic urothelial MIBC after radical cystectomy. 62% pT3-4, 41% pN+, 28% variant-histology component; median age 57, median 20 nodes dissected, 4.6% positive margins, 2.6% neobladder.
50.4 Gy / 28 fx to cystectomy bed plus pelvic nodes (common / internal / external iliac, presacral, obturator). Stoma- and bowel-sparing IMRT with daily onboard image guidance.
Primary: 2-year locoregional failure-free survival. Secondary: bladder-cancer-specific survival, DFS, overall survival. Fine-Gray competing-risk analysis (distant mets, non-cancer death).
Primary met; the time-to-event secondaries (DFS, BCSS, OS) all favoured RT numerically but none reached significance.
| Endpoint (2y) | Adjuvant RT | Observation | HR (95% CI), p |
|---|---|---|---|
| LRFFS (ITT) | 87.1% | 76.0% | 0.43 (0.20-0.96), p=0.04 |
| LRFFS (per-protocol) | 93.2% | 75.0% | 0.27 (0.10-0.71), p=0.008 |
| DFS | 71.6% | 58.7% | 0.62 (0.36-1.05), p=0.07 |
| BCSS | 79.6% | 65.0% | 0.59 (0.33-1.10), p=0.09 |
| OS | 70.4% | 57.4% | 0.78 (0.49-1.26), p=0.31 |
| Subgroup | HR (95% CI) |
|---|---|
| T3+ and N+ | 0.25 (0.07-0.84) |
| N+ disease | 0.22 (0.06-0.75) |
| Adverse event | Adjuvant RT | Observation |
|---|---|---|
| Late G3+ | 8.4% | 10.5% (p=0.60) |
| Acute G3 GI | 1.6% | 4.1% |
| Acute G2 GI | 17.5% | 1.4% |
Late grade 3+ toxicity comparable between arms; acute grade 2 GI higher with RT while grade 3 GI was lower, with no toxicity-related discontinuation.
Adjuvant RT after cystectomy is not routine (historic locoregional recurrence ~30% in high-risk pts); BART is the largest RCT in this space. A planned MERCY individual-patient-data meta-analysis will test the OS question.
Underpowered, OS not significant (HR 0.78, p=0.31) on a locoregional surrogate primary. 14/77 RT-arm pts never received RT, so the ITT HR (0.43) understates the per-protocol effect (HR 0.27). No immunotherapy used.
Randomised phase III, prespecified 2y LRFFS primary hit, diverging from the current no-adjuvant-RT norm. Underpowered and OS not significant, so short of practice-changing.
In pN+ or margin-positive high-risk MIBC after cystectomy and cisplatin chemo, this supports weighing adjuvant pelvic RT for locoregional control; it does not establish an OS benefit and does not extend to low-risk node-negative, margin-negative disease.
- OS benefit of adjuvant RT (planned MERCY IPD meta-analysis) n=76 · primary completion 2018-10 · adjuvant EBRT post-cystectomy, ≥pT3 high-riskactive Adjuvant Radiotherapy in Patients With Pathological High-risk Bladder Cancer (GETUG-AFU 30) Phase NAn=81 · primary completion 2027-12 · randomised adjuvant pelvic RT post-cystectomy, survival
- Adjuvant RT plus immunotherapy after cystectomy
📚 Sources · 📄 1 paper
Abstract
PRIMARY2 NCT05154162
ForBiopsy-naive men, high clinical risk, PI-RADS 2-3 MRI, PSA ≤20, ≤cT2
TL;DRNon-inferior csPCa detection (12% vs 16%, diff -3.7%) with PSMA-PET biopsy triage, avoiding biopsy in 49% of equivocal/negative-MRI men.
10 details 2 trials watching
Multicentre non-inferiority phase 3 RCT, 7 Australian hospitals, N=660 biopsy-naive men, randomised 1:1, unmasked, stratified by site. Recruited Mar 2022 to Aug 2025; follow-up ongoing.
Clinical suspicion of significant prostate cancer with non-suspicious or equivocal MRI (PI-RADS 2 in 51%, PI-RADS 3 in 49%) plus high clinical risk (PSA density >0.1, abnormal DRE, family history, BRCA, PSA >10). PSA ≤20 ng/mL, ≤cT2; median age 61, median PSA 5.2.
Co-primary: proportion with clinically significant cancer (Gleason ≥3+4, ≥10% pattern 4; non-inferiority margin 10%) and proportion of the PET arm avoiding biopsy by 6 months (20% threshold), by intention-to-treat.
Both co-primary endpoints met: csPCa detection non-inferior with PET triage, and biopsy avoided in nearly half the PET arm. Post-biopsy AE rates similar between arms.
| AE | PSMA-PET | Systematic biopsy |
|---|---|---|
| Pain | 33 (21%) | 62 (21%) |
| Haematuria | 60 (38%) | 126 (43%) |
| Haematospermia | 77 (48%) | 133 (45%) |
Open-label with no masking; follow-up ongoing, so long-term safety of avoided biopsies is unconfirmed. Single-country, single tracer ([68Ga]PSMA-11); health-economic and cross-radiopharmaceutical generalisability untested.
Phase 3 non-inferiority RCT met both co-primary endpoints; PSMA-PET biopsy triage diverges from biopsy-all standard. Open-label, single-country, follow-up ongoing.
- Safety of avoiding biopsy in PET-negative men over longer follow-up recruiting Image-guided Focal Dose Escalation- Primary pc Treated With Primary External Beam Hypofract.Stereotactic rt Phase NAn=374 · primary completion 2025-08 · candidate match
- Generalisability beyond Australia and to other PSMA radiopharmaceuticals n=18 · primary completion 2023-07 · candidate match
- Health-economic impact of PSMA-PET-first diagnostic pathway
📚 Sources · 📄 1 paper
mRCAT-III NCT06507371
ForpMMR/MSS LARC, cT3-4N0/+, tumor ≤10cm from verge, no lateral node
61.0% vs 28.6%
P<0.0001, ITT, blinded central review
TL;DRpCR 61.0% vs 28.6% (P<0.0001) with node-sparing SCRT + tislelizumab + CAPOX vs conventional SCRT + CAPOX in pMMR LARC.
The RT read is a confound, not a green light for nodal omission: the experimental arm changed two things at once, tumor-bed-only targeting AND added tislelizumab, so node-sparing's own contribution to the pCR doubling (61.0% vs 28.6%) can't be isolated. Node-sparing plausibly drove the lower severe-GI toxicity, but this doesn't yet license dropping elective nodal RT.

| Endpoint | Experimental | Control | P |
|---|---|---|---|
| pCR (ITT) | 61.0% (47/77) | 28.6% (22/77) | <0.0001 |
| MPR (TRG0+1) | 77.9% (60/77) | 50.6% (39/77) | <0.0001 |
+1 more figure

6 details 5 trials watching
Open-label, multicenter phase 3 RCT across 17 China hospitals; randomized 1:1, 77 pts per arm, stratified by clinical N stage (cN0 vs cN+). Primary pCR read by blinded independent central review.
pMMR/MSS rectal adenocarcinoma, cT3-4N0/+M0, tumor lower edge ≤10cm from the anal verge, ECOG 0-1, age 18-75, no positive lateral pelvic node.
Both arms CAPOX (oxaliplatin 130mg/m² d1, capecitabine 1000mg/m² d1-14). Experimental adds tislelizumab 200mg d1; control is chemo + RT only.
Both arms short-course 5Gy×5. Experimental is node-sparing (tumor bed only, spares tumor-draining nodes); control is conventional elective-nodal coverage. This target-volume contrast is the RT question.
Primary: pCR (ITT). Secondary: MPR, TRG, organ-preservation rate, EFS, OS, AEs.
Primary pCR and secondary MPR both favored the experimental arm (see figure); EFS, OS, organ-preservation not reported in source.
Experimental arm reported fewer severe GI AEs (author takeaway), plausibly from the smaller node-sparing volume; numeric AE rates not in source.
Control pCR 28.6% matches short-course RT + consolidation chemo benchmarks (RAPIDO ~28%). The novelty is a PD-1 benefit in an MSS population usually IO-refractory, with nodal-RT omission as the immunologic rationale.
Open-label; pCR is a surrogate with EFS/OS immature; the experimental arm confounds node-sparing target volume with added tislelizumab, so the RT-attributable effect can't be isolated; N=154, single country.
Divergent MSS-rectal result from a randomized P3 with blinded-review primary; kept off practice-changing because pCR is a surrogate (EFS/OS immature) and node-sparing is confounded with added tislelizumab.
In pMMR/MSS LARC (cT3-4, tumor ≤10cm from verge), this is a trial-stage signal that neoadjuvant PD-1 may help an IO-resistant group; it does not extend to dMMR disease and does not yet displace conventional elective-nodal short-course RT off-protocol.
- Node-sparing RT's independent contribution vs added tislelizumab
- Whether pCR gain translates to EFS, OS, organ preservation n=30 · primary completion 2025-01 · 1° endpoint organ-retention, MSS/pMMR SCRT+IOrecruiting Node-sparing Radiotherapy Combined With Total Neoadjuvant CAPOX and Sintilimab for MSS Middle and Low Rectal Cancer Phase 2n=37 · primary completion 2027-09 · node-sparing SCRT+PD-1, W&W organ preservation
- PD-1 benefit reproducibility in MSS/pMMR rectal cancer recruiting A Series of Neoadjuvant Chemoradiotherapy Combined With Immunotherapy for Locally Advanced Rectal Cancer Phase 2/3n=375 · primary completion 2026-12 · RCT chemoRT ± tislelizumab, pMMR/MSS LARCrecruiting Neoadjuvant Chemoradiotherapy Plus Tislelizumab With or Without Probio-M9 in pMMR/MSS Locally Advanced Rectal Cancer Phase 2n=50 · primary completion 2027-05 · pMMR/MSS chemoRT+tislelizumab vs CRT-only armnot yet Neoadjuvant Chemoradiotherapy Followed by Chemotherapy With or Without Tislelizumab for Resectable Ultra-low Rectal Cancer: The RELIEVE-02 Study Phase 3n=154 · primary completion 2027-12 · phase 3 chemoRT ± tislelizumab, pMMR/MSS
📚 Sources · 🐦 1 tweet
One of most interesting rectal ca studies at #ASCO26
— Dr. Nina Niu Sanford (@NiuSanford) June 2, 2026
P3 RCT in pMMR LARC: Node-sparing short-course RT + CAPOX + tislelizumab doubled pCR v conventional SCRT + CAPOX (61 v 29%)
Hypothesis = sparing elective node RT preserves antitumor immunity & improves PD1 response @OncoAlert pic.twitter.com/6xvA6ne0mg
LBA8005: Concurrent Thoracic RT + Chemoimmunotherapy in ES-SCLC
ForTreatment-naïve ES-SCLC, stage IV or III ineligible for curative chemoRT
HR 1.14
10.0 vs 11.8 mo, 95% CI 0.84-1.56, p=0.40; OS not met
TL;DROS 10.0 vs 11.8 mo, HR 1.14 (0.84-1.56), p=0.40: concurrent thoracic RT added no benefit to durvalumab-based chemoIO in ES-SCLC.
The tested RT is concurrent (30 Gy/10 fx, day 21-28 with chemoIO), not CREST's consolidative post-chemo RT in responders, so the consolidative question stays open. Even the low-burden subgroup without brain or liver metastases was null (HR 1.10). Adding concurrent thoracic RT to chemoIO carries no OS benefit.

| Arm | Median OS | HR (95% CI) | p |
|---|---|---|---|
| ChemoIO + TRT | 10.0 mo | 1.14 (0.84-1.56) | 0.40 |
| ChemoIO | 11.8 mo | n/a | n/a |
+2 more figures

| Subgroup | ChemoIO+TRT | ChemoIO | HR (95% CI) | p |
|---|---|---|---|---|
| Completed 4 chemoIO courses | 11.9 mo | 12.1 mo | 1.02 (0.72-1.44) | 0.92 |
| No brain/liver mets | 11.9 mo | 13.2 mo | 1.10 (0.65-1.87) | 0.72 |

| Arm | Median PFS | HR (95% CI) | p |
|---|---|---|---|
| ChemoIO + TRT | 5.1 mo | 1.10 (0.84-1.45) | 0.49 |
| ChemoIO | 5.0 mo | n/a | n/a |
7 details 5 trials watching
Randomized phase III, 1:1 (chemoIO+TRT n=115, chemoIO n=113). Stratified by liver and brain metastases. Primary: overall survival; secondary ORR, PFS, toxicity.
Treatment-naïve ES-SCLC, stage IV or stage III ineligible for curative chemoRT, ECOG 0-1, ≥1 measurable thoracic lesion. Asymptomatic or stable brain metastases allowed.
Four cycles durvalumab 1500 mg + carboplatin AUC 5 + etoposide (100 mg/m² IV days 1-3, or 200 mg/m² PO days 2-4) Q3W, then durvalumab 1500 mg Q4W maintenance.
Concurrent thoracic RT 30 Gy in 10 fractions, starting day 21-28. PCI 25-30 Gy offered to responders in both arms; WBRT 20-30 Gy for brain metastases per routine.
Primary OS not met and numerically favored chemoIO alone; PFS and both prespecified subgroups (course completers, no brain/liver metastases) were also null. Effect sizes in figures.
CREST (Slotman, Lancet 2015) used the same 30 Gy/10 fx but as consolidative RT after chemotherapy in responders, before immunotherapy, and suggested a survival benefit. Adding RT concurrently to chemoIO shows none.
Open-label (RT cannot be blinded). Tests only the concurrent schedule, not the consolidative timing prior data supported. No toxicity or RT-delivery data in source to explain the numerically inferior OS.
Randomised phase III, prespecified OS primary, null; contests the CREST-era expectation that thoracic RT benefits ES-SCLC, now tested concurrently with chemoIO.
In treatment-naïve ES-SCLC beginning durvalumab plus platinum/etoposide, this questions adding concurrent thoracic RT (no OS benefit); it does not extend to consolidative thoracic RT given after chemotherapy in responders.
- Does consolidative thoracic RT after chemoimmunotherapy still benefit ES-SCLC? n=150 · primary completion 2025-03 · RT to all residual lesions after chemoIO in ES-SCLCrecruiting Phase II Trial of Consolidative Thoracic Radiotherapy for ES-SCLC After Standard Care of Chemo-immunotherapy Phase NAn=104 · primary completion 2025-09 · single-arm consolidative TRT after PD-1/L1 chemoIOrecruiting Association of Thoraco-mediastinal Radiotherapy With Maintenance Immunotherapy Treatment With Atezolizumab Phase 2n=37 · primary completion 2026-12 · thoraco-mediastinal RT + maintenance atezolizumab
- Optimal timing and sequencing of thoracic RT with chemoimmunotherapy active Low-dose Radiotherapy Combined With Durvalumab, Chemotherapy(EP) in the Treatment of ES-SCLC Phase 2n=30 · primary completion 2023-02 · low-dose RT concurrent with 1L durvalumab chemon=46 · primary completion 2027-12 · sequential TRT after 1L durvalumab chemoIO
📚 Sources · 🐦 1 tweet
🚨 #ASCO26 | #️⃣LBA8005⁰☢️ Concurrent thoracic radiotherapy + chemoimmunotherapy in ES-SCLC
— Masahiro TORASAWA, MD. PhD. (@M_Torasawa) June 2, 2026
👥 ES-SCLC⁰Durvalumab + platinum/etoposide⁰± concurrent thoracic radiotherapy⁰TRT: 30 Gy / 10 fractions, starting day 21–28
📊 Randomized phase III⁰ChemoIO + TRT: n=115⁰ChemoIO… pic.twitter.com/TDA5amz59e
ROADS
ForResected brain metastasis > 2 cm, post-op cavity RT candidates
NR vs 17 mo
Surg bed recurrence 1% GammaTile vs 12% SRS
TL;DRSurgical bed recurrence 1% vs 12% and 2yr OS 62% vs 36% favoring intraoperative GammaTile brachytherapy over post-op SRS for resected brain mets >2cm.
The safety tradeoff the headline buries: leptomeningeal disease ran 10% with GammaTile vs 3% with SRS, even as surgical-bed recurrence fell to 1% vs 12%. Radiation necrosis was comparable (8% vs 7%). This moves the intraoperative-brachytherapy-vs-staged-cavity-SRS decision for resected mets >2 cm, where SRS local control is weakest.

| Endpoint | GammaTile | SRS |
|---|---|---|
| Time to surg bed recurrence | NR | 17 mo |
| Surg bed recurrence-free survival | NR | 11 mo |
| 2-yr OS | 62% | 36% |
8 details 2 trials watching
Randomized trial, N=230, resected brain metastasis > 2 cm. GammaTile (Cs-131 collagen-tile brachytherapy) placed in the cavity at resection vs post-op stereotactic radiosurgery. ASCO 2026 final results. Primary: time to surgical bed recurrence and surgical-bed recurrence-free survival.
Resected brain metastasis > 2 cm, the larger-cavity setting where single-fraction post-op SRS local control is weakest. Histology / primary tumor not specified in source.
Experimental: intraoperative permanent Cs-131 seed brachytherapy (GammaTile) at resection. Control: post-op cavity SRS. Dose, fractionation, and cavity margin not reported in source.
Both primary endpoints and 2yr OS favored GammaTile. Safety: radiation necrosis comparable (8% vs 7%), leptomeningeal disease higher with brachytherapy (10% vs 3%).
Post-op cavity SRS is the current standard for resected brain mets (N107C, Mahajan). ROADS challenges it, favoring intraoperative brachytherapy on local control.
Abstract-only, not yet peer-reviewed; open-label. The 2yr OS advantage is large for a local therapy and OS was not a stated primary endpoint, raising the question of baseline arm imbalance.
Randomized, primary endpoint (surg bed control) hit favoring intraop brachy over the post-op SRS standard; but abstract-only, open-label, and the large OS gain warrants scrutiny.
In pts with a resected brain metastasis >2 cm needing cavity radiotherapy, this supports intraoperative brachytherapy as an alternative to post-op SRS for local control; it does not extend to intact (unresected) mets or cavities ≤2 cm.
- Whether the large OS gain reflects arm imbalance vs true benefit active Post-Surgical Stereotactic Radiotherapy (SRT) Versus GammaTile-ROADS (Radiation One and Done Study) Phase 3n=230 · primary completion 2029-08 · randomized phase 3 GammaTile vs SRT
- Leptomeningeal failure risk with intraoperative brachytherapy active Intracavitary Carrier-embedded Cs131 Brachytherapy for Recurrent Brain Metastases: a Randomized Phase II Study Phase 2n=103 · primary completion 2026-12 · randomized brachytherapy vs surgery-alone safety
- Applicability to resection cavities ≤ 2 cm
📚 Sources · 🐦 1 tweet
🚨🚨 ASCO 2026 Final Results Randomized trial resected brain met Brachytherapy vs Post-Op SRS🚨
— PDBrown (@PDBrownOnc) May 30, 2026
- Incredible Surg Bed Control with Brachy (↑↑OS as well)
- Surg bed recurrence 12% SRS vs 1% GammaTile pic.twitter.com/PCTsCluyUd
Neo-CRAG
ForHigh-risk locally advanced gastric/EGJ (cT3N2-3 to cT4), fit for D2 resection
mDFS 52.7 vs 24.4 mo
HR 0.750 (95% CI 0.607-0.928), P=0.008
TL;DRAdding neoadjuvant chemoRT (45Gy/25fx) to periop XELOX improved mDFS 52.7 vs 24.4mo (HR 0.75) and mOS 67.5 vs 37.6mo in high-risk LAGC.
The RT read is clean attribution: both arms share the XELOX backbone and the CRT arm got dose-reduced chemo during RT, yet locoregional recurrence halved (9.4% vs 18.3%) with more ypN0 and downstaging. On 45Gy/25fx, this revives neoadjuvant chemoRT for high-risk D2-resected gastric/EGJ, on a non-FLOT backbone.

| Endpoint | CRT | CT | HR (95% CI), P |
|---|---|---|---|
| Median DFS | 52.7 mo | 24.4 mo | 0.750 (0.607-0.928), P=0.008 |
| 3-yr DFS | 55.6% | 42.4% | — |
| Median OS | 67.5 mo | 37.6 mo | 0.781 (0.628-0.970), P=0.025 |
| 5-yr OS | 50.1% | 44.2% | — |
7 details 2 trials watching
Phase 3 open-label RCT, 1:1, N=620 (310/arm), 13 Chinese referral centers, enrolled 2013-2022. Primary: disease-free survival; secondary OS, pCR, R0, safety.
High-risk locally advanced gastric/EGJ adenocarcinoma: cT3N2-3M0, cT4aN+M0, or cT4bNanyM0; 36.3% EGJ (Siewert II/III). All planned standardized D2 gastrectomy.
Both arms: 3 cycles preoperative + 3 cycles adjuvant XELOX (oxaliplatin 130, capecitabine 1000 BID D1-14, Q3W) around D2 gastrectomy.
CRT arm only: concurrent 45 Gy/25 fx begun after chemo cycle 1, with dose-reduced XELOX (oxaliplatin 100, capecitabine 825) during RT. RT is the sole added variable between arms.
Primary DFS met and secondary OS positive, both favoring CRT; pathologic downstaging, ypN0, and locoregional control also improved (see figure and table).
Contrasts with CRITICS and TOPGEAR, where adding radiotherapy to a chemo backbone did not improve survival. A positive DFS/OS here reopens neoadjuvant chemoRT in high-risk, D2-resected LAGC.
Open-label; non-FLOT XELOX backbone limits transfer to current perioperative standard. Single-country (China) with high D2-resection quality; DFS (not OS) was the primary endpoint.
Randomised phase 3, primary DFS and OS both hit, but positive chemoRT diverges from negative CRITICS/TOPGEAR; non-FLOT XELOX backbone limits transfer to current SOC.
In high-risk cT3N2-3/cT4 gastric or EGJ adenocarcinoma planned for D2 gastrectomy on a XELOX backbone, these data support a DFS/OS and locoregional-control benefit from adding neoadjuvant chemoRT; the signal does not extend to FLOT-backbone or metastatic patients.
- Incremental benefit of RT on a FLOT chemo backbone n=776 · primary completion 2023-06 · candidate match
- Generalizability beyond high-quality-D2 Asian centers
- Whether EGJ and distal gastric benefit equally n=4 · primary completion 2024-03 · candidate match
📚 Sources · 🐦 1 tweet
Neo-CRAG: Ph3 RCT (n=620, gastric/GEJ) - adding neoadj chemoRT to peri-op XELOX improved OS (68 v 38 mo).
— Dr. Nina Niu Sanford (@NiuSanford) May 30, 2026
Limitation=non-FLOT, BUT still relevant IMO b/c:
1) DFS/OS benefit substantial.
2) Improvements in pCR, downstg, LRR supports plausible RT effect on OS. #ASCO26 @OncoAlert pic.twitter.com/eeM0Z8p20M
PEACE V-STORM NCT03569241
ForPelvic nodal oligorecurrent prostate (≤5 nodes), post radical local Rx, PS 0-1
76% vs 63% at 4y
HR 0·62 (80% CI 0·44-0·86), p=0·063
TL;DR4-yr MFS 76% vs 63% favoring ENRT over MDT for pelvic nodal oligorecurrence, HR 0·62 (80% CI 0·44-0·86, p=0·063).
The RT read: whole-pelvis ENRT (45 Gy/25fx + SIB 65 Gy) beat node-only MDT on 4-yr MFS (76% vs 63%, HR 0·62), consistent with occult pelvic nodal disease driving the failures MDT leaves untreated. Moves the elective-nodal-coverage decision in ≤5-node pelvic recurrence.
7 details 1 trial watching
Phase 2, open-label, randomised (1:1) screening trial, 21 hospitals in 6 countries. 196 randomised (MDT 99, ENRT 97), 190 evaluable, modified ITT. Median follow-up 50 mo (IQR 42-58).
Men with PET-detected pelvic nodal oligorecurrence (≤5 nodes) after radical local prostate treatment; WHO PS 0-1, histologically confirmed adenocarcinoma. All male.
ENRT: 45 Gy/25fx whole pelvis + SIB 65 Gy to PET-positive nodes (or salvage LND). MDT: SBRT 30 Gy/3fx every other day (or salvage LND). Both + 6 mo ADT. Stratified by tracer (choline vs PSMA) and MDT type.
Primary: metastasis-free survival (any M1 on PET or death), modified ITT. Reported with 80% CIs, a phase 2 screening threshold, not the conventional 95%.
Grade 3 events low in both arms and numerically higher with ENRT (urinary incontinence, diarrhoea). No treatment-related deaths.
First randomised ENRT-vs-MDT comparison for nodal oligorecurrence. Prior oligomet RCTs (STOMP, ORIOLE) tested MDT vs observation, not elective nodal RT, so this adds the missing head-to-head.
Open-label; primary endpoint p=0·063 did not clear conventional significance and rests on a phase 2 screening design. Authors position ENRT as a potential standard awaiting phase 3.
| Endpoint | ENRT (80% CI) | MDT (80% CI) | HR (80% CI) |
|---|---|---|---|
| 4-yr MFS | 76% (69-81) | 63% (56-69) | 0·62 (0·44-0·86), p=0·063 |
| Grade 3 AE | ENRT | MDT |
|---|---|---|
| Urinary incontinence | 10% | 6% |
| Diarrhoea | 2% | 1% |
First randomised ENRT-vs-MDT comparison; ENRT's MFS edge diverges from MDT-favouring practice. Phase 2 screening design, p=0·063, awaits phase 3.
In men with PET-detected pelvic nodal-only oligorecurrence (≤5 nodes) after radical local treatment, this favors whole-pelvis ENRT over node-only MDT; it does not extend to extrapelvic M1, bone, or visceral oligometastatic recurrence.
- Phase 3 confirmation of ENRT superiority over MDT n=26 · primary completion 2029-07 · elective nodal SBRT added to MDT for nodal oligorecurrence
- Whether the MFS benefit translates to overall survival
- Long-term GU and GI toxicity of whole-pelvis ENRT with SIB
📚 Sources · 📄 1 paper
EORTC 22922/10925
ForStage I-III breast, medial/central primary or axillary node-positive
HR 1.00
95% CI 0.90-1.10, p=.967; 20yr OS 61.0% vs 61.8% (ns)
TL;DR20yr OS 61.0% vs 61.8%, HR 1.00 (p=.967): IM-MS-RT cut breast cancer mortality (HR 0.82) but raised non-BC deaths (HR 1.26).
The RT read is competing mortality: IM-MS-RT's breast cancer mortality benefit (HR 0.82) is fully offset by excess cardiac and lung deaths (HR 1.26) at 20yr. With 1996-2004 planning the survival case nets to zero, so contemporary heart-sparing (DIBH/IMRT) is the variable that decides whether IM-MS nodal coverage still pays off.
7 details 5 trials watching
Phase 3 multicenter RCT with central RT quality assurance; 4004 women randomized 1996-2004 to added IM-MS nodal RT vs none. Prespecified for final analysis at 20yr on a delayed-benefit hypothesis; median follow-up 22.2yr.
Stage I-III breast adenocarcinoma, age ≤75. Eligible if central/medial primary (any nodal status) OR any-quadrant primary with axillary node involvement. Surgery was mastectomy or BCS plus ALND; median age 54.
Intervention added internal-mammary + medial-supraclavicular (levels 3-4) nodal irradiation on top of standard breast/chest-wall RT. 1996-2004 planning era (2D/3D, pre-DIBH/IMRT); dose and fractionation not specified in source text.
Primary: overall survival. Secondary: disease-free survival, distant metastasis-free survival, breast cancer mortality, any breast recurrence.
Primary OS was flatly null; the significant efficacy signals (lower breast cancer mortality, fewer breast recurrences) were offset in OS terms by excess non-breast-cancer deaths. Per-endpoint numbers in the table.
| Endpoint (20yr) | IM-MS-RT | Control | HR (95% CI), p |
|---|---|---|---|
| Overall survival | 61.0% | 61.8% | 1.00 (0.90-1.10), p=.967 |
| Disease-free survival | 48.2% | 49.0% | 0.97 (0.89-1.06), p=.515 |
| Distant metastasis-free | 58.9% | 59.8% | 0.97 (0.88-1.08), p=.578 |
| Breast cancer mortality | 18.6% | 22.4% | 0.82 (0.72-0.95), p=.006 |
| Non-BC/unknown deaths | 20.4% | 15.8% | 1.26, p=.002 |
| Late morbidity | IM-MS-RT | No IM-MS-RT |
|---|---|---|
| Lung fibrosis | 6.3% | 3.2% |
| Cardiac fibrosis | 2.7% | 1.7% |
| Cardiac disease | 15.2% | 11.7% |
| Severe cardiac (G3-4) | 1.9% | 1.7% |
| Severe lung (G3-4) | 0.3% | 0.0% |
Excess late lung fibrosis, cardiac fibrosis, and cardiac disease with IM-MS-RT is the mechanism behind the competing non-breast-cancer mortality; severe grade 3-4 cardiac and lung events stayed rare in both arms (table).
Aligns with the 10-yr EORTC 22922 report (Poortmans, NEJM 2015) and MA.20 in showing regional nodal RT improves disease control more than OS. The new 20yr signal: late cardiopulmonary deaths neutralize the breast cancer mortality gain.
1996-2004 planning predates modern cardiac-sparing, so the non-breast-cancer-death penalty likely overstates contemporary risk. Systemic therapy followed era standards (tamoxifen era), not current regimens. OS as primary is a high bar a single nodal-RT field rarely clears.
Large randomized phase 3, OS-primary, 22yr f/u: internally valid to contest the IM-MS-RT survival rationale, which the mortality-toxicity tradeoff nullifies. Divergence is the headline.
In a woman with a medial/central or node-positive stage I-III breast tumor, this tempers the survival rationale for adding the internal-mammary + medial-supraclavicular field specifically; it does not change breast/chest-wall or axillary RT indications.
- Does modern heart-sparing RT (DIBH/IMRT) preserve the mortality benefit without the cardiac penalty? recruiting Robustness Evaluation of Deep Inspiration Breath-Hold (DIBH) Plans in Internal Mammary Irradiationn=25 · primary completion 2026-12 · DIBH heart sparing while covering IMNn=500 · primary completion 2029-11 · IMPT vs IMRT toxicity for nodal breast RT
- Which subgroups still net an OS gain from IM-MS-RT coverage? active Postmastecomy Internal Mammary Nodal Irradiation for High-risk Breast Cancer Patients Phase 3n=2400 · primary completion 2025-11 · IMN vs no-IMN on DFS in high-risk pts
- Optimal patient selection for internal-mammary chain coverage in the contemporary era recruiting Evaluating Omitting of Internal Mammary Irradiation Among Early Stage Intermediate Risk (N1) Breast Cancer Phase NAn=214 · primary completion 2025-10 · clinical-genomic model to omit IMI in N1recruiting Radiotherapy Dose Adaptation Based on Tumor Biology in Patients With cN2b-N3 Breast Cancer Phase NAn=120 · primary completion 2028-03 · dose adaptation for IM/SCV nodal mets
📚 Sources · 📄 1 paper
Abstract
Bladder Adjuvant Radiotherapy Trial
ForHigh-risk MIBC post-cystectomy (pT3-4, N+, or margin+), chemo-treated
HR 0.43
2y LRFS 87.1% vs 76.0%; 95% CI 0.20-0.96, P=.04
TL;DR2y LRFS 87.1% vs 76.0%, HR 0.43 (0.20-0.96) P=.04 favoring adjuvant pelvic IMRT after cystectomy; DFS/BCSS/OS all NS.
Locoregional control is the RT read: 2y LRFS 87.1% vs 76.0% (HR 0.43) with stoma-sparing IG-IMRT 50.4Gy/28fx to the cystectomy bed plus pelvic nodes, no added severe toxicity. DFS, BCSS, and OS all trended toward RT but none significant at N=153, reopening adjuvant pelvic RT for high-risk MIBC without settling survival benefit.
8 details 3 trials watching
Phase 3 multicenter RCT, 1:1, N=153 (RT=77 vs Obs=76); stratified by nodal involvement and chemotherapy timing (neoadjuvant/adjuvant/none). Median follow-up 47 mo.
High-risk nonmetastatic urothelial MIBC after radical cystectomy: any of pT3-4, N1-3, margin-positive, or ≤10 nodes dissected. Enrolled 62% pT3-4, 41% pN+.
Stoma-sparing IG-IMRT, 50.4Gy in 28 fractions to the cystectomy bed and pelvic nodes.
Over 90% received perioperative chemotherapy (71% neoadjuvant, 20% adjuvant). None received immunotherapy.
Primary: 2-year locoregional recurrence-free survival. Secondary: disease-free survival, bladder-cancer-specific survival, overall survival.
Primary LRFS met (HR 0.43, P=.04); DFS, BCSS, and OS all favored RT but none reached significance (see table).
| Endpoint | RT | Obs | HR (95% CI) |
|---|---|---|---|
| 2y LRFS (1°) | 87.1% | 76.0% | 0.43 (0.20-0.96), P=.04 |
| DFS | 71.6% | 58.7% | 0.62 (0.36-1.05) |
| BCSS | 79.6% | 65.0% | 0.59 (0.33-1.10) |
| OS | 70.4% | 57.4% | 0.78 (0.49-1.26) |
No additional severe toxicity reported with adjuvant pelvic IMRT versus observation.
Reopens the adjuvant-RT-after-cystectomy question that prior Egyptian NCI trials raised for local control; first randomized test in the modern IG-IMRT era.
Small (N=153); primary endpoint is a locoregional-control surrogate, and survival endpoints were underpowered and nonsignificant. No immunotherapy-era comparator.
Randomised phase III hit prespecified primary LRFS endpoint favoring adjuvant RT (non-standard); but N=153 and DFS/BCSS/OS all NS. Field reopened, not settled.
In high-risk post-cystectomy MIBC (pT3-4, N+, or margin+) after perioperative chemo, this supports adjuvant pelvic IMRT as a locoregional-control option but not a proven survival gain; it does not extend to organ-confined, node-negative low-risk disease.
- Does the locoregional control benefit translate to overall survival in a larger trial? active Adjuvant Radiotherapy in Patients With Pathological High-risk Bladder Cancer (GETUG-AFU 30) Phase NAn=81 · primary completion 2027-12 · randomized adjuvant post-cystectomy RT, survival EP
- How does adjuvant RT integrate with adjuvant immunotherapy (nivolumab)? active Adjuvant Nivolumab Following Chemo-Radiation in Localized Muscle-Invasive Bladder Cancer Phase 2n=200 · primary completion 2025-02 · adjuvant nivolumab after chemoRT, 2y FFS EPrecruiting Adjuvant Concurrent Immunotherapy and Radiotherapy for the Treatment of Bladder Cancer Phase 1n=10 · primary completion 2027-04 · adjuvant concurrent IO + RT for bladder cancer
- Which high-risk subgroup (pN+ vs margin+) benefits most from adjuvant RT?
📚 Sources · 📄 1 paper
Abstract
High-Dose Hyperfractionated SIB RT vs Standard RT for LS-SCLC NCT03214003
ForLS-SCLC, age 18-70, ECOG 0-1, ≤1 prior chemo course
TL;DRmOS 60.7 vs 39.5mo, HR 0.55 (0.37-0.72), p=0.003 favoring dose-escalated 54Gy BID SIB over standard 45Gy BID in LS-SCLC.
The escalation route is the RT read: 54Gy/30fx twice-daily via SIB beat the 45Gy BID standard (HR 0.55) where prior once-daily escalation (CONVERT, CALGB 30610) didn't, with grade 3-4 oesophagitis (13% vs 12%) and pneumonitis (5% vs 6%) flat. Moves the dose-escalation decision toward hyperfractionation, not once-daily.
7 details 3 trials watching
Open-label phase 3 RCT at 16 Chinese public hospitals, randomised 1:1 (54Gy n=108, 45Gy n=116), N=224. Median follow-up 46 mo. DSMB stopped the trial early for benefit (Apr 2021).
LS-SCLC, age 18-70, ECOG 0-1, previously untreated or ≤1 course of platinum-etoposide. Median age 64 (IQR 58-68), 54% male. Stratified by ECOG, stage, prior chemo course and choice.
Both arms VMAT twice-daily, 10 fx/week, PTV 45Gy/30fx. Experimental arm adds a simultaneous integrated boost to 54Gy/30fx to the gross tumour volume. PCI 25Gy/10fx for responders.
Primary: overall survival in the ITT population. Safety analysed as-treated.
mOS 60.7 mo (95% CI 49.2-62.0) with 54Gy vs 39.5 mo (27.5-51.4) with 45Gy, HR 0.55 (0.37-0.72), p=0.003.
Grade 3-4 oesophagitis 13% vs 12% (p=0.84) and pneumonitis 5% vs 6% (p=0.663), no excess with dose escalation. One treatment-related death (MI) in the 54Gy arm.
Prior escalation via once-daily RT (CONVERT, CALGB 30610) did not beat 45Gy BID; this instead escalates the twice-daily schedule with a SIB and shows an OS gain.
Open-label; early DSMB termination for benefit can overestimate the effect. Single-country, modest N=224, and predates adjuvant durvalumab consolidation (ADRIATIC).
Randomised phase 3, primary OS hit (HR 0.55), diverges from the 20-yr 45Gy BID standard. Open-label and DSMB-stopped-early temper it, but design is valid for the divergence.
In fit LS-SCLC pts aged 18-70 with ECOG 0-1 on concurrent chemoradiation, this supports 54Gy/30fx twice-daily thoracic RT over the 45Gy standard; it does not extend to pts over 70, ECOG 2+, or the durvalumab-consolidation era.
- Generalizability beyond age ≤70, ECOG 0-1, Asian cohort
- Optimal RT dose alongside durvalumab consolidation n=65 · primary completion 2027-01 · SIB high-dose RT then PD-L1 maintenance, LS-SCLC
- Confirmation in a multinational trial given early stopping active Two Schedules of Hyperfractionated Thoracic Radiotherapy in Limited Disease Small Cell Lung Cancer Phase NAn=177 · primary completion 2020-07 · randomised 45 vs 60Gy BID hyperfractionated TRTrecruiting Dose-Escalation Radiotherapy in Limited-Stage Small Cell Lung Cancer: A Phase III Randomized Trial Phase 3n=300 · primary completion 2028-09 · phase 3 RCT: 45 vs 60 vs SIB 45-54Gy BID
📚 Sources · 📄 1 paper
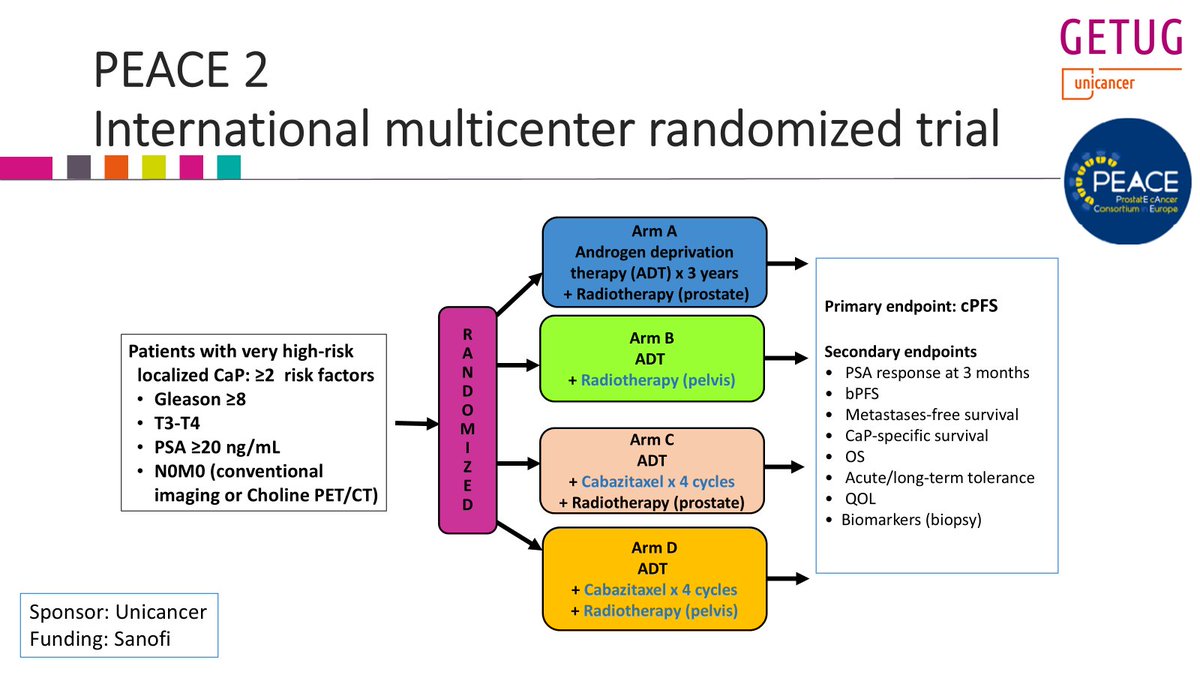
PEACE 2
ForcN0 very-high-risk localized prostate (Gleason≥8, T3-4, or PSA≥20)
HR 0.81, ns
95% CI 0.63-1.03, p=0.088; primary endpoint not met
TL;DRPelvic nodal RT missed 1° endpoint: 7yr cPFS 67.1% vs 62.9% prostate-only, HR 0.81 (0.63-1.03) p=0.088; no MFS/PCSS/OS gain.
The RT decision is elective nodal coverage: a randomized head-to-head (n=380 vs 381) shows whole-pelvic RT adds no cPFS, MFS, PCSS or OS benefit over prostate-only in cN0 very-high-risk disease, with modern-technique toxicity minimal. Staging was conventional imaging/choline PET, not PSMA, so PSMA-defined N0 pts remain untested.
Also covered May 17

| Arm | 7yr cPFS (95% CI) | HR (95% CI) | p |
|---|---|---|---|
| Prostate-only RT | 62.9% [57.4-68.1] | ref | |
| Pelvic RT | 67.1% [61.6-72.2] | 0.81 [0.63-1.03] | 0.088 |
+1 more figure
8 details 2 trials watching
Phase 3 randomized 2×2 factorial (pelvic vs prostate-only RT × cabazitaxel ×4 vs none), ADT ×3 yr in all arms. Pelvic-RT comparison n=380 vs 381, 7-year outcomes reported. Multicenter GETUG/Unicancer.
Very high-risk localized prostate: ≥2 of Gleason ≥8, T3-T4, PSA ≥20 ng/mL. N0M0 by conventional imaging or choline PET/CT, not PSMA.
High-dose RT to prostate vs whole pelvis. Dose, fractionation and nodal target volume not reported in source.
Primary: clinical PFS. Secondary: PSA response at 3 mo, bPFS, MFS, PCSS, OS, tolerance, QoL, biopsy biomarkers.
cPFS 7yr 67.1% pelvic vs 62.9% prostate-only, HR 0.81 (0.63-1.03), p=0.088, primary endpoint not met. No benefit on MFS, PCSS or OS per authors.
Authors report side effects minimal with modern RT technique; per-arm toxicity rates not reported in source.
POP-RT (2021) found whole-pelvic RT improved biochemical control in PSMA-staged high-risk N0. PEACE 2's conventionally-staged cohort shows no benefit.
Conference presentation, not peer-reviewed. Non-PSMA staging risks occult nodal misclassification. cPFS is a surrogate; RT dose/technique unspecified in source.
Randomized phase 3, prespecified cPFS not met (p=0.088); null across all clinical endpoints diverges from POP-RT's whole-pelvic benefit, so the WPRT question is contested.
In cN0 very-high-risk localized prostate staged by conventional imaging or choline PET, this questions routine elective whole-pelvic RT; it does not address PSMA-staged N0 or radiologic node-positive disease.
- Whether PSMA-staged N0 pts benefit from elective pelvic RT
- Cabazitaxel's effect and interaction with pelvic RT active A Phase III of Cabazitaxel and Pelvic Radiotherapy in Localized Prostate Cancer and High-risk Features of Relapse Phase 3n=761 · primary completion 2025-12 · phase 3 cabazitaxel + pelvic RT, high-risk localized
- A nodal-risk subgroup that still benefits from pelvic RT recruiting Abi/Pred + ADT vs ADT in PSMA-Positive, Conventionally Node-Negative Prostate Cancer Phase 2n=140 · primary completion 2033-04 · PSMA-avid occult nodes; RT + abiraterone ADT
📚 Sources · 🐦 1 tweet
Yesterday, I presented the @GETUG_Unicancer PEACE 2 trial at #ESTRO26 on the role of pelvic RT in very high risk #prostatecancer pts (staged with conventional imaging).
— Pierre Blanchard, MD (@PBlanchardMD) May 18, 2026
Twittorial below
Key conclusion: pelvic RT did not improve clinical outcomes (cPFS, MFS, PCSS, OS)...
1/n pic.twitter.com/ZKRt2QZzt1
PEACE-2
ForVery high-risk localized N0M0 prostate ca (≥2 of GS≥8, T3-T4, PSA≥20)
67.1% vs 62.9% at 7yr
HR 0.81, 95% CI 0.63-1.03, p=0.088; primary endpoint not met
TL;DR7yr cPFS 67.1% pelvic vs 62.9% prostate-only RT, HR 0.81 (0.63-1.03), p=0.088: primary endpoint not met.
The elective pelvic nodal decision in very high-risk N0 disease loses its randomized support: 4.2 absolute points of 7yr cPFS, HR 0.81, CI crossing 1. Staging was conventional or choline PET, so pts PSMA PET would now upstage sat in both arms, diluting any true nodal benefit. Toxicity by arm not reported in source.
Also covered May 18

| Arm | 7yr cPFS | HR (95% CI) | p |
|---|---|---|---|
| Pelvic RT | 67.1% (61.6-72.2) | 0.81 (0.63-1.03) | 0.088 |
| Prostate-only RT | 62.9% (57.4-68.1) | n/a | n/a |
+2 more figures


7 details 5 trials watching
International multicenter randomized trial with four arms crossing RT volume (prostate vs pelvis) with cabazitaxel ×4 cycles, all on ADT ×3 years. Readout presented at ESTRO 2026 with 7-year outcomes and follow-up extending to 120 months.
Very high-risk localized prostate cancer defined as ≥2 risk factors among Gleason ≥8, T3-T4, and PSA ≥20 ng/mL. N0M0 by conventional imaging or choline PET/CT.
The randomized comparison is target volume: prostate-only versus pelvic irradiation. Dose, fractionation, and nodal CTV definition are not reported in the source.
Primary: cPFS. Secondary: PSA response at 3 months, bPFS, metastasis-free survival, CaP-specific survival, OS, acute and long-term tolerance, QoL, and biopsy biomarkers.
Pelvic RT did not significantly improve cPFS on multivariable analysis. Secondary endpoints including MFS, CaP-specific survival, and OS are not reported in the source.
Effect estimate is from multivariable analysis; the 2×2 cabazitaxel randomization complicates attribution of the RT-volume effect. RT-attributable GU/GI toxicity by arm is not reported in source, which is the other half of the elective-nodal decision.
The investigators' own conclusion pivots from the RT question to the definition of "very high-risk": with <1 in 10 men dying of prostate cancer in the first decade, the population may be over-labeled. They call for biomarkers to guide intensification or de-intensification rather than uniform volume escalation.
Randomised, prespecified primary cPFS, mature 7yr readout, null result against a widely adopted practice. Design internally valid; the divergence is the headline.
In very high-risk localized N0M0 prostate cancer staged without PSMA PET, this questions routine whole-pelvis coverage over prostate-only RT with 3yr ADT; it does not speak to pts with PSMA-detected nodal disease, who were not enrolled.
- Does pelvic RT help when PSMA PET stages N0 more accurately? recruiting Extended vs. No Pelvic Lymph Node Dissection During Radical Prostatectomy. DISSECTION 2.0. Phase NAn=400 · primary completion 2027-02 · ePLND vs none in PSMA-PET node-negative high-riskn=250 · primary completion 2031-05 · randomises PORT vs whole-pelvis RT in PSMA-N0M0 pts
- RT-attributable late GU/GI toxicity by target volume n=700 · primary completion 2021-12 · longitudinal GU/GI/heme toxicity after WPRT, n=700n=400 · primary completion 2027-03 · late GI toxicity endpoint, whole-pelvis protons vs photons
- Biomarkers to select pts for treatment intensification vs de-intensification recruiting Treatment of High-Risk Prostate Cancer Guided by Novel Diagnostic Radio- and Molecular Tracers Phase 2/3n=493 · primary completion 2030-07 · tracer-guided darolutamide intensification + de-intens arm
📚 Sources · 🐦 1 tweet
📣@PBlanchardMD shows #ESTRO26 that pelvic #radiotherapy in high risk #prostatecancer does not have a large improve in outcomes.
— Shankar Siva (@_ShankarSiva) May 17, 2026
- With only 1 in 10 dying of prostate cancer in 10 years, are these patients truly “high risk”? #pcsm #radonc pic.twitter.com/D0XrGD6iNX
DBCG RT Natural
For≥60yr, pT1N0 unifocal non-lobular ER≥10% HER2-normal grade 1-2, margin ≥2mm
1.5% vs 9.8%
+RT 2/236 (0.3-5.1%) vs -RT 19/272 (5.9-14.9%)
TL;DR5yr invasive LR 1.5% with PBI vs 9.8% randomised no-PBI vs 8.2% self-selected no-PBI; RT+ET arm had zero events.
The RT read is the 2x2: +RT+ET was 0/105 events while -RT-ET hit 12.2%, and +RT-ET (3.0%) tracked -RT+ET (3.7%). PBI at 40Gy/15fr can therefore substitute for endocrine therapy in a woman who will not take or tolerate ET, rather than only supplement it.

| Study arm | Events/Total | CIF % (95% CI) |
|---|---|---|
| +RT | 2/236 | 1.5 (0.3-5.1%) |
| -RT | 19/272 | 9.8 (5.9-14.9%) |
| S-RT | 18/278 | 8.2 (4.5-13.3%) |
+2 more figures


10 details 4 trials watching
Phase III randomised Danish (DBCG) trial of PBI vs no PBI after breast conservation, stratified by institution and ET yes/no, with a third self-selecting no-PBI cohort. Planned 926 randomised, interim at 200 pts with 2yr f/u; median follow-up 4 years at this first report.
≥60 years, unilateral unifocal pT1N0 breast cancer, non-lobular, ER≥10%, HER2 normal, grade 1-2, limited DCIS, margin ≥2mm, treated with breast conservation. ET given per DBCG guideline (recommended for pT1c and/or grade 2).
Partial breast irradiation, 40Gy in 15 fractions. No whole-breast or nodal arm, so the result speaks to PBI specifically, not to omission of comprehensive breast RT.
Primary: 5-year invasive local recurrence, assumed 2% with an accepted maximum of 4%. Secondary: loco-regional side effects and QoL, neither reported in source.
All 41 recurrences were invasive, 36 isolated, and 39 of 41 occurred in pts without PBI. Distant failure was rare (4 events, 2 per group). The no-RT arms crossed the prespecified 4% threshold.
PRIME II and CALGB 9343 licensed RT omission in older low-risk pts on the strength of low absolute LR with ET, but both assumed ET adherence. Here the -RT -ET group reached 12.2%, which is the population omission actually creates when ET is declined or stopped.
Median f/u 4 years for a 5-year endpoint, and the trial was stopped early by the DMC, both of which favour an inflated effect estimate. The self-selecting no-PBI cohort is not randomised, and the 2x2 treatment-received analysis is not the randomised comparison. Toxicity and QoL, the secondary endpoints that would price the cost of PBI, are not in source.
The discussant framed it as RT or ET giving similar local control in low-risk pts, with surgery alone carrying high LR even here. That reframes the omission question from "can we drop RT" to "which single adjuvant modality, and what happens when the pt takes neither".
Randomised, prespecified LR endpoint, stopped early for excess recurrence without PBI. Directly contests RT omission in the ≥60yr low-risk group PRIME II / CALGB 9343 licensed.
In a woman ≥60 with pT1N0 grade 1-2 ER+ HER2-normal disease after breast conservation, this questions omitting PBI on PRIME II grounds, particularly where ET adherence is doubtful; it does not speak to lobular histology, ER<10%, or node-positive disease.
- Does the 1.5% LR hold at the full 5-year endpoint
- PBI toxicity and QoL vs endocrine therapy in this group n=168 · primary completion 2030-07 · 30 vs 26 Gy/5 fx APBI, 1° breast-related QoL
- Whether 5-fraction PBI reproduces this local control recruiting Accelerated Partial Breast Irradiation (APBI) Using Stereotactic Body Radiation Therapy (SBRT)n=200 · primary completion 2024-08 · 30 Gy/5 fx APBI registry, 5y f/u, n=200n=134 · primary completion 2029-08 · single-fx vs 5-fx APBI, 1° local controln=910 · primary completion 2029-11 · phase 3 5-fx PBI vs WBI, 1° LR non-inferiority
📚 Sources · 🐦 2 tweets
Another trial showing even for lR optimal local control with RT and ET and suboptimal adherence to ET. In era of 5 fraction decision making is easier # Estro2026 pic.twitter.com/nkvYl3iuTn
— Sushil (@Sushilberiwal) May 17, 2026
Danish #breastcancer partial breast #radiotherapy “natural” trial.
— Shankar Siva (@_ShankarSiva) May 17, 2026
➡️ No postoperative treatment had highest risk of recurrence
➡️either tamoxifen or #radonc reduced recurrence
➡️combined tamoxifen + RT had no recurrences
In context of EUROPA trial, RT has best QoL vs endocrine… pic.twitter.com/bDVmbDKRNb
EORTC IM-MS (22922/10925)
ForStage I-III breast cancer, incl. pN0, considering IM + medial supraclavicular RT
61.0% vs 61.8%
HR=1.00; 95% CI 0.90-1.10, P=0.967 (ns)
TL;DR20yr OS 61.0% vs 61.8%, HR 1.00 (0.90-1.10), P=0.967: early 15yr survival signal gone, BCM benefit offset by non-BCM deaths.
The mortality split is the RT read: BCM 18.6% vs 22.4% (HR 0.82) bought at a non-BCM cost of 20.4% vs 15.8% (HR 1.26), with cardiac disease 15.2% vs 11.7%. Since DBCG IMN2 heart doses ran 4-9× lower, the target-volume decision hinges on achievable MHD, not on abandoning IM coverage.

| Endpoint | IM-MS RT | No IM-MS RT | HR (95% CI) | P |
|---|---|---|---|---|
| BCM | 18.6% | 22.4% | 0.82; 0.72-0.95 | 0.006 |
| non-BCM | 20.4% | 15.8% | 1.26; 1.09-1.46 | 0.002 |
+3 more figures


| RT-related side effect | IM-MS RT | No IM-MS RT |
|---|---|---|
| Lung fibrosis | 6.3% | 3.2% |
| Cardiac fibrosis | 2.7% | 1.7% |
| Cardiac diseases | 15.2% | 11.7% |

| Endpoint (pN0) | IM-MS RT | No IM-MS RT | HR (95% CI) | P |
|---|---|---|---|---|
| DFS | 53.9% | 53.6% | 0.93; 0.81-1.07 | 0.318 |
| DMFS | 67.2% | 67.4% | 0.93; 0.78-1.10 | 0.397 |
8 details 5 trials watching
Randomised EORTC phase 3 (22922/10925), stage I-III breast cancer, ± internal mammary and medial supraclavicular irradiation. This is the 20-year ITT readout, presented as an ESTRO 2026 plenary, with a prespecified pN0 analysis.
The randomised question is target volume, not dose: adding IM-MS fields to standard breast/chest-wall treatment. Dose and fractionation are not reported in source. Mean heart dose is the operative technical variable, and the discussant contrasts it with DBCG IMN2 (MHD 1.2 Gy right-sided, 2.3 Gy left-sided, 4-9× lower than in this trial).
Primary: overall survival (ITT). Secondary reported here: DFS and DMFS (DATECAN definitions, so DFS includes all deaths and all breast events including DCIS and contralateral), breast-cancer mortality, non-breast-cancer mortality, second cancers, and late RT toxicity.
OS was flat at 20 years (HR=1.00, P=0.967), as were DFS 48.2% vs 49.0% (HR=0.97, P=0.515) and DMFS 58.9% vs 59.8% (HR=0.97, P=0.578). The signal sits in the competing-mortality split shown in the table above, not in any composite endpoint.
Cardiac disease 15.2% vs 11.7%, lung fibrosis 6.3% vs 3.2%, cardiac fibrosis 2.7% vs 1.7%. No statistical difference in second cancers or second breast cancers between arms, so the excess non-breast-cancer mortality tracks with cardiopulmonary late effects rather than second malignancy.
DBCG IMN2 (irradiation 2007-2014) reported reduced distant metastasis, reduced BCM and improved OS in node-positive pts at 15 years, with mean heart doses 4-9× lower than here. The two trials disagree on OS, and heart dose is the most plausible discriminator.
Toxicity and the competing-mortality penalty are technique-era dependent; RT dose, fractionation and delivery details are not reported in source. The pN0 analysis is a subgroup, though the null OS is the trial-level primary result.
The 15-year positive read did not hold to 20 years because non-breast-cancer deaths kept accruing. The clinical question shifts from whether IM-MS coverage works (it lowered BCM) to whether the heart dose it costs can be made small enough to let that benefit surface in OS.
Randomised, prespecified OS primary, 20y follow-up, now null after a positive 15y read. Divergence is internally valid; era-dependent heart dose is the caveat, not a design flaw.
In pN0 stage I-III breast cancer this does not support adding internal mammary and medial supraclavicular coverage (DFS HR 0.93, P=0.318); it does not settle the node-positive question, where modern low heart-dose technique still carries a 15-year benefit signal.
- Does IM-MS benefit survive at modern mean heart doses?
- Which node-positive subsets justify IM coverage? active Standard or Comprehensive Radiation Therapy in Treating Patients With Early-Stage Breast Cancer Previously Treated With Chemotherapy and Surgery Phase NAn=1636 · primary completion 2023-09 · randomised comprehensive nodal vs standard RT fieldsrecruiting RecurIndex Guided Avoidance of Regional Nodal Irradiation for Node Positive Breast Cancer Phase NAn=540 · primary completion 2029-08 · RecurIndex-gated RNI in clinically low-risk N1
- Do proton or DIBH techniques eliminate the non-BCM excess? recruiting Robustness Evaluation of Deep Inspiration Breath-Hold (DIBH) Plans in Internal Mammary Irradiationn=25 · primary completion 2026-12 · DIBH dose coverage + OAR params in IM irradiationn=220 · primary completion 2027-01 · proton locoregional RT, 10-15y cardiac mortality + SMNn=750 · primary completion 2027-12 · IMPT vs IMRT/VMAT, cardiac + lung toxicity endpoints
📚 Sources · 🐦 2 tweets
📌 Internal Mammary and Medial Supraclavicular irradiation in stage I-III breast cancer: 20 years results of the randomised EORTC trial 22922/10925, including in pNo patients
— Elisabetta Bonzano MD, PhD (@to_be_elizabeth) May 17, 2026
Special Joint Presentation Led by Prof. Philip Poortmans and Orit Kaidar-Person ✨ at #ESTRO26 @ESTRO_RT… pic.twitter.com/KIoJtdhEzp
20-year outcomes of @EORTC internal mammary #radiotherapy trial.
— Shankar Siva (@_ShankarSiva) May 17, 2026
➡️internal mammary improved control
➡️ survival counterbalanced by late adverse events #radiotherapy #bcsm
Great to see the long term data at #ESTRO26, and discussing Charlotte Cole suggests with modern RT, long… pic.twitter.com/yPtlfrLcri